Find the Top Knee Arthroscopy Surgeon in Dallas: Your Essential Guide
Key Takeaway
Looking for accurate information on Find the Top Knee Arthroscopy Surgeon in Dallas: Your Essential Guide? To find a top knee arthroscopy surgeon in Dallas, research online using sites like Healthgrades or Zocdoc, and seek referrals from your doctor or trusted contacts. Evaluate potential candidates based on their experience, credentials, patient ratings, and communication style. Selecting a surgeon in Dallas with proven expertise ensures quality care for your knee pain.
Introduction & Epidemiology
Knee arthroscopy represents a cornerstone procedure in contemporary orthopedic surgery, allowing for minimally invasive diagnosis and treatment of a vast array of intra-articular pathologies. Its evolution from a purely diagnostic tool to a therapeutic intervention has revolutionized the management of knee disorders, significantly reducing post-operative morbidity compared to traditional open approaches. The inherent advantages of arthroscopy, including enhanced visualization of intra-articular structures, smaller incisions, reduced pain, accelerated rehabilitation, and lower rates of complications, have cemented its status as the preferred modality for numerous knee conditions.
Epidemiologically, knee arthroscopy remains one of the most frequently performed orthopedic procedures worldwide. The incidence of knee pathologies requiring arthroscopic intervention is substantial, driven by factors such as an aging population, increased participation in recreational and competitive sports, and a growing prevalence of degenerative joint conditions. Common indications include symptomatic meniscal tears (degenerative, traumatic), chondral lesions, anterior cruciate ligament (ACL) ruptures, removal of loose bodies, management of synovial diseases, and evaluation of unexplained knee pain. While the volume of arthroscopic procedures for degenerative meniscal tears in stable knees has seen scrutiny in recent literature, its application in acute traumatic scenarios and mechanical symptoms remains robustly supported. Understanding the indications, contraindications, meticulous surgical technique, and comprehensive post-operative care is paramount for achieving optimal patient outcomes.
Surgical Anatomy & Biomechanics
A thorough understanding of the intricate surgical anatomy and biomechanics of the knee joint is foundational for safe and effective arthroscopic intervention. Precise navigation, accurate diagnosis, and successful treatment hinge upon this detailed knowledge.
Bony Anatomy
The knee is a modified hinge joint formed by the articulation of the distal femur, proximal tibia, and patella.
*
Distal Femur:
Comprises medial and lateral femoral condyles, separated posteriorly by the intercondylar notch. The condyles are asymmetric; the medial condyle is larger and extends more distally and anteriorly. The trochlear groove, an anterior continuation of the intercondylar notch, articulates with the patella.
*
Proximal Tibia:
Features medial and lateral tibial plateaus, separated by the intercondylar eminence (tibial spines). The plateaus are slightly concave, with the medial plateau being larger and more oval, and the lateral plateau smaller and rounder. The articular surfaces are covered by hyaline cartilage.
*
Patella:
A sesamoid bone within the quadriceps tendon, it possesses medial and lateral articular facets that articulate with the femoral trochlea. Its primary function is to enhance the quadriceps moment arm.
Ligamentous Structures
These ligaments provide static stability to the knee.
*
Cruciate Ligaments:
Located within the intercondylar notch.
*
Anterior Cruciate Ligament (ACL):
Originates from the posterior aspect of the lateral femoral condyle and inserts into the anteromedial aspect of the tibial plateau, anterior to the tibial spines. Composed of anteromedial (AM) and posterolateral (PL) bundles. The AM bundle is taut in flexion, and the PL bundle in extension. It resists anterior tibial translation and internal rotation.
*
Posterior Cruciate Ligament (PCL):
Originates from the anterior aspect of the medial femoral condyle and inserts onto the posterior aspect of the tibial plateau in the PCL fossa. Also has AM and PL bundles. The AM bundle is taut in flexion, and the PL bundle in extension. It resists posterior tibial translation.
*
Collateral Ligaments:
*
Medial Collateral Ligament (MCL):
Consists of superficial and deep components. The superficial MCL originates from the medial femoral epicondyle and inserts onto the proximal tibia (pes anserinus region). The deep MCL is a thickening of thear joint capsule, intimately attached to the medial meniscus. It resists valgus stress.
*
Lateral Collateral Ligament (LCL):
A cord-like structure originating from the lateral femoral epicondyle and inserting onto the fibular head. It is entirely extra-capsular and separate from the lateral meniscus. It resists varus stress.
*
Posterolateral Corner (PLC):
A complex of structures including the popliteus tendon and muscle, popliteofibular ligament, arcuate ligament complex, and fabellofibular ligament. This region is critical for resisting varus stress, external tibial rotation, and posterior tibial translation. Injury to the PLC often accompanies multi-ligamentous knee trauma.
Menisci
The medial and lateral menisci are crescent-shaped fibrocartilaginous structures that enhance joint congruity, distribute loads, absorb shock, aid in joint lubrication, and contribute to knee stability.
