Impaction Bone Grafting for Defects: Achieve Optimal R-TKA Results

Key Takeaway
Discover the latest medical recommendations for Impaction Bone Grafting for Defects: Achieve Optimal R-TKA Results. Grafting for defects, specifically impaction bone grafting, is indicated for contained femoral and proximal tibial metaphyseal and epiphyseal defects. It is also used for uncontained proximal tibial and distal femoral defects in combination with wire mesh, serving as a crucial reconstructive option in complex revision total knee arthroplasties.
Introduction & Epidemiology
Revision total knee arthroplasty (R-TKA) for aseptic loosening or periprosthetic joint infection (PJI) frequently involves significant bone loss in the distal femur and proximal tibia. The management of these bone defects presents a considerable reconstructive challenge, directly impacting component stability, limb alignment, and long-term implant survivorship. Impaction bone grafting (IBG) has emerged as a well-established biological reconstructive technique, aiming to restore lost bone stock, provide a stable foundation for the new prosthesis, and facilitate biological incorporation.
The prevalence of bone defects in R-TKA varies depending on the indication for revision, but estimates suggest that up to 70% of revision cases involve some degree of bone loss, with 20-30% classified as severe (Anderson Orthopaedic Research Institute, AORI, Type 2 or 3). IBG, popularized in hip revision surgery, has been adapted for knee revisions, offering a biological alternative to structural allografts, metallic augments, or metaphyseal cones and sleeves. The fundamental principle involves compacting cancellous bone graft into the defect to create a mechanically stable bed that subsequently undergoes creeping substitution and biological integration. The ultimate goal is to achieve a durable, osseointegrated construct, particularly beneficial in younger or more active patients where the longevity of the revision is paramount.
Surgical Anatomy & Biomechanics
Effective utilization of impaction bone grafting in R-TKA necessitates a comprehensive understanding of the surgical anatomy of the distal femur and proximal tibia, along with the biomechanical principles governing graft behavior and host response.
The distal femur consists of the medial and lateral condyles, the intercondylar notch, and the metaphyseal flare. Defects commonly occur in the posterior condyles, the distal articular surface, and within the metaphysis, often due to osteolysis around a loose femoral component. The cortical shell provides critical support, while the cancellous bone within the metaphysis is crucial for primary stability and biological integration.
The proximal tibia comprises the medial and lateral tibial plateaus, the intercondylar eminence, and the proximal metaphysis. Defects are frequently encountered beneath the tibial tray, particularly in the medial plateau, or involve significant metaphyseal bone loss. The tibial cortex, particularly the anterior and medial aspects, plays a key role in containing defects and providing structural integrity. Understanding the bony contours and the vascular supply to these regions is essential for optimizing graft healing and minimizing complications.
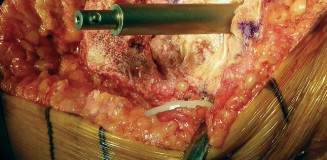
Figure 1: Illustration depicting typical locations and morphologies of bone defects encountered in the distal femur and proximal tibia during revision total knee arthroplasty.
Biomechanics of Impaction Bone Grafting:
The core biomechanical principle of IBG relies on the controlled impaction of cancellous bone chips to achieve a high packing density. This compaction serves several critical functions:
1.
Mechanical Stability:
A densely packed graft creates a stable, load-bearing construct capable of resisting forces applied by the prosthesis. Studies have shown that appropriately impacted cancellous graft can achieve compressive strengths comparable to cancellous bone, albeit lower than cortical bone.
2.
Biological Environment:
The impaction process reduces the inter-particle distance, facilitating revascularization and osteoconduction. The high density allows for direct contact between graft particles and the host bone, promoting creeping substitution and eventual remodeling into viable bone.
3.
Stress Shielding Prevention:
Unlike large structural allografts or rigid metallic augments, a biologically integrated impaction graft aims for load sharing with the surrounding host bone, potentially reducing stress shielding and promoting long-term host bone health.
4.
Containment:
For successful impaction, the defect must be contained, either by existing host bone or by reconstructive techniques such as wire mesh. Containment prevents graft dispersal and allows for the buildup of sufficient pressure during impaction to achieve high density. Without adequate containment, the graft cannot be effectively compacted, leading to instability and potential failure.
