Principles and Techniques of Tendon Transfers in the Upper Extremity
Key Takeaway
Tendon transfer surgery in the upper extremity restores critical motor function lost to peripheral nerve injury, tetraplegia, or neuromuscular disease. Successful outcomes rely on strict adherence to biomechanical principles, including matching muscle excursion, tension, and synergistic phase. This comprehensive guide details the indications, surgical approaches, and postoperative protocols for radial, median, and ulnar nerve palsies, providing orthopedic surgeons with evidence-based strategies for functional reconstruction.
Introduction to Tendon Transfers
The restoration of upper extremity function following irreparable peripheral nerve injury, brachial plexus trauma, or spinal cord injury (tetraplegia) represents one of the most profound applications of reconstructive orthopedic surgery. Pioneered by luminaries such as Sterling Bunnell, Paul Brand, and Joseph Boyes, tendon transfer surgery involves the detachment of a functioning muscle-tendon unit at its insertion and its re-routing to substitute for a paralyzed muscle.
This comprehensive guide synthesizes decades of evidence-based practice, detailing the biomechanical prerequisites, surgical indications, and operative techniques required to successfully execute tendon transfers for radial, median, and ulnar nerve palsies, as well as the tetraplegic upper limb.
Biomechanical Principles and Prerequisites
Successful tendon transfer surgery is unforgiving of poor planning. The surgeon must adhere strictly to established biomechanical principles to ensure predictable functional outcomes.
Prerequisites for Transfer
Before any tendon transfer is performed, the following clinical prerequisites must be met:
* Supple Joints: A tendon transfer cannot overcome a fixed joint contracture. Maximum passive range of motion (ROM) must be achieved preoperatively through therapy or surgical release.
* Tissue Equilibrium: The soft tissue bed must be free of acute inflammation, edema, or induration. Scars should be mature and pliable.
* Adequate Donor Strength: A muscle typically loses one grade of strength (on the MRC scale) following transfer. Therefore, only muscles with Grade 5 (normal) or Grade 4+ strength should be selected as donors.
* Expendability: The donor muscle must not result in an unacceptable loss of function at its native site.
Excursion and Amplitude
Muscle excursion (amplitude) is the distance a muscle can contract. A donor muscle must possess an excursion similar to that of the paralyzed muscle it replaces.
* Wrist flexors/extensors: ~33 mm of excursion.
* Finger extensors: ~50 mm of excursion.
* Finger flexors: ~70 mm of excursion.
Clinical Pearl: If a donor muscle lacks sufficient excursion, its effective amplitude can be augmented by utilizing the tenodesis effect of adjacent joints. For example, transferring a wrist flexor (33 mm excursion) to a finger extensor (50 mm excursion) is viable because active wrist flexion will passively augment finger extension.
Synergy and Phase
Muscles that work together during a specific motion are synergistic. Transferring a muscle in the same phase of motion (e.g., wrist extensors acting synergistically with finger flexors during grip) facilitates easier postoperative cortical re-education.
Straight Line of Pull
The transferred tendon should be routed as directly as possible from its origin to its new insertion. Acute angles or multiple pulleys increase friction, reduce mechanical efficiency, and risk tendon rupture or adhesion.
Radial Nerve Palsy Reconstruction
Radial nerve palsy results in the loss of wrist extension, finger extension at the metacarpophalangeal (MCP) joints, and thumb extension/abduction. The primary goal of reconstruction is to restore a stable wrist to facilitate power grip, followed by digital extension.
Indications and Timing
Tendon transfers are indicated for irreparable radial nerve injuries, or as early internal splinting while awaiting nerve recovery (e.g., Burkhalter's early pronator teres to extensor carpi radialis brevis transfer).
Standard Radial Nerve Transfer (The FDS Transfer / Boyes Technique)
While multiple variations exist, the standard transfer utilizes the following donor-recipient pairs:
1. Pronator Teres (PT) to Extensor Carpi Radialis Brevis (ECRB): Restores wrist extension. The ECRB is preferred over the ECRL to prevent radial deviation during extension.
