Free Functioning Muscle Transfer & Vascularized Bone Grafts
Key Takeaway
Free functioning muscle transfer (FFMT) and vascularized bone grafting represent the pinnacle of reconstructive microsurgery. This guide details the Manktelow technique for restoring forearm function using gracilis transfers, emphasizing the critical length-tension relationship via 5-cm interval marking. Furthermore, it explores the indications, anatomical characteristics, and surgical nuances of vascularized fibula, iliac crest, and rib grafts for complex skeletal defect reconstruction, providing orthopaedic surgeons with an evidence-based framework for optimal clinical outcomes.
INTRODUCTION TO RECONSTRUCTIVE MICROSURGERY
The advent of microvascular surgery has revolutionized the orthopaedic approach to catastrophic limb injuries, massive tumor resections, and severe ischemic contractures. When local reconstructive options are exhausted, the free transfer of functioning muscle and vascularized bone becomes the definitive salvage pathway. These procedures demand not only meticulous microsurgical technique but also a profound understanding of biomechanics, muscle physiology, and neurovascular anatomy.
This comprehensive guide delineates the principles of Free Functioning Muscle Transfer (FFMT), specifically focusing on the Manktelow technique for forearm reconstruction, followed by an in-depth analysis of free vascularized bone grafts, including the fibula, iliac crest, and rib.
FREE TRANSFER OF FUNCTIONING MUSCLE TO THE FOREARM
The primary goal of transferring a functioning muscle to the forearm is the restoration of active finger flexion or extension following devastating conditions such as Volkmann’s ischemic contracture, severe brachial plexus avulsions, or massive traumatic soft-tissue loss. The gracilis, latissimus dorsi, and pectoralis major are the most frequently utilized donor muscles due to their reliable neurovascular pedicles and favorable excursion profiles.
Biomechanics and the Length-Tension Relationship
The functional success of any muscle transfer hinges entirely on restoring the muscle's optimal physiological length. According to the Blix curve, a muscle generates its maximum active tetanic tension at its resting length. If a muscle is inset too loosely, it will expend its excursion merely taking up slack; if inset too tightly, it will suffer from passive insufficiency and ischemia.
Clinical Pearl: The Manktelow 5-cm marking technique is the gold standard for preserving the length-tension relationship. By marking the muscle at its maximal physiological length before harvest and restoring that exact distance during inset, the surgeon guarantees optimal sarcomere overlap for maximum postoperative contractile force.
Preoperative Planning and Recipient Site Preparation
Before initiating the donor harvest, the recipient forearm must be meticulously prepared.
- Exposure and Debridement: Radically debride all fibrotic and non-viable muscle tissue. Expose the medial epicondyle (for flexor reconstruction) or the lateral epicondyle (for extensor reconstruction).
- Vascular Assessment: Identify and dissect the recipient artery and veins. Before proceeding with the donor harvest, definitively confirm that the recipient artery exhibits robust, free pulsatile flow.
- Nerve Preparation: Isolate the recipient motor nerve (e.g., anterior interosseous nerve for flexor reconstruction). The nerve should be sectioned back to healthy fascicles.
- Soft Tissue Coverage Plan: Plan to cover the distal musculotendinous repair with a local skin flap or a skin paddle carried with the transplanted muscle. The proximal muscle belly can be covered with a split-thickness skin graft if primary closure is not feasible.
Donor Muscle Harvest: The Gracilis Flap
The gracilis muscle is highly favored for forearm reconstruction due to its parallel fiber arrangement, which provides excellent excursion, and its reliable neurovascular pedicle (ascending branch of the medial circumflex femoral artery and the anterior branch of the obturator nerve).
- Positioning: Place the patient supine with the hip abducted and externally rotated, and the knee slightly flexed (frog-leg position).
- Incision: Make a longitudinal incision along the medial thigh, posterior to the palpable adductor longus tendon.
- Dissection: Identify the gracilis muscle. Dissect the anterior margin to locate the neurovascular pedicle entering the deep surface of the muscle in the proximal third.
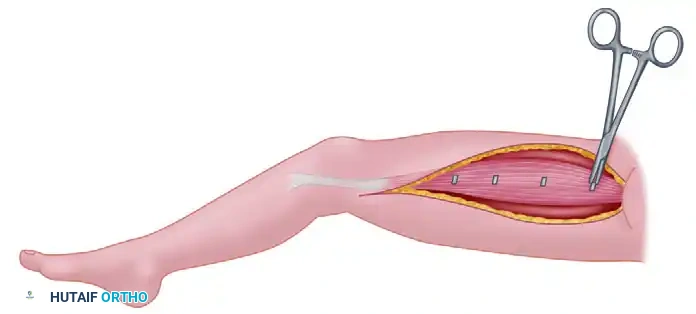
- Length Determination (Manktelow Technique): Position the extremity so the muscle is at its maximal physiological length. For the gracilis, this requires the knee to be fully extended.