The immediate mechanical stability provided by IBG is generally lower than that achieved with structural allografts or metallic augments, necessitating a period of protected weight-bearing to allow for biological incorporation and maturation of the graft. This biological healing process involves osteoclastic resorption of necrotic graft bone and simultaneous osteoblastic deposition of new, living bone. The extent and speed of this process are influenced by factors such as graft quality, host bone vascularity, patient comorbidities, and the mechanical environment.
Indications & Contraindications
Impaction bone grafting is a powerful tool in the reconstructive armamentarium for R-TKA, but its judicious application is critical. Patient selection and careful defect characterization are paramount to achieving successful outcomes.
Indications for Impaction Bone Grafting
- Contained Femoral Metaphyseal and Epiphyseal Defects: AORI Type 1 and Type 2A defects on the femoral side are ideal. These defects typically involve cancellous bone loss without significant cortical compromise, allowing for inherent containment.
- Contained Proximal Tibial Metaphyseal and Epiphyseal Defects: Similarly, AORI Type 1 and Type 2A defects in the proximal tibia are well-suited for IBG, particularly those involving subsidence of the tibial tray or localized osteolysis.
-
Uncontained Proximal Tibial and Distal Femoral Defects (AORI Type 2B, Type 3):
In these more extensive defects involving cortical loss, IBG can still be utilized, but requires adjunctive containment strategies.
- Wire Mesh: The use of wire mesh (e.g., titanium or stainless steel mesh) is a classic technique to create a biological "basket" for the graft. While effective, as noted, it "is difficult and time consuming, and other reconstructive options may be more suitable." However, in cases prioritizing biological reconstruction, it remains a viable option.
- Cement Mantle/Restrictors: In some uncontained defects, a peripheral cement mantle or specialized cement restrictors can provide temporary containment.
- Trabecular Metal Cones/Sleeves (Hybrid Approach): In cases of severe metaphyseal bone loss (AORI Type 2B or 3), a hybrid approach combining IBG to fill the smaller epiphyseal defects with a metaphyseal cone or sleeve to provide robust structural support and containment for the graft can be highly effective. The cone/sleeve acts as a scaffold into which the graft can be impacted, offering both immediate stability and a biological reconstruction option.
- Defects from Aseptic Loosening or Osteolysis: IBG is particularly effective in restoring bone stock lost due to chronic aseptic loosening or extensive osteolysis secondary to polyethylene wear.
- Defects Following PJI Eradication: Once an infection has been successfully eradicated, IBG can be considered for reconstruction of remaining bone defects, provided there is no active inflammatory process.
- Desire for Biological Reconstruction: In younger or more active patients, IBG offers the advantage of restoring native bone stock, potentially leading to a more durable implant fixation and allowing for easier future revisions if required.
Controversies & Relative Contraindications
- Extensive Uncontained Defects (AORI Type 3): While IBG with mesh can be attempted, for very large, globally uncontained defects, especially in older, less active patients, alternative methods providing immediate mechanical stability, such as bulk allografts, metallic augments, or metaphyseal cones/sleeves, may be preferred.
- Active Infection: Absolute contraindication. IBG should only be performed after complete eradication of infection.
- Poor Host Bone Quality: Patients with severe osteoporosis or other conditions leading to extremely poor host bone quality may not provide a suitable environment for graft incorporation, potentially leading to graft collapse or non-union.
- Inability to Adhere to Post-operative Weight-Bearing Restrictions: IBG typically requires a period of protected weight-bearing (often 6-12 weeks) to allow for graft incorporation. Patients who cannot comply with these restrictions may be better suited for options providing immediate full weight-bearing.
- Rapidly Progressive Disease: In cases of aggressive tumor or rapidly progressive osteolysis where the underlying pathology cannot be controlled, IBG may not be appropriate.