*
Medial Meniscus:
C-shaped, wider posteriorly, and firmly attached to the tibia via the coronary ligaments and to the deep MCL. It is less mobile than the lateral meniscus.
*
Lateral Meniscus:
More O-shaped, covers a larger portion of the lateral tibial plateau, and is only loosely attached to the capsule, allowing for greater mobility. The popliteus tendon courses through the posterolateral aspect, separating the lateral meniscus from the capsule.
*
Blood Supply:
The peripheral 10-30% of the menisci (red-red zone) receives vascular supply from the geniculate arteries, facilitating healing. The central portion (white-white zone) is avascular, while the transitional zone (red-white zone) has limited vascularity. This vascularity dictates repair vs. resection strategies.
Articular Cartilage
The articular surfaces of the femur, tibia, and patella are covered by hyaline cartilage, a specialized tissue that provides a low-friction surface for joint movement and distributes compressive loads. Its intricate structure (zones of varying collagen orientation and cell density) is key to its biomechanical properties. It has a limited capacity for self-repair.
Synovial Membrane & Plicae
The synovial membrane lines the non-articular surfaces of the joint, producing synovial fluid for lubrication and nutrition. Pathological conditions like synovitis can be diagnosed and treated arthroscopically. Synovial plicae are embryonic remnants that can become symptomatic (e.g., medial plica syndrome).
Neurovascular Structures
Understanding the proximity of neurovascular bundles to arthroscopic portals is critical for preventing iatrogenic injury.
*
Anterior Portals (AM, AL):
Relatively safe; however, the infrapatellar branch of the saphenous nerve courses near the AM portal, risking sensory neuropathy. The superficial peroneal nerve is lateral.
*
Posterior Portals (PM, PL):
Higher risk. The saphenous nerve and vein are medial to the posteromedial portal. The common peroneal nerve is lateral to the posterolateral portal. Most critically, the popliteal artery and vein lie directly posterior to the posterior capsule, necessitating careful transillumination and blunt dissection for posterior portal establishment.
Knee Biomechanics
The knee's complex motion involves a combination of flexion/extension, internal/external rotation, and subtle translation (e.g., screw-home mechanism).
*
Flexion/Extension:
Primarily a hinge motion, but coupled with axial rotation.
*
Rotation:
Critical for unlocking the knee during initial flexion. The ACL and PCL play significant roles in controlling anterior-posterior translation and rotation throughout the range of motion.
*
Load Transmission:
The menisci transmit approximately 50% of the compressive load in extension and up to 85% in 90 degrees of flexion, highlighting their crucial role in protecting articular cartilage.
Indications & Contraindications
The decision to proceed with knee arthroscopy requires careful consideration of both operative indications and patient-specific contraindications, prioritizing evidence-based practice and shared decision-making.
Indications for Knee Arthroscopy
Knee arthroscopy is indicated for a wide range of intra-articular pathologies, often after a trial of conservative management has failed.
-
Meniscal Pathology:
- Symptomatic Meniscal Tears: Acute traumatic tears (e.g., bucket-handle, radial, longitudinal, horizontal, complex flaps) causing mechanical symptoms (locking, catching, giving way, persistent pain). Repairable tears (e.g., peripheral longitudinal tears in vascular zones) are prioritized for repair over meniscectomy.
- Meniscal Cysts: Symptomatic cysts often associated with horizontal meniscal tears.
- Discoid Meniscus: Symptomatic discoid menisci (often lateral) that cause pain, clicking, or locking.
-
Chondral and Osteochondral Lesions:
- Chondromalacia/Chondral Flaps: Debridement of unstable chondral flaps causing mechanical symptoms.
- Osteochondral Defects (OCD): Diagnostic and therapeutic for stable or unstable OCD lesions, including microfracture, osteochondral autograft/allograft transplantation (OATS), or autologous chondrocyte implantation (ACI) procedures.
-
Ligamentous Pathology:
- ACL Rupture: Arthroscopic-assisted reconstruction is the gold standard for symptomatic instability. Arthroscopy is essential for diagnostic assessment, notchplasty, and tunnel placement.
- PCL Injuries: Diagnostic assessment and, in select cases, arthroscopic-assisted reconstruction.
- MCL/LCL Injuries: Primarily managed non-operatively; however, arthroscopy can address associated intra-articular pathology.
- Loose Bodies: Removal of intra-articular loose bodies (osteochondral fragments, synovia) causing pain, locking, or mechanical irritation.
-
Synovial Conditions:
- Synovitis: Diagnostic biopsy or synovectomy for chronic synovitis (e.g., rheumatoid arthritis, pigmented villonodular synovitis (PVNS), synovial chondromatosis).
- Plica Syndrome: Resection of symptomatic medial plicae.
-
Patellofemoral Pathology:
- Lateral Retinacular Release: For refractory patellofemoral pain or lateral patellar compression syndrome.
- Chondroplasty: For patellar or trochlear chondral lesions.
- Patellar Instability: Diagnostic arthroscopy for associated chondral lesions and to evaluate tracking.
