Knee Dislocation: Epidemiology, Anatomy, and Initial Management
Key Takeaway
Knee dislocation (KD) is a severe, often limb-threatening injury involving tibiofemoral articulation disruption. Characterized by multi-ligamentous damage, it poses a high risk of neurovascular compromise. Initial management prioritizes limb salvage through prompt recognition, neurovascular assessment, and immediate reduction, addressing critical structures like the popliteal artery and common peroneal nerve.
Introduction & Epidemiology
Knee dislocation (KD) represents a severe, often limb-threatening, injury characterized by disruption of the tibiofemoral articulation. It is a complex injury involving multiple ligamentous structures, with a high propensity for associated neurovascular compromise. While often considered rare, the true incidence may be underestimated due to spontaneous reduction prior to medical evaluation. Reported incidence ranges from 0.02% to 0.17% of all orthopedic injuries, but this figure likely underrepresents the full spectrum given the frequency of emergency department reductions.
KDs are typically categorized by the mechanism of injury:
*
High-energy trauma:
Often associated with motor vehicle accidents (MVAs), falls from height, or athletic injuries, these usually present with gross deformity and higher rates of neurovascular injury.
*
Low-energy trauma:
Increasingly recognized, particularly in obese patients. These can occur with simple falls or twisting injuries, and may present with less obvious deformity, sometimes leading to missed or delayed diagnosis of the underlying instability and associated injuries.
The Schenck classification system, based on the direction of tibial displacement relative to the femur, is widely utilized:
*
KD I (Anterior):
Tibia anterior to femur. Most common, often due to hyperextension.
*
KD II (Posterior):
Tibia posterior to femur. Often due to direct blow to the proximal tibia with the knee flexed.
*
KD III (Medial/Lateral):
Tibia medial or lateral to femur. Result of varus or valgus stress.
*
KD IV (Rotatory):
Combination of displacements.
*
KD V (Irreducible):
Buttonholing of the femoral condyle through the joint capsule or interposition of soft tissues.
Further descriptors include:
*
Open vs. Closed:
Open dislocations carry a significantly higher risk of infection.
*
Associated Injuries:
Vascular injury (popliteal artery) is the most critical and time-sensitive complication, occurring in 10-50% of cases, with amputation rates rising sharply with delayed diagnosis (>8 hours). Neurologic injury (common peroneal nerve) is also common, affecting 20-40% of patients. Other associated injuries include meniscal tears, chondral lesions, and fractures.
Initial management prioritizes limb salvage through prompt recognition, neurovascular assessment, immediate reduction, and stabilization. The profound soft tissue disruption necessitates a structured, multidisciplinary approach involving orthopedic surgery, vascular surgery, and rehabilitation services.
Surgical Anatomy & Biomechanics
A thorough understanding of the knee's static and dynamic stabilizers is paramount for managing knee dislocations. The knee joint relies heavily on its ligamentous structures for stability, making it particularly vulnerable to multi-ligamentous injury during dislocation.
Static Stabilizers
The primary static stabilizers of the knee include:
*
Cruciate Ligaments:
*
Anterior Cruciate Ligament (ACL):
Resists anterior translation of the tibia relative to the femur and secondary valgus/varus and internal/external rotation. Typically tears with hyperextension or valgus/external rotation stress.
*
Posterior Cruciate Ligament (PCL):
Resists posterior translation of the tibia relative to the femur and internal rotation. Often tears with direct posterior force to the tibia or hyperflexion.
*
Collateral Ligaments:
*
Medial Collateral Ligament (MCL):
Primary restraint to valgus stress. Comprises superficial and deep layers.
*
Lateral Collateral Ligament (LCL):
Primary restraint to varus stress. Part of the posterolateral corner (PLC).
*
Posterolateral Corner (PLC):
A complex of structures crucial for varus and external rotation stability. Key components include:
* Fibular collateral ligament (FCL, often used interchangeably with LCL).
* Popliteus tendon.
* Popliteofibular ligament.
* Posterolateral joint capsule.
* Biceps femoris tendon (dynamic stabilizer, but its distal attachment integrates with PLC).
*
Posteromedial Corner (PMC):
Less commonly emphasized in KD classifications but contributes to valgus and internal rotation stability. Includes the superficial MCL, deep MCL (meniscofemoral and meniscotibial ligaments), posterior oblique ligament (POL), and semimembranosus tendon.
*
Joint Capsule:
Provides overall containment and is disrupted in all knee dislocations.
Dynamic Stabilizers
Muscles surrounding the knee contribute significantly to stability, particularly after ligamentous injury.
*
Quadriceps Femoris:
Extensors of the knee, anterior stabilizers.
*
Hamstrings:
Flexors of the knee, posterior stabilizers, and contribute to rotational stability.
*
Popliteus Muscle:
Internally rotates the tibia on the femur, unlocks the knee, and provides posterolateral stability.
*
Gastrocnemius:
Biarticular muscle, assists in knee flexion, and its heads contribute to posterior stability.
Neurovascular Structures
The intimate relationship of critical neurovascular structures to the knee joint makes them highly susceptible to injury during dislocation.