Operative vs. Alternative Reconstructive Strategies for Bone Defects in R-TKA
| Feature/Consideration | Impaction Bone Grafting (IBG) | Structural Allografts (e.g., femoral head/condyle) | Metallic Augments (blocks, wedges) | Metaphyseal Cones/Sleeves (e.g., Trabecular Metal, Porous Titanium) |
|---|---|---|---|---|
| Primary Goal | Biological restoration of bone stock, long-term incorporation | Immediate structural support, bone stock restoration, load transfer | Immediate mechanical support, gap filling, load transfer | Immediate structural support, biological ingrowth potential, stable metaphyseal fixation, defect containment |
| Bone Loss Type | AORI Type 1, 2A (contained); Type 2B, 3 (with containment, e.g., mesh) | AORI Type 2B, 3 (large, uncontained defects) | AORI Type 2A, 2B, 3 (focal defects, contained or uncontained) | AORI Type 2B, 3 (significant metaphyseal loss, contained or uncontained) |
| Immediate Stability | Moderate (requires meticulous impaction); typically needs protected weight-bearing | High (provides robust structural support) | High (provides robust structural support) | High (provides robust metaphyseal fixation and stability) |
| Biological Potential | Excellent (creeping substitution, eventual remodeling into host bone) | Good (biological incorporation over time, but often slower and less complete than IBG) | None (inert material) | Excellent (porous structure allows for bone ingrowth, biological fixation) |
| Graft Material | Morcellized cancellous allograft (preferred), autograft (limited) | Cortical-cancellous bone from femoral head/condyle | Cobalt-chromium, titanium alloys | Tantalum, titanium alloys with highly porous structures |
| Surgical Complexity | Moderate to high (meticulous impaction, containment often needed) | High (precise sizing, contouring, fixation) | Moderate (proper sizing and fixation) | High (precise sizing, reaming, impaction for press-fit) |
| Post-op Weight-Bearing | Protected weight-bearing (6-12 weeks) is typically recommended for optimal graft incorporation | Often allows earlier weight-bearing | Allows immediate weight-bearing | Often allows earlier or immediate weight-bearing due to press-fit stability |
| Complications | Non-union, graft resorption, infection, component subsidence | Non-union, fracture, infection, graft collapse, slow incorporation | Aseptic loosening, stress shielding, infection | Subsidence, aseptic loosening, fracture (rare), infection |
| Cost | Moderate (allograft processing, specialized instrumentation) | High (allograft procurement, specialized preparation) | Moderate to high (implant cost) | High (specialized implant cost) |
| Revision Potential | Excellent (restored bone stock facilitates future revisions) | Good (may present challenges if revised due to fibrous ingrowth or non-union) | Good (removal can be straightforward, but may leave large defect) | Good (can be removed, but bone ingrowth may complicate removal) |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful impaction bone grafting in R-TKA. This phase dictates the approach, graft requirements, implant selection, and potential intra-operative challenges.
Pre-Operative Planning
-
Clinical Evaluation:
- Thorough history regarding previous surgeries, complications (especially infection), pain characteristics, and functional limitations.
- Assessment of comorbidities, nutritional status, and overall patient health to optimize for surgery.
- Evaluation of skin integrity, range of motion, and ligamentous stability.
- Pre-operative aspiration and synovial fluid analysis (cell count, differential, culture) are mandatory for any suspected infection.
-
Imaging Assessment:
-
Standard Radiographs:
Standing anteroposterior (AP), lateral, and patellar sunrise views of the affected knee. These views are crucial for initial assessment of component position, alignment, signs of loosening (e.g., lucencies, subsidence), and obvious bone defects.
-
In Figure 2, anteroposterior (Fig. 2A) and lateral (Fig. 2B) radiographs show a failed revision total knee arthroplasty with subsidence of the tibial component, polyethylene wear, and osteolysis beneath the tibial tray and posterior femur.

Figure 2: Pre-operative radiographs (A: AP, B: Lateral) demonstrating significant tibial component subsidence, polyethylene wear, and associated osteolytic bone loss in a failed revision TKA.
-
In Figure 2, anteroposterior (Fig. 2A) and lateral (Fig. 2B) radiographs show a failed revision total knee arthroplasty with subsidence of the tibial component, polyethylene wear, and osteolysis beneath the tibial tray and posterior femur.
- Long-Leg Standing Radiographs: Essential for assessing overall limb alignment and planning for correction.