- Infection: Septic arthritis requiring arthroscopic lavage and debridement, often with antibiotic administration.
- Fractures: Arthroscopically assisted reduction and internal fixation of select intra-articular fractures (e.g., tibial plateau fractures, intercondylar eminence fractures).
- Diagnostic Arthroscopy: For persistent, unexplained knee pain where non-invasive imaging is inconclusive, or to confirm/exclude specific intra-articular pathology prior to definitive treatment planning.
Contraindications for Knee Arthroscopy
Contraindications can be absolute or relative, necessitating careful patient selection.
-
Absolute Contraindications:
- Active Local Skin Infection: Cellulitis or open wounds at planned portal sites pose a significant risk of introducing infection into the joint.
- Severe Medical Comorbidities: Uncontrolled systemic diseases (e.g., severe cardiac, pulmonary, renal, or endocrine disorders) that preclude safe anesthesia or surgical tolerance.
- Ankylosis: Severely limited range of motion or bony ankylosis can prevent adequate instrument manipulation and visualization.
-
Relative Contraindications:
- Severe Arthrofibrosis: May limit visualization and instrument mobility, increasing technical difficulty and risk of iatrogenic injury.
- Extreme Obesity: Can make portal placement challenging, increase surgical time, and heighten complication risks (e.g., DVT, infection).
- Severe Osteoarthritis (Trifasicular OA): While chondroplasty can be performed, severe, end-stage osteoarthritis is often better managed with arthroplasty, as arthroscopy may offer limited long-term benefit for diffuse degenerative changes.
- Poorly Controlled Coagulopathy: Increased risk of hemarthrosis.
- Vascular Insufficiency: Increased risk of wound healing complications and compromised limb viability.
- Poor Patient Compliance: Rehabilitation is crucial for recovery, and non-compliance can compromise outcomes.
Operative vs. Non-Operative Indications
| Indication Type | Operative (Arthroscopic Intervention) | Non-Operative (Conservative Management) |
|---|---|---|
| Meniscal Tears | - Symptomatic tears (locking, catching, effusion) | - Asymptomatic tears |
| - Acute traumatic tears (especially in vascular zone for repair) | - Degenerative tears (stable knee, minimal mechanical symptoms) | |
| - Bucket-handle tears (true locking) | - Small, stable tears without mechanical symptoms | |
| Chondral Lesions | - Unstable chondral flaps causing mechanical symptoms | - Mild chondromalacia without mechanical symptoms |
| - Focal, full-thickness lesions (for microfracture/restoration) | - Diffuse degenerative cartilage loss (unless for debridement) | |
| Ligamentous Inst. | - Symptomatic ACL ruptures in active individuals | - Isolated grade I/II MCL/LCL sprains |
| - Multi-ligamentous injuries with instability | - Asymptomatic ACL tears with stable knee on examination | |
| Loose Bodies | - Any symptomatic intra-articular loose bodies | - Asymptomatic, stable loose bodies (rarely observed) |
| Synovial Path. | - Chronic synovitis, PVNS, synovial chondromatosis | - Acute, transient synovitis (e.g., post-traumatic) |
| - Symptomatic plica syndrome | - Asymptomatic plica | |
| Fractures | - Displaced intra-articular tibial plateau/eminence fractures | - Non-displaced, stable intra-articular fractures |
| Infection | - Septic arthritis (urgent lavage and debridement) | - Cellulitis (treat with antibiotics prior to joint involvement) |
| Pain | - Persistent, unexplained pain after non-invasive workup | - Mild, intermittent pain responsive to analgesia/PT |
Note: The primary determinant for operative intervention, particularly in degenerative conditions, is often the failure of a structured course of non-operative management (e.g., physical therapy, anti-inflammatory medication, injections) and the presence of significant mechanical symptoms or functional limitations.
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and precise patient positioning are critical for optimizing surgical safety, efficiency, and outcomes in knee arthroscopy.
Pre-Operative Assessment
- History and Physical Examination: A comprehensive medical history, including comorbidities, medications (especially anticoagulants), allergies, and prior surgical history, is essential. A detailed knee examination should assess range of motion (ROM), effusion, tenderness, ligamentous stability (e.g., Lachman, pivot shift, posterior drawer, varus/valgus stress tests), meniscal signs (e.g., McMurray, Apley), and neurovascular status. Documentation of pre-existing deficits is crucial.
-
Imaging Review:
- Plain Radiographs: Weight-bearing anteroposterior (AP), lateral, patellar skyline, and oblique views are standard to assess alignment, joint space narrowing, osteophytes, and occult fractures.
- Magnetic Resonance Imaging (MRI): The gold standard for soft tissue evaluation, providing detailed assessment of menisci, ligaments, articular cartilage, and bone marrow edema. Review all sequences (T1, T2, PD, fat-suppressed) for specific pathology.
- Computed Tomography (CT): Useful for complex bony pathologies, malalignment, or pre-operative planning for osteochondral defects.