*
Popliteal Artery:
Located directly posterior to the knee joint, fixed proximally by the adductor hiatus and distally by the soleal arch. This tethering makes it highly prone to stretch or transection with significant tibiofemoral displacement. Assessment of popliteal artery integrity is the top priority.
*
Common Peroneal Nerve:
Wraps around the fibular neck, making it vulnerable to stretch or direct trauma, particularly with posterolateral corner injuries or valgus stress. Palsy can result in foot drop.
*
Tibial Nerve:
Less frequently injured than the common peroneal nerve dueing KD, located more medially and protected by musculature.
The typical pattern of ligament disruption in knee dislocations involves two or more primary stabilizers. For instance, an anterior dislocation (KD I) frequently involves ACL and PCL disruption, along with either the MCL or LCL/PLC, depending on the valgus/varus component. A posterior dislocation (KD II) classically involves PCL rupture, often with ACL and collateral ligament involvement.
Biomechanical studies emphasize the interdependence of knee ligaments. Injury to one ligament often overloads others, leading to progressive failure. Restoring the anatomical relationships and tensioning of these ligaments is critical for successful long-term outcomes and prevention of post-traumatic arthritis. The posterolateral corner is particularly challenging to manage, and its unrecognized or inadequately treated injury is a leading cause of persistent instability and reconstruction failure.
Indications & Contraindications
The management of knee dislocations is predominantly surgical, given the severe soft tissue disruption and high potential for long-term instability and functional deficits. Initial assessment, reduction, and neurovascular stabilization are acute priorities. The decision for definitive operative versus non-operative management is typically made after the acute limb-threatening issues are addressed and a comprehensive injury assessment (including MRI) is completed.
Indications for Operative Management
The vast majority of knee dislocations will require surgical intervention.
*
Vascular Compromise:
This is the most urgent indication. Any signs of vascular injury (absent pulses, diminished Ankle-Brachial Index (ABI < 0.9), expanding hematoma, cold limb, pulsatile bleeding) necessitate immediate surgical exploration and repair by a vascular surgeon.
*
Irreducible Dislocation:
Inability to achieve or maintain a closed reduction. This often indicates soft tissue interposition (e.g., meniscal bucket-handle tear, medial retinaculum, or medial femoral condyle "buttonholing" through the capsule), requiring open reduction.
*
Open Dislocation:
Requires immediate surgical debridement, copious irrigation, and stabilization to prevent infection and facilitate healing.
*
Gross Instability After Reduction:
If the knee remains grossly unstable after successful reduction, suggesting extensive ligamentous damage, operative stabilization is indicated to restore joint congruity and prevent recurrent dislocation.
*
Concomitant Bony Injuries Requiring Fixation:
Intra-articular fractures (e.g., tibial plateau, femoral condyle) or avulsion fractures (e.g., Segond fracture, arcuate complex avulsion) that contribute to instability or joint incongruity require surgical fixation.
*
Multi-Ligamentous Injuries:
While the timing of definitive ligament reconstruction can be debated (acute vs. staged), the presence of multi-ligamentous disruption in an otherwise healthy and active individual is a strong indication for surgical reconstruction to restore stability and function. This includes injuries to two or more of the major ligaments (ACL, PCL, MCL, LCL/PLC).
*
Meniscal Tears Causing Mechanical Symptoms:
Large, unstable meniscal tears (especially bucket-handle tears) that cause locking, catching, or impede full range of motion may require repair or debridement.
Indications for Non-Operative Management
Non-operative management is rare and typically reserved for very specific circumstances.
*
Stable, Reduced Dislocation with Isolated, Lower-Grade Ligamentous Injuries:
Extremely uncommon in true knee dislocations. This might apply to grade I/II MCL or LCL injuries in the context of an overall stable joint after reduction, but complete tears of two or more major ligaments constitute a dislocation.
*
Medically Unfit Patients:
Patients with severe comorbidities that contraindicate surgery, or those with very limited functional demands. In these cases, a hinged knee brace and protected weight-bearing for comfort and basic mobility may be chosen.
*
Delayed Presentation with Minimal Symptoms:
Very occasionally, a spontaneously reduced dislocation with mild residual symptoms and stable examination (often in elderly or sedentary individuals) might be managed non-operatively, though long-term instability and arthritis remain significant concerns.