-
Computed Tomography (CT) Scan:
The most valuable imaging modality for precise characterization of bone defects. It allows for:
- Accurate measurement of defect volume and dimensions.
- Identification of cortical breaches and evaluation of defect containment (AORI classification).
- Assessment of remaining host bone stock quality.
-
3D reconstruction provides an invaluable roadmap for surgical strategy.

Figure 3: Coronal CT image illustrating a significant metaphyseal bone defect in the proximal tibia, characterized by cortical erosion and loss of cancellous bone.
- Magnetic Resonance Imaging (MRI): Less commonly used specifically for bone defect assessment in R-TKA, but may be useful if soft tissue pathology or occult infection (though less accurate than aspiration) is suspected.
- Nuclear Medicine Scans (Bone Scintigraphy, PET Scan): May aid in differentiating aseptic loosening from infection, especially in cases with equivocal aspiration results.
-
Standard Radiographs:
Standing anteroposterior (AP), lateral, and patellar sunrise views of the affected knee. These views are crucial for initial assessment of component position, alignment, signs of loosening (e.g., lucencies, subsidence), and obvious bone defects.
-
Templating:
- Utilize pre-operative radiographs and CT images for templating the planned revision components (femoral, tibial, patellar).
- Estimate the size and volume of bone graft required.
- Plan for appropriate sizing of metaphyseal augments, stems, or specialized cones/sleeves if a hybrid approach is considered.
- Plan for any necessary defect containment devices (e.g., wire mesh).
-
Allograft Ordering:
- Confirm availability of appropriate cancellous morcellized allograft (freeze-dried or fresh-frozen). Often 200-400cc of graft is required for moderate to large defects.
- Autograft is rarely sufficient due to limited quantities.
-
Instrumentation:
- Ensure availability of specialized impaction grafting instruments, including various sizes of impactors, tampers, and graft delivery systems.
- Have wire mesh (e.g., titanium or stainless steel), screws, and wire-tightening devices available for uncontained defects.
- Specific revision TKA instrumentation for component removal and re-implantation.
Patient Positioning
- Supine Position: The patient is typically positioned supine on the operating table.
- Leg Preparation: The affected leg is prepared and draped in a sterile fashion, allowing for full range of motion, particularly flexion, which is crucial for adequate exposure.
- Tourniquet Application: A pneumatic tourniquet is routinely applied to the proximal thigh to ensure a bloodless field, which is critical for clear visualization and effective bone graft impaction.
- Leg Holder: A knee positioner or leg holder may be used to provide stable support and facilitate controlled flexion and extension during the procedure. Careful padding of pressure points is essential to prevent neurovascular complications.
Detailed Surgical Approach / Technique
The execution of impaction bone grafting demands precision, patience, and adherence to specific technical principles to ensure optimal graft density and biological integration.
Incision and Exposure
- Standard Medial Parapatellar Approach: This is the most common approach for R-TKA. The previous incision is typically re-entered. If skin viability is compromised, a different incision may be necessary (e.g., lateral parapatellar, quadriceps snip, or V-Y quadriceps plasty for severe stiffness).
- Component Removal: Meticulous removal of existing femoral, tibial, and patellar components. Care must be taken to minimize further bone loss during this stage. Cement removal tools, osteotomes, and specialized extraction devices are employed.
- Debridement: All fibrous tissue, granulomatous material, residual cement, and necrotic bone are meticulously debrided to expose a bed of healthy, bleeding bone at the periphery of the defect. This is critical for encouraging host bone ingrowth and graft incorporation.
Defect Assessment and Preparation
- Defect Classification: Re-assess the bone defect intra-operatively and classify it using the AORI system (Type 1, 2A, 2B, 3) to guide the reconstructive strategy.
-
Defect Creation/Containment:
- For contained defects, simply debride to healthy margins.
-
For uncontained defects, the primary goal is to create a contained space where the graft can be impacted.
-
Wire Mesh (as per seed content):
For femoral defects, a pre-contoured wire mesh (titanium or stainless steel) can be used to reconstruct the lost cortical wall. The mesh is shaped to the defect, providing a basket for the morcellized graft. It is secured with small screws or sutures to the surrounding host bone. This technique can be challenging and time-consuming but offers a biological solution.