- Informed Consent: A thorough discussion with the patient regarding the diagnosis, proposed procedure, potential benefits, risks (e.g., infection, DVT, nerve/vascular injury, stiffness, pain, failure), and alternative treatments (including non-operative management) is paramount.
- Medical Optimization: Address any systemic medical issues, optimize chronic conditions, and manage anticoagulation according to institutional protocols. Pre-operative labs, EKG, and anesthetic consult may be required based on patient comorbidities.
Equipment & Operating Room Setup
- Arthroscopy Tower: Includes a high-definition monitor, camera control unit, light source, fluid pump/inflow system, shaver control unit, and image/video recording device.
- Instrumentation: Standard arthroscopy set (cannulas, trocars, blunt/sharp obturators, arthroscopic probe, basket forceps, punches, scissors, graspers, arthroscopic shaver/burr), and procedure-specific instruments (e.g., suture passers, drill guides, graft-harvesting instruments, suture anchors for meniscal repair or ACL reconstruction).
- Tourniquet: A pneumatic tourniquet is routinely used, typically placed high on the ipsilateral thigh. Pre-inflation exsanguination is performed with an Esmarch bandage. Inflation pressure is usually 250-300 mmHg or 100 mmHg above systolic blood pressure. Tourniquet time should be minimized and monitored.
- Leg Holder/Positioner: A lateral post with a foot support or traction device is commonly used to apply valgus stress and facilitate joint distraction. Some surgeons prefer a free-leg technique without a post.
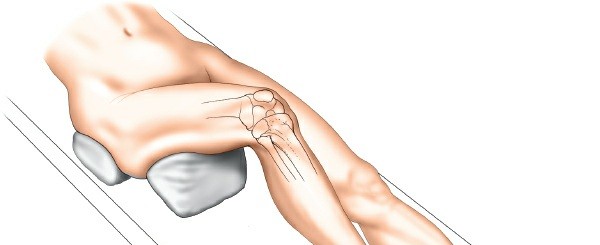
Patient Positioning
- Supine Position: The patient is positioned supine on the operating table. Ensure adequate padding at pressure points.
- Leg Preparation: The entire lower extremity from the groin to the toes is prepped and draped to allow for full range of motion, knee flexion beyond 90 degrees, and manipulation of the foot.
- Tourniquet Application: Applied to the proximal thigh.
- Leg Holder/Post Placement: If a lateral post is used, it is placed just proximal to the knee joint, securely against the medial aspect of the thigh, applying a gentle valgus force to open the medial compartment. A foot holder or traction device may be utilized to apply traction, particularly for improved visualization of the posterior compartments.
- Examination Under Anesthesia (EUA): Prior to prepping and draping, a thorough EUA is performed to re-evaluate the knee's stability, range of motion, and confirm pre-operative findings. This is crucial as muscle guarding and pain can mask instability in the awake patient. Document findings.
- Sterile Prep and Drape: The entire lower extremity is prepped with an antiseptic solution (e.g., chlorhexidine-alcohol) and sterilely draped, allowing the surgeon to freely manipulate the knee through a full range of motion. A stockinette is typically applied from the mid-thigh to the foot, followed by an adhesive incise drape around the knee.
Detailed Surgical Approach / Technique
Knee arthroscopy follows a systematic approach, combining diagnostic evaluation with therapeutic intervention. The general principles involve fluid management, triangulation, and careful portal creation to minimize iatrogenic injury.
General Principles of Arthroscopy
- Distraction and Fluid Management: A constant inflow of sterile saline via a gravity feed or mechanical pump distends the joint capsule, creating a working space and clearing debris. Adequate fluid pressure (typically 50-80 mmHg) is crucial for visualization and joint lavage.
- Triangulation: The technique of positioning the arthroscope and working instrument at different portals to allow precise manipulation and visualization within the joint.
- Portal Creation: Small incisions through the skin, subcutaneous tissue, and capsule, followed by blunt dissection, to introduce the arthroscope and instruments. Precise placement is paramount for safe and effective access.
Portal Placement
Standard knee arthroscopy typically utilizes anteromedial (AM) and anterolateral (AL) portals. Accessory portals are created as needed.
-
Anterolateral (AL) Portal (Visualization Portal):
- Landmark: Approximately 1 cm lateral to the patellar tendon, at the level of the inferior pole of the patella or slightly above the lateral joint line.
- Technique: A small skin incision (approximately 5-7 mm) is made. A blunt trocar and cannula are advanced towards the intercondylar notch, aiming posterosuperiorly, parallel to the tibial plateau. Gentle pressure and a "pop" sensation indicate capsular penetration.
- Safety: Avoid injury to the lateral patellar retinaculum and superficial peroneal nerve branches.
-
Anteromedial (AM) Portal (Working Portal):
- Landmark: Approximately 1 cm medial to the patellar tendon, at the level of the inferior pole of the patella or slightly above the medial joint line.