Table 1: Operative vs. Non-Operative Indications for Knee Dislocation
| Indication Category | Operative Management | Non-Operative Management (Rare) |
|---|---|---|
| Acute Limb Threat | - Vascular injury (ABI < 0.9, absent pulses, ischemia) : Immediate exploration and repair. | - N/A (always operative for vascular compromise) |
| Dislocation Status | - Irreducible dislocation: Open reduction required. | - Spontaneously reduced and demonstrably stable knee without other high-grade ligamentous or associated injuries (extremely rare in true KD). |
| Knee Stability | - Gross instability after reduction: Requires surgical stabilization (external fixator, repair/reconstruction). | - Reduced knee with minimal residual instability (e.g., isolated Grade I/II collateral ligament injury without cruciate rupture, though this is not a true "dislocation"). Limited functional demands. |
| Associated Injuries | - Open dislocation: Immediate debridement and stabilization. | - N/A (open dislocations are surgical emergencies). |
| - Multi-ligamentous injuries (2+ major ligaments): Acute repair/reconstruction (timing debated, but definitive surgical management indicated). | - Isolated, low-grade ligament injuries (e.g., Grade I MCL/LCL strain) in a stable, reduced knee. | |
| - Significant intra-articular or avulsion fractures: Requiring ORIF for stability or joint congruity. | - Medically unfit patient for surgery, very low functional demand, or non-displaced stable fractures not contributing to instability. | |
| Patient Factors | - Young, active patient: High functional demands, desire to return to sport/activity. | - Elderly, sedentary patient with multiple comorbidities precluding surgery. Limited functional demands. |
| Other Mechanical Issues | - Meniscal tears causing mechanical locking/symptoms: Surgical repair or partial meniscectomy. | - Asymptomatic meniscal tears not causing mechanical symptoms and not contributing to instability (uncommon in KD). |
Pre-Operative Planning & Patient Positioning
Comprehensive pre-operative planning for knee dislocation management is critical due to the complex nature of the injury and potential for multi-system involvement.
Initial Assessment and Stabilization ("What to Do First")
- Primary Survey (ATLS Protocol): Rule out life-threatening injuries.
-
Neurovascular Assessment:
This is paramount.
- Pulses: Palpation of dorsalis pedis and posterior tibial pulses.
- Ankle-Brachial Index (ABI): Crucial screening tool. An ABI < 0.9 in an awake patient is highly suspicious for arterial injury and warrants further investigation (e.g., CT angiogram or immediate surgical exploration). In an obtunded patient, a single pulse check may be unreliable, and a CTA should be considered liberally.
- Neurological Exam: Document common peroneal nerve (foot dorsiflexion, toe extension, sensation to first web space) and tibial nerve (foot plantarflexion, toe flexion, sensation to sole of foot) function.
- Compartment Syndrome Check: Monitor for the "5 Ps" (pain, pallor, paresthesia, pulselessness, paralysis), particularly after reperfusion of an ischemic limb.
-
Emergency Reduction:
Prompt reduction of the dislocated knee is essential to minimize soft tissue tension and potentially restore blood flow to an ischemic limb.
- Technique: Gentle longitudinal traction with appropriate counter-traction. For anterior dislocations, apply posterior force to the tibia. For posterior dislocations, apply anterior force. May require sedation or conscious sedation.
- Post-Reduction Assessment: Re-evaluate neurovascular status immediately. Apply a well-padded splint (e.g., posterior slab with extension components) with the knee in 15-30 degrees of flexion to relax the popliteal artery and common peroneal nerve.
-
Imaging:
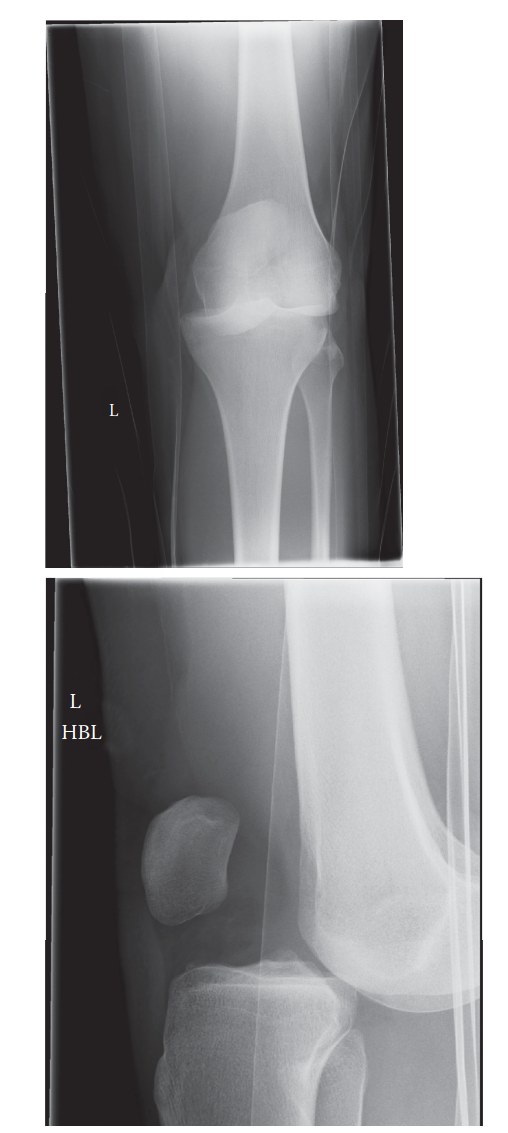
- Plain Radiographs: AP, lateral, and oblique views to confirm dislocation, assess reduction, and identify any associated fractures (tibial plateau, femoral condyle, fibular head avulsion).
- CT Angiogram (CTA): The gold standard for evaluating suspected popliteal artery injury if the ABI is abnormal or clinical suspicion is high. It can also assess bony anatomy.