Figure 4: Intraoperative image demonstrating the placement of a wire mesh to contain an uncontained femoral condylar defect, creating a "basket" for subsequent impaction grafting. - Tibial Defects: Similar wire mesh techniques can be applied for large peripheral tibial defects. Cement restrictors or specialized revision components with augmented flanges can also assist in containment.
- Hybrid Approach: In significant metaphyseal defects (AORI 2B or 3), a metaphyseal cone or sleeve can be press-fit into the reamed canal, providing immediate structural support and creating a contained chamber within which to perform impaction grafting for the more superficial defects.
-
Wire Mesh (as per seed content):
For femoral defects, a pre-contoured wire mesh (titanium or stainless steel) can be used to reconstruct the lost cortical wall. The mesh is shaped to the defect, providing a basket for the morcellized graft. It is secured with small screws or sutures to the surrounding host bone. This technique can be challenging and time-consuming but offers a biological solution.
Graft Preparation
- Morcellized Cancellous Allograft: This is the preferred graft material. It should be thawed according to protocol. The graft chips should be approximately 3-5mm in size, ensuring they can be effectively impacted and revascularized. Autograft may be harvested from the reamed intramedullary canal but is usually insufficient in quantity.
- Antibiotic Soaking (Optional): Some surgeons advocate soaking the allograft in a dilute antibiotic solution (e.g., vancomycin) for a specified period to minimize infection risk, though evidence for its routine use with sterile allograft is not universally strong.
Graft Impaction
-
Layer-by-Layer Impaction:
The cancellous allograft is introduced into the defect in small, sequential layers. Each layer is meticulously compacted using specialized impaction instruments (impactors and tampers) of various sizes and shapes. The goal is to achieve maximal packing density.
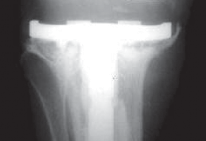
Figure 5: Schematic diagram illustrating the layer-by-layer impaction technique for bone graft within a contained defect, demonstrating the progressive increase in graft density. - Centripetal Compaction: Compaction should proceed from the periphery of the defect towards the center, ensuring uniform density and maximizing graft-host bone contact.
- Achieving High Density: The impaction process continues until the graft feels hard and resilient, similar to cortical bone. A firm, stable bed is essential for the primary stability of the prosthesis. The sound of impaction should transition from dull to a higher pitch as density increases.
-
Sculpting the Graft Bed:
The impacted graft is then sculpted and reamed to conform precisely to the contours of the revision prosthesis, creating a stable platform for the new components. Trial components are used to confirm proper fit and fill.

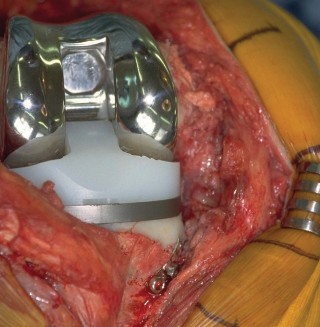
Figure 6: Intraoperative image showing the appearance of a densely impacted tibial metaphyseal defect, prepared to receive the new tibial tray.
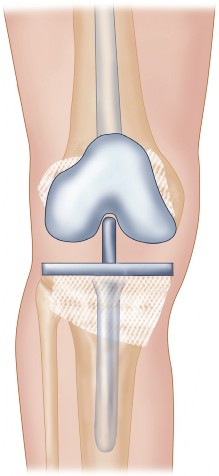
Figure 7: A different view of an impacted tibial defect, demonstrating the smooth, contoured surface ready for component implantation.
Prosthetic Implantation
- Component Selection: Revision TKA components, often with intramedullary stems for enhanced stability and load transfer, are typically used. The stems can be cemented or cementless, depending on surgeon preference and host bone quality.
- Cementing Technique (if used): If cemented components are used, particular attention must be paid to cementation technique on the graft bed. Adequate pressurization of cement into the densely impacted graft and host bone is crucial for robust fixation.
- Stem Fixation: Stems can be cemented into the intramedullary canal or utilize a press-fit technique, depending on the stem design and surgeon preference.