- Technique: After establishing the AL portal and visualizing the joint, the arthroscope is inserted. The AM portal is then created under direct arthroscopic visualization. A spinal needle is first introduced from the skin to confirm optimal trajectory and ensure no iatrogenic damage to intra-articular structures. The needle should appear lateral to the medial meniscus and medial to the patellar tendon. The skin incision is made, and a blunt trocar is advanced through the path of the needle.
- Safety: Protect the infrapatellar branch of the saphenous nerve.
-
Posteromedial (PM) Portal:
- Indications: Visualization/treatment of posterior horn medial meniscal pathology, PCL evaluation/reconstruction, loose body removal from the posterior compartment.
- Landmark: 1-2 cm superior to the medial joint line, posterior to the MCL, adjacent to the posteromedial corner.
- Technique: Established under direct visualization from the intercondylar notch (through the AL portal), using a switching stick or spinal needle. Care must be taken to avoid the saphenous nerve and vein. The blunt trocar is directed towards the center of the posterior compartment, above the posterior horn of the medial meniscus.
- Safety: Critical awareness of the saphenous nerve and vein anteriorly, and the popliteal artery and vein posteriorly. Transillumination and digital palpation of the popliteal fossa are essential.
-
Posterolateral (PL) Portal:
- Indications: Posterior horn lateral meniscal pathology, loose body removal, PLC assessment.
- Landmark: Similar to PM, 1-2 cm superior to the lateral joint line, posterior to the LCL, adjacent to the posterolateral corner.
- Technique: Similar to PM, under direct visualization.
- Safety: Protect the common peroneal nerve laterally and the popliteal artery/vein posteriorly.
Systematic Diagnostic Arthroscopy
Once portals are established, a systematic evaluation of all compartments is performed:
1.
Suprapatellar Pouch:
Synovial inflammation, plicae, loose bodies, articular cartilage of the patella and trochlea.
2.
Patellofemoral Joint:
Articular surfaces of patella and trochlea, patellar tracking.
3.
Medial Gutter:
Plicae, loose bodies.
4.
Medial Compartment:
Medial femoral condyle, medial tibial plateau articular cartilage, medial meniscus (anterior horn, body, posterior horn). Probe the meniscus for stability and tears.
5.
Intercondylar Notch:
ACL (integrity, tension, tears), PCL (origin, insertion, tears), notch dimensions, cyclops lesions.
6.
Lateral Compartment:
Lateral femoral condyle, lateral tibial plateau articular cartilage, lateral meniscus (anterior horn, body, posterior horn, popliteal hiatus). Probe the meniscus.
7.
Lateral Gutter:
Loose bodies.
8.
Posterior Compartments:
If posterior portals are used, evaluate posterior capsule, PCL, and posterior aspects of menisci.
Detailed Surgical Techniques (Examples)
1. Arthroscopic Partial Meniscectomy
- Indication: Symptomatic, irreparable meniscal tears (e.g., complex, degenerative, radial, horizontal tears extending to avascular zones, unstable flap tears).
-
Technique:
- Visualization: Position the arthroscope and instruments for optimal viewing of the torn meniscus. Apply valgus or varus stress with knee flexion/extension as needed to open the compartment.
- Probing: Use an arthroscopic probe to assess the tear pattern, stability, and extent. Identify the unstable fragment.
- Resection: Use a combination of arthroscopic basket forceps, punches, and a shaver to resect the unstable meniscal fragment. The goal is to create a stable, smooth rim, preserving as much healthy meniscal tissue as possible to maintain load-bearing function.
- Debridement: Use a motorized shaver to smooth the edges of the resected meniscus and remove any remaining frayed tissue.
- Final Assessment: Re-probe the remaining meniscus to ensure stability and absence of further unstable fragments. Check for associated chondral lesions.
2. Arthroscopic Meniscal Repair
- Indication: Acute, traumatic longitudinal tears in the vascularized red-red or red-white zones, especially in younger, active patients, or bucket-handle tears if reduced and stable.
-
Technique:
- Tear Assessment and Debridement: Assess the tear pattern, length, and reducibility. Debride the tear edges and the adjacent capsule (rasping or synovial abrasion) to promote bleeding and enhance healing potential.
- Reduction: Reduce the displaced meniscal fragment back to its anatomical position.
-
Repair Technique (e.g., All-Inside Repair):
- Device Delivery: An all-inside repair device (e.g., Fast-Fix, Meniscal Cinch) is used. The first implant is passed from the meniscus into the capsule, followed by the second implant, typically 5-10 mm apart, across the tear.
- Suture Tensioning: The sutures connecting the implants are then tensioned and locked, bringing the torn edges together and apposing the meniscus to the capsule.
- Multiple Constructs: Multiple suture constructs are typically placed along the tear to ensure stable repair.
-
Repair Technique (e.g., Inside-Out Repair):
- Needle Placement: Long, curved cannulas and needles are used to pass non-absorbable sutures from the intra-articular side, through the meniscus, and out through the capsule.
- Retrieval: The needles and sutures are retrieved from a small accessory incision on the skin (often protected by a posterior "popliteal" incision or specific skin protectors).
- Knot Tying: The sutures are tied over the capsule, outside the joint, securing the repair.