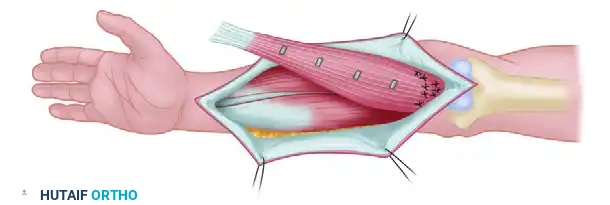
- Marking: Place metal clips or non-absorbable suture markers on the surface of the muscle belly at exact 5-cm intervals.
- Harvest: Once the length determinations are secured, detach the muscle from its origin (pubic symphysis) and insertion (pes anserinus). Carefully section the artery, veins, and nerve. Leave the muscle attached to its major vascular pedicle until the recipient site is absolutely ready, thereby minimizing ischemia time.
Muscle Transfer and Inset
Immediately transfer the harvested muscle to the prepared forearm. The orientation of the muscle must prioritize the ease of neurovascular repair. This frequently requires reversing the ends of the muscle so that the anatomical origin becomes the new insertion.
- Proximal Attachment:
- Flexor Surface: Attach the origin of the muscle securely to the medial epicondyle and surrounding antebrachial fascia.
- Extensor Surface: Attach the origin to the lateral epicondyle, adjacent fascia, and periosteum.
- Temporary Fixation: Loosely suture the muscle in place to prevent displacement or traction on the pedicle during the delicate neurovascular repairs.
Microvascular and Microneural Anastomosis
Position the transferred muscle so that the arterial and venous anastomoses can be executed without tension or kinking.
Surgical Warning: Position the vascular repairs so that the nerve coaptation is as close to the muscle's motor endplates as possible. Shortening the distance of nerve regeneration (ideally 2 to 3 cm, as reported by Manktelow) drastically reduces the period of muscle denervation and prevents irreversible motor endplate atrophy.
- Vascular Repair: Blood loss can be mitigated by repairing one or more large veins before the artery. However, the absolute priority is minimizing total ischemia time; thus, the specific order of repair is secondary to efficiency.
- Neural Repair: Following successful revascularization, perform a tension-free, epineurial or group fascicular repair using 10-0 or 11-0 nylon sutures under the operating microscope.
Distal Tendon Weaving and Tensioning
- Restoring Length: Apply traction to the transferred muscle to stretch it from its new origin toward the distal recipient tendons. Pull the muscle until the pre-placed markers exactly reestablish their 5-cm intervals.
- Marking the Tendons: At this precise tension, mark the appropriate locations on the recipient tendons (e.g., flexor digitorum profundus) for repair.
- Tendon Coaptation: Secure the recipient tendons to each other with side-to-side sutures to ensure a unified cascade. Weave the recipient tendons into the transplanted muscle's tendon (or directly into the muscle belly using locking mattress sutures if no donor tendon is available).
- Closure: Close the wounds loosely to avoid any constriction of the microvascular pedicle. Apply split-thickness skin grafts over the proximal muscle belly if required.
Postoperative Care and Rehabilitation
The postoperative protocol is as critical as the surgical execution.
- Immediate Post-Op: Maintain systemic circulation with optimal peripheral perfusion and adequate hydration. The extremity is immobilized in a plaster splint with the wrist and fingers moderately flexed to relieve tension on the repairs. Anticoagulation protocols (e.g., aspirin, dextran, or heparin) are instituted based on surgeon preference and institutional guidelines.
- 3 Weeks: Initiate gentle, controlled passive stretching exercises to maintain joint mobility and promote tendon gliding without disrupting the repair.
- 2 to 4 Months: As reinnervation occurs (evidenced by advancing Tinel's sign and palpable muscle flicker), begin active finger flexion exercises.
- 6 to 12 Months: Introduce daily active resistive exercises. Intensive physical therapy is paramount to maximize excursion and strength.
- Long-Term: Muscle strength typically plateaus and stabilizes 2 to 3 years following the transplantation.
FREE VASCULARIZED BONE GRAFTS
When skeletal defects exceed 6 to 8 cm—often due to tumor resection, osteomyelitis debridement, or high-energy trauma—traditional non-vascularized autografts suffer from poor incorporation, central necrosis, and high fracture rates. Free vascularized bone grafts (FVBG) circumvent these issues by transferring living bone with its intrinsic blood supply, allowing for primary osteogenesis rather than creeping substitution.
The Vascularized Fibula Graft
As outlined by Taylor, the free vascularized fibula is the workhorse of orthopaedic skeletal reconstruction.
Advantages of the Fibula Graft
- Single-Stage Reconstruction: Achieves immediate structural bridging of massive defects.
- Mechanical Stability: The graft can be "doweled" into the medullary canals of the recipient bone (e.g., tibia or femur) proximally and distally, providing excellent intrinsic stability during the anastomoses.