- MRI: Performed after stabilization, often within the first 7-10 days (or acutely if limb is stable and patient is going to OR for vascular repair) to precisely delineate the extent of ligamentous, meniscal, and chondral injuries. This guides definitive surgical planning.
Pre-operative Planning for Definitive Surgery
-
Timing of Surgery:
- Immediate: Vascular repair, open dislocation, irreducible dislocation, compartment syndrome.
- Acute (within 1-3 weeks): Many surgeons prefer early ligament repair/reconstruction to capitalize on tissue healing potential and facilitate rehabilitation, provided soft tissue swelling has subsided.
- Staged/Delayed: Some prefer to defer definitive ligament reconstruction until swelling resolves, inflammatory phase settles, and ROM is recovered (typically 3-6 weeks post-injury) to reduce the risk of arthrofibrosis, especially in complex multi-ligament injuries. External fixation may be used acutely for stability, followed by staged reconstruction.
- Instrumentation and Implants: Pre-order all necessary grafts (autograft: hamstring, patellar tendon, quadriceps; allograft: Achilles, tibialis anterior, patellar tendon), hardware (interference screws, Endobuttons, suture anchors, staples), and external fixator components if anticipated.
- Graft Choice: Discuss with patient. Autografts are generally stronger but have donor site morbidity. Allografts avoid donor site morbidity but carry theoretical risks of disease transmission and immunological response, and may have slightly lower incorporation strength.
Patient Positioning
- Supine Position: The most common approach. The injured leg is typically placed on a leg holder or beach chair attachment allowing for full flexion and extension. A bump may be placed under the ipsilateral hip for better access to the medial side.
- Tourniquet: A pneumatic thigh tourniquet is routinely used for visualization and hemorrhage control during ligament reconstruction.
- Distal Leg Prep: The foot and ankle should remain sterilely draped to allow for assessment of foot movement and neurovascular status during the procedure, especially during trial reductions or graft tensioning.
- Fluoroscopy: Often utilized for confirmation of tunnel placement or hardware positioning.
Detailed Surgical Approach / Technique
The surgical management of knee dislocation involves a sequence of critical steps, prioritizing limb viability and then restoring stability. The specific technique varies based on the individual ligament injuries, surgeon preference, and available resources.
1. Initial Management and Vascular Intervention
- Emergency Reduction: As described in pre-operative planning, this is the first priority in the ED.
-
Vascular Exploration and Repair:
If a popliteal artery injury is confirmed or highly suspected (e.g., absent pulses, ABI < 0.9, expanding hematoma despite successful reduction), immediate vascular surgery consultation and exploration are mandated.
- Approach: Typically a medial approach to the popliteal fossa (medial gastrocnemius mobilization) provides good access to the artery. If the artery is anteriorly dislocated, a posterior approach may be needed.
- Procedure: Often involves temporary shunting to restore blood flow, followed by debridement of damaged vessel, and primary repair or interposition grafting (e.g., saphenous vein graft).
- Fasciotomy: Post-reperfusion fasciotomies of all four compartments of the lower leg are often necessary to prevent or treat compartment syndrome. This is a critical step to ensure limb salvage.
2. External Fixation (Optional)
- For grossly unstable knees, open dislocations, or patients with significant soft tissue swelling or other severe injuries, an external fixator may be applied initially to provide temporary stability.
- Technique: Usually involves two pins in the distal femur and two pins in the proximal tibia, connected by carbon fiber rods. The fixator can be static or hinged, allowing for controlled range of motion.
- Benefits: Provides stability, allows soft tissue swelling to subside, facilitates wound care in open injuries, and defers complex reconstruction until the patient is more stable.
- Disadvantages: Pin tract infection, stiffness, and patient inconvenience.
3. Ligamentous Reconstruction/Repair
The approach to definitive ligamentous stabilization depends on the pattern of injury. Acute repair (within 3 weeks) may be considered for collateral ligaments (MCL, LCL, PLC) or capsular avulsions. Cruciate ligament reconstruction (ACL, PCL) is often performed acutely or in a staged manner, typically with allograft due to the need for multiple grafts.
General Principles:
- Arthroscopy vs. Open: Cruciate reconstructions are often performed arthroscopically or arthroscopically-assisted. Collateral ligament repairs/reconstructions typically require open approaches.
- Graft Choice: Autografts (hamstring, patellar tendon, quadriceps tendon) offer biological healing but have donor site morbidity. Allografts (Achilles, tibialis anterior, patellar tendon) avoid donor site morbidity, are larger, and allow for multiple ligament reconstruction without additional incisions.
- Sequence: Typically, the PCL is addressed first as it is the primary posterior stabilizer, followed by the ACL, and then the collateral ligaments and PLC.
a. ACL Reconstruction
- Approach: Standard anteromedial and anterolateral portals.
-
Technique:
- Debridement: Remove remnants of the torn ACL.
- Tunnel Placement: Create femoral and tibial tunnels in anatomical locations, confirmed with fluoroscopy. Femoral tunnel typically transtibial, anteromedial portal, or outside-in technique. Tibial tunnel aims for the center of the ACL footprint.