- Final Assessment: Visually confirm stable reduction and appropriate tension. Avoid overtightening.
3. Arthroscopic Microfracture (for Chondral Lesions)
- Indication: Full-thickness chondral defects (International Cartilage Repair Society (ICRS) Grade IV) in contained lesions, typically 1-4 cm² in younger patients.
-
Technique:
- Lesion Preparation: Debride any unstable chondral flaps around the lesion to create stable, vertical shoulders. Remove all calcified cartilage down to healthy subchondral bone.
- Microfracture Drilling: Use a sharp arthroscopic awl or small drill bit (typically 1 mm) to create multiple microfracture holes within the defect.
- Hole Spacing and Depth: Holes should be spaced 3-4 mm apart to allow for an adequate blood clot to form. The depth should be sufficient to penetrate the subchondral bone plate and tidemark, allowing marrow elements (mesenchymal stem cells, growth factors) to egress into the defect. Observe egress of fat droplets and blood.
- Final Irrigation: Lavage the joint to remove debris.
- Internervous Planes: For standard anterior knee arthroscopy, specific internervous planes are not typically dissected as in open approaches. Instead, portals are created through capsular and retinacular structures. However, for posterior portals, careful blunt dissection is crucial to avoid vital neurovascular structures, particularly the popliteal neurovascular bundle in the posterior compartment and branches of the saphenous and peroneal nerves.
Complications & Management
While knee arthroscopy is generally considered safe, complications, though rare, can occur. Early recognition and appropriate management are vital for mitigating their impact.
Common Complications and Salvage Strategies
| Complication | Incidence | Etiology / Risk Factors | Clinical Presentation | Salvage Strategy / Management |
|---|---|---|---|---|
| Infection (Septic Arthritis) | 0.01% - 0.5% | Poor sterile technique, patient comorbidities, prolonged surgery | Pain, swelling, warmth, fever, limited ROM, elevated WBC/ESR/CRP | Urgent arthroscopic lavage & debridement, targeted IV antibiotics (based on cultures), serial lavages if needed |
| Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE) |
DVT: 0.1% - 1%
PE: <0.1% |
Immobility, tourniquet use, hypercoagulable state, obesity |
DVT: Calf pain/swelling, tenderness
PE: Dyspnea, chest pain, tachycardia, hypoxia |
Anticoagulation (LMWH, oral), early mobilization, compression stockings; IVC filter for recurrent PE/contraindication to anticoagulation |
| Nerve Injury | 0.2% - 1% | Direct trauma from portal, excessive traction, tourniquet compression | Sensory loss (infrapatellar branch of saphenous nerve is most common), motor weakness (peroneal nerve - foot drop) | Conservative (observation for neuropraxia), nerve blocks, neurolysis; surgical exploration/repair for persistent severe deficits |
| Vascular Injury | <0.01% | Popliteal artery/vein during posterior portal creation, direct instrument trauma | Swelling, rapidly expanding hematoma, pulsatile bleeding, absent distal pulses, limb ischemia | Immediate tourniquet inflation, urgent surgical exploration, vascular repair (by vascular surgeon), compartment fasciotomy if needed |
| Hemarthrosis | 0.5% - 2% | Inadequate hemostasis, vessel injury, post-op anticoagulation | Acute painful swelling, ecchymosis, restricted ROM | Aspiration (diagnostic/therapeutic), compression, RICE, observation. Repeat aspiration if tense. |
| Arthrofibrosis / Stiffness | 1% - 5% | Inadequate pain control, delayed rehab, infection, poor surgical technique | Restricted ROM, pain with movement, quadriceps weakness | Aggressive physical therapy, manipulation under anesthesia, arthroscopic lysis of adhesions (LOA), quadricepsplasty in severe cases |
| Extravasation of Fluid / Compartment Syndrome |
Fluid extrav: Common
Comp. Synd: <0.01% |
High pump pressure, prolonged surgery, capsular defects, tight dressings |
Extrav: Swelling, crepitus in soft tissues
Comp. Synd: Severe pain out of proportion, pallor, paresthesia, pulselessness |
Extrav: Reduce pump pressure, tight dressing removal, observation
Comp. Synd: EMERGENCY fasciotomy |
| Instrument Breakage | Rare | Faulty instrument, forceful manipulation | Retained metallic/plastic fragment in joint | Arthroscopic retrieval (if visible), open arthrotomy for inaccessible fragments |
| Complex Regional Pain Syndrome (CRPS) | <0.1% | Unclear etiology, possibly nerve irritation, psychological factors | Severe disproportionate pain, allodynia, hyperalgesia, swelling, vasomotor changes | Multidisciplinary approach: regional nerve blocks, gabapentin/pregabalin, physical therapy, psychological support |
| Graft Failure (ACL Recon) | 2% - 10% | Technical error, early return to sport, poor graft incorporation | Instability, positive Lachman/pivot shift, recurrent effusions | Revision ACL reconstruction (often with staged procedure or alternative graft) |
| Meniscal Repair Failure | 10% - 30% | Tear type/location, poor healing, early stress | Persistent pain, mechanical symptoms (locking, clicking), recurrent effusion | Repeat arthroscopy for partial meniscectomy or revision repair |
General Management Principles for Complications
- Prevention: Adherence to sterile technique, meticulous hemostasis, careful portal placement, appropriate tourniquet use, judicious fluid management, and early post-operative mobilization are crucial.