-
Final Seating:
The final components are seated firmly, ensuring proper alignment, rotation, and stability.
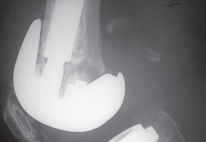
Figure 8: Post-implantation radiograph showing a well-fixed revision femoral component with a stem, following impaction bone grafting of distal femoral defects.

Figure 9: Post-implantation radiograph demonstrating a revised tibial component securely fixed after impaction bone grafting, showing good fill of the metaphyseal defect.

Figure 10: Lateral radiograph showcasing a successful impaction bone graft reconstruction of a posterior femoral condylar defect, with the revision femoral component well-aligned.

Figure 11: A combined AP and lateral radiographic view of a successful revision TKA utilizing impaction grafting, demonstrating appropriate component positioning and early signs of graft integration.

Figure 12: Long-term follow-up radiograph showing stable implants and mature, incorporated impaction bone graft at the site of previous defects.

Figure 13: Another example of a well-integrated impaction bone graft at several years post-operation, highlighting the successful biological reconstruction.
Closure
- Irrigation and Hemostasis: Thorough irrigation and careful hemostasis are performed.
- Capsular Closure: The capsule and retinaculum are meticulously repaired to restore knee stability.
- Layered Closure: Standard layered closure of the subcutaneous tissues and skin. Drains may be used based on surgeon preference.
Complications & Management
While impaction bone grafting offers significant advantages for biological reconstruction in R-TKA, potential complications exist. Vigilant post-operative monitoring and prompt intervention are critical for successful outcomes.
Common Complications
-
Non-union or Fibrous Ingrowth of Graft:
- Incidence: Varies, but can be seen in 5-15% of cases, particularly with poor impaction technique, inadequate containment, or compromised host factors.
-
Management:
- Asymptomatic: Close observation.
- Symptomatic/Progressive Loosening: Revision surgery with further impaction grafting, consideration of structural allograft, metallic augments, or metaphyseal cones/sleeves to provide more immediate stability. Autologous bone marrow aspirate concentrate (BMAC) or platelet-rich plasma (PRP) may be considered as adjuncts to stimulate healing.
-
Graft Resorption:
- Incidence: Some degree of early remodeling and resorption is normal, but excessive resorption can lead to graft collapse and component subsidence. Incidence of clinically significant resorption leading to failure is low (1-5%).
- Management: Similar to non-union. Address underlying mechanical factors, revise with more stable construct if failure is imminent.
-
Infection (Periprosthetic Joint Infection - PJI):
- Incidence: Similar to general revision TKA rates (1-3%), but potentially higher in cases with extensive soft tissue dissection or prolonged surgical time.
-
Management:
- Acute PJI: Debridement, antibiotics, and implant retention (DAIR) in selected early cases, or two-stage revision (explantation, spacer, infection eradication, then reimplantation).
- Chronic PJI: Almost always requires two-stage revision.
-
Aseptic Loosening of Components:
- Incidence: Long-term follow-up studies suggest acceptable rates (5-year survival >90-95%), but still the primary mode of failure. Can be due to graft failure or inadequate host bone fixation.
- Management: Revision arthroplasty, addressing the bone defects with IBG, structural allograft, or augments as indicated.
-
Fracture of Host Bone During Impaction:
- Incidence: Rare (<1%), but possible if excessive force is used during impaction or if host bone is osteoporotic.
- Management: Immediate internal fixation (e.g., cerclage wires, plates) to stabilize the fracture, potentially with altered post-operative weight-bearing protocols.
-
Persistent Pain:
- Incidence: Multifactorial, can occur in up to 15-20% of TKA revisions.
- Management: Comprehensive workup to rule out infection, loosening, instability, or malalignment. Non-operative management (analgesics, physical therapy, injections) or targeted revision for identifiable cause.
-
Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE):
- Incidence: Variably reported, but significant risk in major orthopedic surgery. Prophylaxis is standard.
- Management: Anticoagulation, aggressive monitoring.
-
Neurovascular Injury:
- Incidence: Very rare (<0.5%).