2. Flexor Carpi Ulnaris (FCU) or Flexor Digitorum Superficialis (FDS) to Extensor Digitorum Communis (EDC): Restores finger extension.
3. Palmaris Longus (PL) to Extensor Pollicis Longus (EPL): Restores thumb extension.
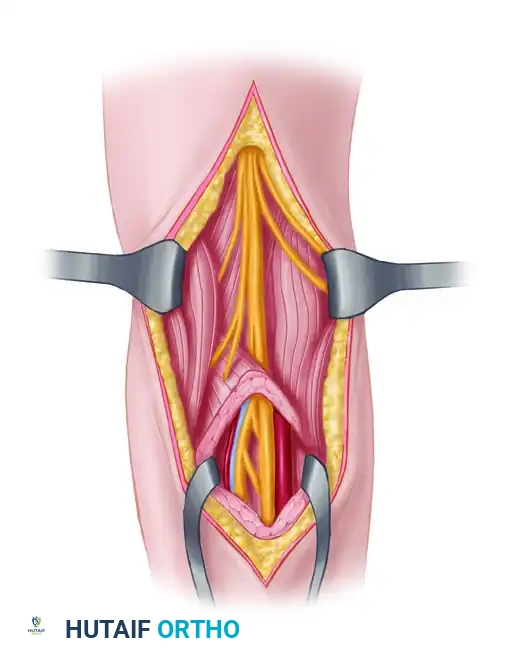
Surgical Technique: PT to ECRB and PL to EPL
- Positioning: Supine, arm on a hand table, tourniquet applied.
- Incision: A longitudinal incision is made over the mid-radial forearm to expose the PT insertion on the radius.
- Harvesting the PT: The PT is detached with a strip of periosteum to maximize length.
- Routing: The ECRB tendon is identified and mobilized. The PT is routed subcutaneously and woven into the ECRB.
- Thumb Extension (PL to EPL): The EPL is divided at the musculotendinous junction, rerouted out of Lister's tubercle (to prevent bowstringing and provide a straighter line of pull), and woven into the PL tendon.
- Tensioning: The wrist is held in 30 degrees of extension, and the thumb in full extension and slight abduction. The weaves are secured using a Pulvertaft technique with 3-0 braided non-absorbable sutures.
Surgical Warning: Over-tensioning the PT to ECRB transfer can lead to a fixed wrist extension contracture, severely impairing the patient's ability to flex the wrist and perform perineal care. Tension should be set so the wrist rests in neutral with gravity, but can be passively flexed.
Median Nerve Palsy and Opponensplasty
Low median nerve palsy results in the loss of thenar intrinsic musculature (abductor pollicis brevis, opponens pollicis, and the superficial head of the flexor pollicis brevis), leading to an inability to oppose the thumb. This severely compromises pinch and grasp.
Indications for Opponensplasty
Opponensplasty is indicated to restore palmar abduction and pronation of the thumb. The ideal transfer must pull from the direction of the pisiform to replicate the vector of the abductor pollicis brevis (APB).
The Camitz Transfer
Originally described for severe thenar atrophy secondary to end-stage carpal tunnel syndrome, the Camitz transfer utilizes the Palmaris Longus (PL).
* Technique: The PL is harvested with a distal strip of the palmar aponeurosis to provide adequate length. It is routed subcutaneously across the thenar eminence and inserted into the APB tendon or the radial aspect of the MCP joint capsule.
* Biomechanics: Because the PL is already located on the volar-ulnar aspect of the wrist, it provides excellent palmar abduction. However, it provides less pronation compared to transfers routed around the FCU.
The FDS Opponensplasty (Bunnell / Royle-Thompson)
For traumatic median nerve palsy, the FDS of the ring finger is a powerful donor.