- Early Recognition: High index of suspicion for post-operative complaints, especially disproportionate pain, swelling, or fever.
- Prompt Intervention: Many complications, particularly infection and vascular injury, require urgent and decisive intervention to prevent long-term morbidity.
- Multidisciplinary Approach: Management of complex complications often benefits from collaboration with infectious disease specialists, vascular surgeons, neurologists, pain management specialists, and physical therapists.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is an integral component of successful knee arthroscopy, critical for restoring function, strength, and proprioception while protecting healing tissues. Protocols are individualized based on the specific procedure performed, patient factors, and surgeon preference.
General Principles
- Pain and Swelling Control: RICE (Rest, Ice, Compression, Elevation), analgesics (opioids, NSAIDs, acetaminophen), and regional nerve blocks are used to manage pain and reduce post-operative edema.
- Early Mobilization (as appropriate): To prevent stiffness and DVT.
- Protection of Healing Tissues: Adherence to weight-bearing restrictions and range-of-motion (ROM) limitations is paramount for procedures involving repair or reconstruction (e.g., meniscal repair, ACL reconstruction, microfracture).
- Progressive Loading: Gradual increase in activity and resistance to safely rebuild strength and endurance.
- Neuromuscular Control and Proprioception: Essential for dynamic joint stability and injury prevention, particularly after ligamentous or meniscal repair.
Phase-Specific Rehabilitation (General Framework)
Phase I: Protection & Early Motion (typically Weeks 0-6)
-
Goals:
- Control pain and swelling.
- Achieve full passive and/or active-assisted ROM (within prescribed limits).
- Protect surgical site/healing tissue.
- Initiate muscle activation.
-
Activities:
- RICE: Continuous application.
- Weight Bearing: As per protocol (e.g., non-weight bearing, partial weight bearing with crutches, weight bearing as tolerated).
- ROM: Passive range of motion (PROM) or active-assisted range of motion (AAROM) exercises. Continuous Passive Motion (CPM) machine may be used for specific procedures (e.g., microfracture).
- Muscle Activation: Quadriceps setting, gluteal sets, gentle hamstring curls (if not contraindicated by graft harvest), ankle pumps.
- Bracing: May be used for protection (e.g., for ACL reconstruction, meniscal repair).
Phase II: Progressive Strengthening & Neuromuscular Control (typically Weeks 6-12)
-
Goals:
- Restore full, pain-free ROM.
- Improve muscle strength and endurance.
- Enhance proprioception and dynamic stability.
-
Activities:
- Full ROM: Work towards achieving full flexion and extension.
- Strengthening: Closed-chain exercises (mini-squats, leg presses, wall slides, lunges), stationary cycling, elliptical trainer. Gradual progression of resistance.
- Balance & Proprioception: Single-leg standing, balance board/foam, perturbation training.
- Core Strengthening: Important for overall kinetic chain stability.
Phase III: Return to Activity (typically Months 3-6+)
-
Goals:
- Maximize strength, power, and agility.
- Achieve sport-specific or activity-specific functional goals.
- Safe return to desired activities.
-
Activities:
- Advanced Strengthening: Plyometric exercises (box jumps, hopping), advanced closed-chain exercises, increased resistance.
- Agility Drills: Ladder drills, cone drills, cutting maneuvers.
- Sport-Specific Training: Gradual progression of sport-specific activities (running, jumping, throwing).
- Return to Play/Activity Testing: Objective criteria (e.g., strength symmetry, hop tests, functional movement screens) are often used to guide return to high-impact activities.
Procedure-Specific Rehabilitation Considerations
-
Partial Meniscectomy:
- Fastest recovery.
- Weight bearing as tolerated immediately.
- Full ROM initiated early.
- Focus on pain control and regaining strength.
-
Meniscal Repair:
- More conservative.
- Protected weight bearing (e.g., partial weight bearing with crutches for 4-6 weeks).
- Limited knee flexion (e.g., 0-90 degrees for 4-6 weeks) to protect the repair from shear forces.
- Slower progression of strengthening and agility to allow for healing.
-
ACL Reconstruction:
- Brace worn for protection (often for 4-6 weeks).
- Weight-bearing restrictions vary by surgeon/graft type.
- Emphasis on early quad activation and full extension.
- Avoid open-chain hamstring curls initially for hamstring autografts.
- Avoid open-chain knee extensions (0-30 degrees) initially for patellar tendon autografts (high stress on graft).
- Return to sport typically 9-12 months post-op, guided by objective criteria.
-
Microfracture:
- Non-weight bearing or toe-touch weight bearing for 6-8 weeks.