- Management: Immediate surgical exploration and repair.
Common Complications, Incidence, and Salvage Strategies for Impaction Bone Grafting in R-TKA
| Complication | Incidence (Approximate) | Salvage Strategy |
|---|---|---|
| Graft Non-union / Fibrous Ingrowth | 5-15% | Revision with debridement, re-impaction of fresh graft, consideration of structural allograft, metallic augments, or metaphyseal cones/sleeves. Use of bone stimulators (e.g., BMAC, PRP). |
| Graft Resorption / Collapse | 1-5% (clinically significant) | Revision with debridement, re-impaction. If extensive, conversion to structural allograft, metallic augments, or metaphyseal cones/sleeves. Address any mechanical instability. |
| Periprosthetic Joint Infection | 1-3% | Acute: DAIR (Debridement, Antibiotics, Implant Retention) for selected cases. Chronic: Two-stage revision arthroplasty (explantation, antibiotic spacer, subsequent reimplantation). |
| Aseptic Loosening of Components | 5-10% (at 5-10 years) | Revision arthroplasty, re-addressing bone defects with repeat IBG, structural allograft, or use of more robust metallic augments/cones. Evaluate stem fixation. |
| Intraoperative Host Bone Fracture | <1% | Immediate stabilization with cerclage wires or small plates. Modify post-operative weight-bearing protocol (e.g., prolonged non-weight-bearing). |
| Persistent Pain | 15-20% | Comprehensive diagnostic workup (imaging, aspiration). Rule out infection, loosening, instability. Non-operative management (PT, analgesics) or targeted revision for identifiable cause (e.g., component malposition, ligamentous imbalance, extensor mechanism dysfunction). |
| DVT/PE | 1-5% | Anticoagulation, close monitoring, inferior vena cava filter if indicated. Prophylaxis crucial. |
| Neurovascular Injury | <0.5% | Immediate surgical exploration and primary repair. |
Post-Operative Rehabilitation Protocols
A structured and progressive rehabilitation protocol is paramount following impaction bone grafting to optimize graft incorporation, ensure component stability, and restore functional mobility. The key difference compared to other revision techniques is the critical need for protected weight-bearing during the initial phase of graft healing.
-
Immediate Post-Operative (Day 0-7):
- Weight-Bearing: Strictly non-weight-bearing (NWB) or touch-down weight-bearing (TDWB) on the operative extremity. This is the most crucial aspect to protect the immature graft. Patients should be educated on crutch or walker use.
-
Range of Motion (ROM):
- Continuous Passive Motion (CPM) machine may be initiated, with limits set by surgeon (e.g., 0-90 degrees initially), focusing on gentle, controlled motion to prevent stiffness without stressing the graft-prosthesis interface.
- Ankle pump exercises, quadriceps sets, and gluteal sets to maintain muscle tone and prevent DVT.
- Pain Management: Multimodal analgesia.
- Edema Control: Compression dressings, elevation, ice.
- DVT Prophylaxis: As per institutional protocol (chemical and mechanical).
-
Early Rehabilitation (Weeks 1-6):
- Weight-Bearing: Maintain NWB/TDWB status. Continue to emphasize protected ambulation with assistive devices.
- ROM: Gradually increase passive and active-assisted ROM, aiming for functional flexion (e.g., 0-100 degrees by 6 weeks), respecting pain and soft tissue healing. Avoid aggressive stretching or forced manipulation.
- Strengthening: Gentle isometric exercises for quadriceps, hamstrings, and gluteals. Start with straight leg raises in supine if tolerated. Avoid resisted knee extension for the first 6 weeks if patellar component revision or extensor mechanism compromise.
- Radiographic Monitoring: Initial radiographs (AP/Lateral) should be performed at 4-6 weeks to assess component alignment, stability, and early signs of graft incorporation (e.g., maintenance of graft density, absence of subsidence).
-
Intermediate Rehabilitation (Weeks 6-12):
- Weight-Bearing Progression: Based on clinical assessment and radiographic evidence of graft healing and component stability, weight-bearing can be gradually progressed from TDWB to partial weight-bearing (PWB), typically advancing 25% of body weight per week.