- Superior Strength: Tubular cortical bone is biomechanically stronger than an onlay cortical bone graft.
- Biological Vitality: Bleeding bone with intact endosteal and periosteal circulation is transferred, ensuring rapid union at the host-graft junctions.
- Fail-Safe Mechanism: Even if the microvascular anastomosis fails, the fibula may still function as a traditional, albeit non-vascularized, creeping cortical bone graft.
Disadvantages and Limitations
- Surgical Complexity: The procedure requires a prolonged operative time and advanced microsurgical expertise, limiting its application primarily to younger patients or those able to tolerate extended anesthesia.
- Elective Nature: It should be performed as an elective, meticulously planned procedure rather than in the acute trauma setting.
- Donor Site Morbidity: Harvest can cause problems at the knee and ankle, including valgus instability (if harvested too proximally in children) or ankle mortise widening (if the distal 6-8 cm is not preserved).
- Monitoring Challenges: The patency of the deeply buried bone anastomosis cannot be easily assessed postoperatively, unlike a cutaneous flap.
- Vessel Sacrifice: A major vessel (the peroneal artery) is sacrificed in the donor limb, necessitating preoperative angiography to ensure the foot has adequate supply from the anterior and posterior tibial arteries.
Anatomical Characteristics of the Fibula
- Morphology: Straight, dense cortical bone.
- Length: A massive graft, up to 26 cm in length, can be harvested from an adult.
- Composite Potential: Can be harvested with a muscle cuff (soleus/flexor hallucis longus), a proximal articular surface, and, in pediatric patients, a proximal physis for continued growth (requiring the anterior tibial artery pedicle).
- Vascular Pedicle: The peroneal artery (1.5 to 2.5 mm in diameter) and its two venae comitantes (2 to 3 mm in diameter). The pedicle length ranges from 1 to 5 cm.
- Surgical Approach: The dissection is relatively superficial and straightforward via a lateral approach.
- Complications: Minimal, provided the common peroneal nerve proximally and the tibial vessels distally are strictly protected.
- Limitation: Overlying skin and cutaneous nerves are generally unreliable or unavailable as a composite flap compared to other donor sites.
The Vascularized Iliac Crest Graft
The iliac crest is the preferred donor site when the defect requires a curved contour or a massive volume of cancellous bone, such as in pelvic ring reconstructions, complex periarticular defects, or mandibular reconstruction.
Anatomical Characteristics of the Iliac Crest
- Morphology: Curved, corticocancellous bone providing rich osteogenic potential.
- Length: A segment of 8 to 10 cm can be reliably harvested.
- Vascular Pedicle: Can be based on either the Superficial Circumflex Iliac Artery (SCIA, 0.5 to 3 mm diameter) or the Deep Circumflex Iliac Artery (DCIA). Venous drainage is via the superficial inferior epigastric veins (1.5 to 3 mm diameter). Pedicle length is 1 to 5 cm.
- Dissection Nuances: If the superficial vessels (SCIA) are used, the dissection is relatively superficial. However, if the deep vessels (DCIA) are chosen—which provide a more robust periosteal and endosteal blood supply—the dissection is deep, tedious, and requires careful division of the abdominal musculature.
- Composite Potential: Overlying skin and cutaneous nerves are readily available, making it an excellent osteocutaneous flap for extremity defects with concomitant soft tissue loss.
- Limitations: Muscle, articular surfaces, and physes are unavailable.
- Complications: Donor site morbidity is significant and includes the risk of abdominal wall herniation (requiring meticulous fascial closure or mesh reinforcement) and painful neuromas of the lateral femoral cutaneous nerve stump.
The Vascularized Rib Graft
While less commonly used in modern extremity reconstruction due to the superiority of the fibula, the vascularized rib graft retains specific indications, particularly in maxillofacial, spinal, and pediatric reconstructive surgery.
Anatomical Characteristics of the Rib
- Morphology: A curved, membranous, and highly flexible bone. Its malleability makes it ideal for contouring.
- Length: An extensive length of up to 30 cm may be obtained.
- Vascular Pedicle: Based on the posterior intercostal artery (1.5 to 2 mm in diameter) and the single intercostal vein.
- Surgical Considerations: Harvest requires a thoracotomy approach, carrying risks of pneumothorax and significant postoperative pain. However, it provides a long, vascularized strut that can be split or contoured to match complex three-dimensional defects.
CONCLUSION
The integration of free functioning muscle transfers and vascularized bone grafts into the orthopaedic armamentarium provides unparalleled solutions for limb salvage. Mastery of these techniques requires strict adherence to biomechanical principles—such as the Manktelow length-tension marking—and a profound respect for microvascular anatomy. Through meticulous preoperative planning, precise surgical execution, and rigorous postoperative rehabilitation, surgeons can restore both structural integrity and dynamic function to severely compromised extremities.
You Might Also Like