-
Graft Passage and Fixation:
Pass the graft (e.g., quadruple hamstring, bone-patellar tendon-bone) through the tunnels. Fixation typically involves interference screws on both sides, or Endobuttons for femoral side and screw/post/staple on tibial side.
- Tensioning: Tension the graft at 15-30 degrees of knee flexion.
b. PCL Reconstruction
- Approach: Posteromedial portal or open posterior approach if significant PLC/PMC damage.
-
Technique (Tibial Inlay vs. Transtibial):
- Tibial Inlay: More technically demanding but avoids the "killer turn" of a transtibial tunnel. Involves a posterior incision, detaching the medial gastrocnemius, and creating a bone trough for the graft insertion.
- Transtibial: More common. Tibial tunnel created from anterior tibia to the posterior PCL footprint. Femoral tunnel created from an anterolateral approach to the medial femoral condyle.
- Graft: Allograft (Achilles or tibialis anterior) is frequently used due to size requirements.
- Fixation: Interference screws on both sides, or Endobuttons for femoral side and screw/washer for tibial side (transtibial).
- Tensioning: Tension at 90 degrees of knee flexion with an anterior drawer applied to neutralizes the posterior sag.
c. Medial Collateral Ligament (MCL) Repair/Reconstruction
- Approach: Medial longitudinal incision along the course of the MCL.
-
Technique:
- Grade III Tear: Acute repair (suture anchors, direct repair) if avulsed from femoral or tibial attachment, especially if proximal.
- Mid-substance Tear: May be repaired with sutures.
- Reconstruction: If severely comminuted or chronic, reconstruction using autograft (semitendinosus) or allograft. Graft passed under the sartorius fascia, fixed proximally to the medial femoral epicondyle and distally to the tibia.
- Posterior Oblique Ligament (POL): Often addressed if PMC instability is significant, by re-attaching or augmenting with part of the MCL repair.
d. Lateral Collateral Ligament (LCL) / Posterolateral Corner (PLC) Reconstruction
- Approach: Posterolateral incision, centered over the fibular head. Care must be taken to protect the common peroneal nerve which is identified and protected throughout.
-
Technique:
PLC injuries are complex and critical for stability. Common techniques aim to reconstruct the FCL, popliteofibular ligament, and popliteus tendon.
- LCL Reconstruction: Graft (e.g., autograft hamstring, allograft Achilles) from the lateral femoral epicondyle to the fibular head.
- Popliteus Reconstruction: Graft from the lateral femoral condyle (anterior and superior to the LCL attachment) to the popliteal hiatus on the tibia or directly to the popliteofibular ligament attachment on the fibular head.
- LaPrade Technique (Anatomical PLC Reconstruction): Reconstructs the FCL and popliteofibular ligament using two separate grafts. A fibular tunnel is drilled. One graft (FCL) passes from the lateral femoral epicondyle through the fibular head tunnel and back to the lateral femoral epicondyle. A second graft (popliteofibular ligament) passes from the popliteal sulcus on the lateral femoral condyle through the fibular head tunnel and attaches to the popliteal sulcus.
- Fixation: Interference screws, cortical buttons, or post fixation.
- Tensioning: LCL tensioned in 30 degrees of flexion and neutral rotation. Popliteofibular ligament tensioned in 70 degrees of flexion and neutral rotation. Over-tensioning can lead to stiffness.
4. Meniscal and Chondral Management
- Meniscal Repair/Debridement: Large, unstable meniscal tears (especially bucket-handle tears) found during arthroscopy should be repaired if possible (all-inside, inside-out, outside-in techniques). Irreparable tears or small tears not causing mechanical symptoms may be debrided.
- Chondral Lesions: Small, stable chondral lesions may be left alone. Larger, unstable lesions may require microfracture, debridement, or OATS procedure depending on size and location.
5. Wound Closure
- Meticulous hemostasis.
- Layered closure of fascia, subcutaneous tissue, and skin.
- Bulky compression dressing and application of a hinged knee brace locked in extension or slight flexion.
Complications & Management
Knee dislocations are associated with a high rate of complications, necessitating diligent post-operative monitoring and aggressive management strategies.
Common Complications
-
Vascular Injury:
The most devastating complication. Incidence 10-50%.
- Management: Immediate recognition is critical. Urgent surgical exploration and repair (shunting, primary repair, interposition graft). Post-repair monitoring for thrombosis and compartment syndrome.
- Salvage Strategies: Timely detection, appropriate surgical technique, post-operative anticoagulation, and aggressive fasciotomy when indicated. Amputation rate is high if diagnosis/treatment is delayed (>8 hours).
-
Neurological Injury (Common Peroneal Nerve Palsy):
Incidence 20-40%.
- Management: Usually a stretch injury (neurapraxia or axonotmesis). Often managed non-operatively with observation, physical therapy, and ankle-foot orthosis (AFO) to prevent foot drop. If nerve laceration is suspected (e.g., open injury), surgical exploration and repair/grafting may be indicated.
- Salvage Strategies: Early diagnosis, protection during surgery, patient education, AFO, potential nerve exploration/decompression if no recovery at 3-6 months.
-
Arthrofibrosis/Stiffness:
Incidence up to 50%, particularly in multi-ligament reconstructions.