- CPM machine often used for 6-8 hours daily to promote cartilage formation.
- Slower progression of weight bearing and impact activities to allow the fibrocartilaginous repair tissue to mature.
Role of Physical Therapy: A skilled physical therapist is indispensable for guiding the patient through the rehabilitation process, ensuring proper technique, advancing exercises safely, and addressing any setbacks. Patient education on activity modifications and adherence to the protocol is crucial for long-term success.
Summary of Key Literature / Guidelines
The field of knee arthroscopy is continuously evolving, driven by evidence from high-level clinical research. Staying abreast of key literature and professional guidelines is essential for contemporary orthopedic practice.
Major Professional Societies & Guidelines
- American Academy of Orthopaedic Surgeons (AAOS): Publishes clinical practice guidelines (CPGs) and appropriate use criteria (AUC) for various orthopedic conditions, including meniscal tears, ACL injuries, and osteoarthritis. These guidelines are evidence-based, derived from systematic reviews of the literature, and provide recommendations for diagnosis and treatment.
- American Orthopaedic Society for Sports Medicine (AOSSM): Focuses on sports-related injuries and provides consensus statements and clinical commentaries relevant to arthroscopic procedures, particularly for ligamentous and meniscal pathology in athletes.
- International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine (ISAKOS): A global organization that promotes education and research in arthroscopy and sports medicine, contributing to consensus statements and global best practices.
- European Society of Sports Traumatology, Knee Surgery & Arthroscopy (ESSKA): Similar to AOSSM and ISAKOS, providing a European perspective on best practices.
Key Literature & Concepts
-
Arthroscopic Partial Meniscectomy (APM) for Degenerative Meniscal Tears:
- Controversy: Several landmark randomized controlled trials (RCTs), notably the FIDELITY trial ( Finnish Degenerative Meniscus Lesion Study ) published in The New England Journal of Medicine (2013, 2016), and other studies (e.g., British Medical Journal 2017 meta-analysis), have questioned the benefit of APM over sham surgery or physical therapy alone for degenerative meniscal tears without mechanical locking symptoms in stable knees. These studies suggest no significant additional benefit from surgery in this specific patient population.
- Implication: Emphasizes the importance of careful patient selection, emphasizing APM for mechanical symptoms (true locking, catching) and failed conservative management, rather than solely for MRI findings of degeneration. Shared decision-making with patients is crucial.
-
Meniscal Repair vs. Meniscectomy:
- Principle: Meniscal repair is generally preferred over meniscectomy when technically feasible (tear type, location in vascularized zone, patient age/activity level) to preserve meniscal tissue and mitigate the long-term risk of osteoarthritis.
- Evidence: Long-term follow-up studies consistently demonstrate that meniscal preservation is associated with better long-term knee health and lower rates of degenerative changes compared to total meniscectomy. Success rates for meniscal repair vary by tear pattern, patient age, and associated pathology (e.g., concomitant ACL reconstruction improves healing rates).
-
ACL Reconstruction Techniques and Outcomes:
- Evolution: Debate continues regarding optimal graft choice (autograft: bone-patellar tendon-bone (BTB), hamstring tendon; allograft), tunnel placement (anatomic single bundle vs. double bundle), and fixation methods.
- Evidence: Meta-analyses and large registry studies provide data on revision rates, functional outcomes, and return to sport. While anatomic single-bundle reconstruction remains the standard, individual patient factors and surgeon experience guide specific choices. The MOON (Multicenter Orthopaedic Outcomes Network) consortium has been instrumental in providing long-term outcomes data for various ACL reconstruction techniques.
- Rehabilitation: Evidence strongly supports structured, progressive rehabilitation, with return to high-impact activities often delayed until 9-12 months to allow for graft maturation and reduce re-rupture rates.
-
Chondral Lesion Management:
- Microfracture: Early results were promising, but long-term data indicates that the fibrocartilaginous repair tissue is biomechanically inferior to native hyaline cartilage and may degenerate over time. It is best suited for smaller, contained lesions in younger patients.
- Advanced Techniques: Autologous chondrocyte implantation (ACI), matrix-induced autologous chondrocyte implantation (MACI), and osteochondral autograft/allograft transfer systems (OATS) have shown promise for larger or more complex defects, with varying levels of evidence and cost-effectiveness.
-
Role of Patient-Reported Outcome Measures (PROMs):
- Importance: Validated PROMs (e.g., KOOS, Lysholm score, WOMAC, IKDC) are increasingly recognized as essential tools for objectively assessing patient function, pain, and quality of life before and after arthroscopic procedures. They provide valuable data for research, quality improvement, and shared decision-making.
In conclusion, the practice of knee arthroscopy is dynamic, necessitating a commitment to lifelong learning, critical appraisal of scientific literature, and adherence to evolving clinical guidelines. Optimal patient care requires a foundation in surgical anatomy, a meticulous approach to technique, proactive management of potential complications, and a robust, individualized rehabilitation strategy, all guided by the best available evidence.
You Might Also Like