- ROM: Continue to work on achieving full functional ROM.
- Strengthening: Progress to isotonic strengthening exercises (e.g., wall slides, mini-squats, stationary cycling with low resistance). Focus on quadriceps and hamstring strength.
- Proprioception/Balance: Initiate balance exercises (e.g., single-leg stance with support).
-
Advanced Rehabilitation (Weeks 12+):
- Weight-Bearing: Full weight-bearing as tolerated once radiographic evidence of robust graft incorporation is confirmed and there is no pain or instability.
- ROM & Strengthening: Continue progressive strengthening with higher resistance exercises. Introduce functional activities (e.g., stair climbing, gentle walking on varied terrain).
- Return to Activity: Gradual return to light recreational activities. High-impact sports are generally discouraged after TKA, especially with extensive bone grafting.
-
Long-Term Follow-up:
Regular clinical and radiographic follow-up (e.g., annually for 5 years, then biannually) to monitor graft integration and implant survivorship.
Figure 14: Post-operative functional outcome in a patient who underwent impaction bone grafting and revision TKA, demonstrating good knee flexion and extension during gait.
Summary of Key Literature / Guidelines
Impaction bone grafting for contained and reconstructible uncontained bone defects in R-TKA is supported by a growing body of literature, highlighting its efficacy in achieving biological reconstruction and durable fixation.
Evidence for IBG Efficacy:
Early studies on IBG in TKA were largely based on principles derived from successful applications in revision hip arthroplasty. Initial concerns regarding the challenges of containment and graft stability in the knee have been largely addressed with improved surgical techniques and instrumentation.
- Mid-to-Long-Term Outcomes: Several series have reported promising mid-to-long-term survival rates for revision TKAs utilizing IBG. Survival rates ranging from 80-95% at 5-10 years have been documented, comparable to other complex revision techniques. Clinical scores (e.g., Knee Society Score, Western Ontario and McMaster Universities Osteoarthritis Index - WOMAC) show significant improvement post-operatively.
- Biological Incorporation: Histological and radiographic evidence consistently demonstrates successful graft incorporation, with remodeling of the impacted allograft into viable host bone over time. This biological integration is a key advantage over inert metallic augments.
-
Comparison with Other Techniques:
- Vs. Structural Allografts: While structural allografts provide immediate mechanical support, they have higher rates of non-union and slower incorporation compared to morcellized impaction grafts. They are often reserved for very large, uncontained AORI Type 3 defects where IBG alone is insufficient. IBG tends to have a lower risk of immune response and graft fracture.
- Vs. Metallic Augments/Cones/Sleeves: Metallic augments offer excellent immediate stability and obviate the need for extensive biological healing. However, they do not restore bone stock and can lead to stress shielding. Metaphyseal cones/sleeves, particularly those with porous coatings (e.g., trabecular metal), offer a compelling hybrid solution, providing both immediate stability and a scaffold for bone ingrowth. IBG often requires a longer period of protected weight-bearing, which can be a disadvantage in frail, elderly patients. However, for younger, active patients, the long-term biological restoration offered by IBG is highly attractive.
- Role in AORI Classification: IBG is widely considered the preferred method for AORI Type 1 and 2A defects. For AORI Type 2B and 3 defects, particularly those with metaphyseal involvement, IBG in combination with containment (wire mesh) or structural support (metaphyseal cones/sleeves, stemmed components) is a recognized and effective strategy.
- Guidelines: While no single universally adopted guideline explicitly dictates the use of IBG over all other options, major orthopedic societies and consensus statements generally acknowledge its role as a valid and effective biological option for bone defect management in R-TKA. The choice often hinges on defect size and location (AORI classification), patient factors, and surgeon experience. The emphasis remains on achieving a durable, stable construct that restores mechanical alignment and function.
In conclusion, impaction bone grafting represents a robust and biologically sound reconstructive option for managing bone defects in revision total knee arthroplasty. When meticulously performed, it offers the potential for true bone stock restoration and long-term implant survivorship, albeit requiring careful patient selection, precise surgical technique, and adherence to a protected post-operative rehabilitation protocol.
Clinical & Radiographic Imaging
You Might Also Like