- Management: Early, controlled range of motion (ROM) exercises post-operatively. Aggressive physical therapy. If conservative measures fail, arthroscopic lysis of adhesions or manipulation under anesthesia may be required.
- Salvage Strategies: Proactive rehabilitation, NSAIDs, early recognition and intervention (MUA, arthroscopic debridement).
-
Residual Instability/Re-dislocation:
Incidence 10-20%. Can be due to inadequate repair/reconstruction, missed injuries (especially PLC), or poor rehabilitation compliance.
- Management: Thorough clinical and imaging re-evaluation to identify the source of instability. Revision surgery may be required, often with more robust grafts or augmentation.
- Salvage Strategies: Comprehensive initial reconstruction, meticulous surgical technique, addressing all injured structures, prolonged bracing/protection, and revision surgery if indicated.
-
Infection:
Incidence 1-5%. Higher in open dislocations or prolonged surgeries.
- Management: Debridement, irrigation, antibiotics (IV and oral), implant removal if necessary.
- Salvage Strategies: Prophylactic antibiotics, meticulous aseptic technique, prompt surgical debridement and culture-directed antibiotics.
-
Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE):
Incidence 10-20% for DVT, 1-3% for PE. High risk due to prolonged immobilization, trauma-induced hypercoagulability.
- Management: Prophylactic anticoagulation (low molecular weight heparin or direct oral anticoagulants) is often recommended. If DVT/PE occurs, therapeutic anticoagulation.
- Salvage Strategies: Appropriate prophylaxis, early mobilization, surveillance if risk is very high.
-
Post-Traumatic Arthritis:
Long-term complication, nearly universal in severe injuries.
- Management: Symptomatic management (NSAIDs, activity modification, injections). Ultimately may require arthroplasty (total knee arthroplasty, TKA) in advanced cases.
- Salvage Strategies: Optimal anatomical reduction and stable fixation of all intra-articular injuries, meticulous reconstruction of ligaments, weight management.
-
Heterotopic Ossification (HO):
Incidence 5-20%. Bone formation in soft tissues around the joint.
- Management: Prophylactic NSAIDs (e.g., indomethacin) or radiation therapy in high-risk cases. Surgical excision if severe and causing mechanical impingement, but often recurs.
- Salvage Strategies: Prophylaxis, early ROM, surgical excision if functionally limiting.
Table 2: Common Complications, Incidence, and Salvage Strategies for Knee Dislocation
| Complication | Estimated Incidence | Management Strategy | Salvage Strategy / Notes |
|---|---|---|---|
| Vascular Injury | 10-50% | Immediate reduction, urgent CT angiogram if ABI < 0.9, immediate vascular surgical exploration and repair (shunt, primary repair, graft), fasciotomy. | Timely diagnosis (<8 hours), appropriate surgical technique, post-op anticoagulation. Amputation rate >50% if treatment delayed. |
| Common Peroneal Nerve Palsy | 20-40% | Observation, neurophysiology (EMG/NCS) at 3-6 weeks, AFO for foot drop. Surgical exploration/neurolysis/repair if laceration suspected or no recovery by 3-6 months. | Patient education, AFO, nerve exploration if indicated. Functional recovery is variable (30-60% achieve useful recovery). |
| Arthrofibrosis / Stiffness | Up to 50% | Early, controlled ROM (CPM), aggressive physical therapy. If persistent: arthroscopic lysis of adhesions, manipulation under anesthesia (MUA). | Proactive rehabilitation, NSAIDs, early recognition and intervention (MUA, arthroscopy). |
| Residual Instability | 10-20% | Thorough clinical and imaging (MRI) evaluation, often requiring revision ligament reconstruction (addressing missed or failed repairs/reconstructions, especially PLC). | Meticulous primary surgery, addressing all injured structures, extended bracing, revision surgery. |
| Infection (Surgical Site) | 1-5% (higher in open KD) | Prophylactic antibiotics, meticulous debridement and irrigation (for open KD), IV and oral antibiotics, surgical debridement, implant removal if persistent or deep. | Aseptic technique, prompt recognition, aggressive surgical debridement, culture-directed antibiotics. |
| DVT / Pulmonary Embolism | DVT: 10-20%; PE: 1-3% | Prophylactic anticoagulation (LMWH, DOACs) for 2-6 weeks. Therapeutic anticoagulation for confirmed DVT/PE. | Early mobilization, appropriate prophylaxis based on risk assessment. |
| Post-Traumatic Arthritis | High (nearly universal) | Symptomatic management (NSAIDs, activity modification, injections). Ultimately may require total knee arthroplasty (TKA) in severe cases. | Optimal anatomical reduction and stable fixation, meticulous ligament reconstruction, weight management, cartilage preservation strategies. |
| Heterotopic Ossification (HO) | 5-20% | Prophylactic NSAIDs (e.g., Indomethacin) or low-dose radiation in high-risk patients. Surgical excision if functionally limiting, but recurrence is common. | Prophylaxis in high-risk patients (e.g., head injury, burns), early ROM, surgical excision if severe and symptomatic after maturation of HO. |
| Hardware-related Issues | Variable | Removal of symptomatic hardware (prominent screws, anchors, external fixator pins). | Proper implant placement to minimize prominence. Early external fixator removal once stability is achieved. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following knee dislocation is a prolonged and critical process, often lasting 12-18 months. It is tailored to the specific ligaments reconstructed/repaired, the quality of fixation, and the patient's individual response to therapy. The overriding goals are to protect the repairs/reconstructions, restore range of motion, regain strength, and facilitate a safe return to functional activities. Communication between the surgeon, physical therapist, and patient is paramount.
General Principles
- Protection: Grafts require significant time to heal and incorporate. Protection from excessive stress (especially shear forces) is essential.
- Controlled Motion: Early, controlled range of motion is crucial to prevent arthrofibrosis, promote cartilage health, and facilitate graft healing by stimulating synovial fluid production.
- Progressive Loading: Gradual increase in weight-bearing and strengthening exercises as healing progresses.
- Neuromuscular Control: Emphasis on proprioception, balance, and dynamic stability.
Phase 1: Maximum Protection (Weeks 0-6)
- Goals: Protect repairs, control pain and swelling, achieve early controlled ROM.
- Bracing: Hinged knee brace locked in full extension or slight flexion (0-30 degrees) for walking, and unlocked for passive ROM exercises. The brace is typically worn at all times, including sleep, for the initial weeks.
- Weight Bearing: Non-weight-bearing (NWB) or touch-down weight-bearing (TDWB) with crutches. Progression to partial weight-bearing (PWB) is gradual and surgeon-dependent, often starting at 4-6 weeks for cruciate reconstructions. For PLC reconstructions, NWB/TDWB may be extended to 6-8 weeks due to the critical nature of these repairs.
-
Range of Motion (ROM):
- Cruciate Ligaments (ACL/PCL): Gentle passive ROM (PROM) 0-90 degrees, gradually progressing. Prone hangs for extension.
- PCL Specific: Avoid isolated hamstring strengthening and excessive knee flexion (>90 degrees) during the initial weeks to protect the posterior graft. No active knee flexion beyond 45 degrees.
- Collateral Ligaments (MCL/LCL/PLC): Limit varus/valgus stress. Gentle PROM within comfortable limits.
-
Exercises:
- Quadriceps sets, gluteal sets, ankle pumps.
- Gentle hamstring sets (avoiding isolated active knee flexion for PCL).
- Straight leg raises (SLR) in supine with knee braced.
- Cryotherapy and elevation for swelling.
Phase 2: Moderate Protection (Weeks 6-12)
- Goals: Restore full ROM (or near full), improve quadriceps and hamstring strength, wean from crutches.
- Bracing: Continue hinged brace for protection during ambulation, may be unlocked for activities. Often continued for 3-4 months.
- Weight Bearing: Progress from PWB to full weight-bearing (FWB) as tolerated, gradually weaning from crutches.
- ROM: Achieve full extension and flexion to 120-130 degrees or full within pain limits.
-
Exercises:
- Closed-chain exercises: Mini-squats (0-45 degrees), leg press (controlled ROM), wall slides.
- Open-chain exercises: Knee extension (avoiding terminal extension for ACL), hamstring curls (controlled).
- Proprioception: Balance activities (single leg stance with brace), wobble board.
- Stationary cycling (light resistance).
- Gait training emphasizing normalized mechanics.
Phase 3: Strength and Neuromuscular Control (Weeks 12-24)
- Goals: Maximize strength, power, and endurance; develop dynamic stability; prepare for sport-specific activities.
- Bracing: May discontinue brace for daily activities, continue for higher-risk activities or until return to sport.
-
Exercises:
- Progressive resistive exercises: Leg press, squats, step-ups, lunges.
- Plyometric training (light hopping, jumping) in controlled environments.
- Agility drills (shuttle runs, cutting) with increasing intensity.
- Sport-specific drills (non-contact).
- Advanced balance and proprioception.
- Cardiovascular conditioning (running on treadmill, elliptical).
Phase 4: Return to Sport / Activity (Months 6-12+)
- Goals: Safe return to previous level of activity or sport.
-
Criteria for Return to Sport:
- Full, pain-free ROM.
- No effusion.
- Isokinetic strength testing: Quadriceps and hamstring strength 90-100% of contralateral limb.
- Functional testing: Hop tests (single, triple, crossover) >90% of contralateral limb.
- Excellent dynamic stability and neuromuscular control.
- Passing sport-specific agility and cutting drills.
- Psychological readiness.
- Exercises: Full return to sport-specific training. Gradual progression to contact sports.
- Bracing: May wear a functional brace for high-risk sports, though evidence for its efficacy in preventing re-injury is mixed.
Special Considerations for Multi-Ligament Injuries
- More Conservative Progression: Rehabilitation is often slower and more protected than for isolated ACL injuries.
- External Fixation: If used, ROM may be delayed until fixator removal, or a hinged fixator may allow controlled motion.
- PCL Reconstruction: Requires careful protection against posterior tibial sag, limiting deep flexion and hamstring strengthening initially.
- PLC Reconstruction: Avoid varus stress and excessive internal rotation. Protect against forces that could stress the posterolateral repairs.
- Patient Education: Emphasize the importance of adherence to the protocol and the long timeline for recovery.
Summary of Key Literature / Guidelines
The management of knee dislocations is continually evolving, with key literature emphasizing prompt diagnosis, comprehensive assessment, and individualized treatment strategies.
1. Vascular Assessment
- Ankle-Brachial Index (ABI): The most critical initial screening tool. A widely cited threshold of ABI < 0.9 is highly predictive of arterial injury and necessitates further investigation, typically with a CT angiogram. Some literature supports that if the ABI is normal (>0.9) and the physical examination is completely benign (no hard or soft signs of vascular injury) in an awake, reliable patient, immediate CTA may be deferred, with serial clinical examinations (every 1-2 hours for 24-48 hours) as an alternative. However, a low threshold for CTA in multi-ligament knee injuries is generally recommended to avoid missed injuries.
- "Hard Signs" of Vascular Injury: Absent or diminished pulses, expanding hematoma, pulsatile bleeding, palpable thrill, audible bruit, limb ischemia (pain, pallor, paresthesia, pulselessness, paralysis). These necessitate immediate surgical exploration.
2. Imaging
- Plain Radiographs: Essential to confirm dislocation, assess reduction, and identify fractures.
- CT Angiogram (CTA): Gold standard for vascular evaluation when suspected.
- MRI: Universally accepted as critical for defining the extent of ligamentous, meniscal, and chondral injuries, guiding definitive surgical planning. Typically performed after reduction and stabilization of any vascular injury. The presence of a medial meniscal bucket-handle tear or interposition of soft tissues on MRI may indicate an irreducible dislocation.
3. Timing of Ligament Reconstruction
-
Acute (within 3 weeks) vs. Staged/Delayed (3-6 weeks or later):
This remains a subject of debate in the literature.
- Arguments for Acute: May facilitate easier identification of anatomical landmarks, primary repair of avulsed structures, better tissue quality for repair, and theoretically better functional outcomes by preventing chronic instability.
- Arguments for Staged/Delayed: Allows resolution of soft tissue swelling, improved range of motion, and reduced risk of arthrofibrosis, especially in complex multi-ligament injuries. Some advocate for initial external fixation to restore stability acutely, followed by staged ligament reconstruction.
- Current Consensus: The trend leans towards early surgical intervention for ligamentous reconstruction (within 1-3 weeks) once swelling has subsided and the knee has achieved a relatively quiescent state. However, the decision is individualized based on patient factors, injury pattern, and surgeon experience. Vascular injuries, open dislocations, and irreducible dislocations always warrant immediate surgical attention.
4. External Fixation
- Role: Increasingly used, especially in high-energy trauma, open dislocations, or when definitive reconstruction is delayed. Provides temporary stability, allows soft tissue healing, and facilitates subsequent reconstruction.
- Benefits: Reduces pain, prevents further joint damage, and assists in achieving acceptable ROM prior to definitive reconstruction.
- Considerations: Pin tract infections, potential for stiffness if maintained for prolonged periods.
5. Ligament Reconstruction Principles
- Anatomical Reconstruction: Emphasized for all major ligaments (ACL, PCL, MCL, LCL, PLC) to restore normal knee kinematics and improve long-term outcomes.
- Posterolateral Corner (PLC): Recognition and meticulous anatomical reconstruction of the PLC is paramount, as untreated or inadequately treated PLC injuries are a major cause of persistent instability and failure of cruciate ligament reconstructions. Techniques like the LaPrade reconstruction are widely cited for their anatomical fidelity.
- Allograft vs. Autograft: Allografts are frequently utilized in multi-ligament knee injuries due to the need for multiple grafts and avoidance of donor site morbidity. While some studies suggest slightly inferior outcomes with allografts compared to autografts in isolated ACL reconstruction, outcomes in multi-ligament settings are often comparable due to the technical demands and extensive tissue needs.
- Graft Tensioning: Proper tensioning of each reconstructed ligament is critical to avoid over-tensioning (leading to stiffness) or under-tensioning (leading to instability). Specific tensioning protocols for ACL (15-30° flexion), PCL (90° flexion with anterior drawer), and collaterals are crucial.
6. Rehabilitation
- Early Motion: Critical for preventing arthrofibrosis and promoting cartilage health.
- Protected Weight-Bearing: Gradual progression based on the stability of repairs and individual patient tolerance.
- Progressive Strengthening and Neuromuscular Control: Essential for restoring function and preventing re-injury.
- Prolonged Recovery: Patients must be counseled on the 12-18 month recovery period and the importance of adherence to rehabilitation protocols.
Key Guidelines and Consensus Statements
Various orthopedic societies (e.g., AAOS, ISAKOS) regularly publish guidelines and consensus statements that inform the evidence-based management of knee dislocations, emphasizing a systematic approach to diagnosis, vascular assessment, surgical planning, and rehabilitation. The overarching goal is limb salvage and restoration of long-term functional stability, acknowledging the high complexity and potential for complications inherent in these severe injuries.
You Might Also Like