* Technique: The FDS IV is harvested at the proximal phalanx, withdrawn into the distal forearm, and looped around the FCU tendon (which acts as a pulley). It is then routed subcutaneously to the thumb MCP joint and inserted into the APB insertion and the extensor hood.
* Advantage: Provides excellent strength and the perfect vector for true opposition (abduction and pronation).
The Huber Transfer
Utilizes the Abductor Digiti Minimi (ADM) transferred to the APB. This is particularly favored in pediatric patients with congenital thumb hypoplasia, as it restores thenar bulk and avoids sacrificing forearm tendons.
Ulnar Nerve Palsy and the Intrinsic-Minus Hand
Ulnar nerve palsy denervates the interossei and the ulnar two lumbricals, resulting in the classic "claw hand" deformity (hyperextension of the MCP joints and flexion of the IP joints) and a profound loss of key pinch strength (due to adductor pollicis paralysis).
Pathomechanics of the Claw Hand
The deformity is driven by the unopposed action of the Extensor Digitorum Communis (EDC) at the MCP joint and the Flexor Digitorum Profundus (FDP) at the IP joints.
Clinical Pearl: The Bouvier test is critical. If passively blocking the MCP joints in slight flexion allows the patient to actively extend the IP joints (Positive Bouvier), the central slip is intact, and surgery only needs to address MCP hyperextension.
Anti-Claw Procedures
The goal is to prevent MCP hyperextension, thereby allowing the EDC to transmit its force distally to extend the IP joints.
- Zancolli Lasso Procedure:
- The FDS of the affected fingers (usually ring and small) is divided at the proximal phalanx.
- The tendon is looped around the A1 pulley and sutured back onto itself.
- This creates a static tenodesis that flexes the MCP joint, preventing hyperextension.
- Brand Transfer (ECRL/ECRB to Intrinsics):
- A dynamic transfer utilizing a wrist extensor extended with a free tendon graft (e.g., plantaris or fascia lata).
- The grafts are routed through the intermetacarpal spaces volar to the deep transverse metacarpal ligament and inserted into the lateral bands.
Restoration of Key Pinch
To restore the function of the Adductor Pollicis, the ECRB or FDS of the middle finger can be transferred.
* Smith's Transfer: The ECRB is prolonged with a tendon graft, routed through the second intermetacarpal space, and inserted into the adductor tubercle of the thumb.
Tendon Transfers in Tetraplegia
Surgical rehabilitation of the upper limb in cervical spinal cord injury (tetraplegia) is highly specialized. The goals are to restore elbow extension, wrist extension, key pinch, and grasp, depending on the level of the injury (classified by the International Classification for Surgery of the Hand in Tetraplegia).
Restoration of Elbow Extension
Loss of triceps function (C5/C6 level) severely limits the patient's ability to transfer from a wheelchair or reach overhead.
* Posterior Deltoid to Triceps Transfer (Moberg): The posterior third of the deltoid is mobilized and extended with fascia lata or a tibialis anterior allograft, then woven into the triceps tendon.
* Biceps to Triceps Transfer: An alternative if the deltoid is weak, provided the brachialis is strong enough to maintain elbow flexion.
Restoration of Key Pinch and Grasp
- Brachioradialis (BR) to Flexor Pollicis Longus (FPL): The BR is a workhorse in tetraplegia. It is transferred to the FPL to restore lateral (key) pinch. Extensive mobilization of the BR to its proximal neurovascular pedicle is required to achieve the necessary 30 mm of excursion.
- ECRL to FDP: If the patient has both ECRB and ECRL (Group 2 or higher), the ECRL can be transferred to the FDP tendons to restore active finger flexion (grasp).
Surgical Execution: The Pulvertaft Weave
The mechanical integrity of the tendon transfer relies on the surgical connection. The Pulvertaft weave is the gold standard for joining tendons of unequal or equal diameter.
- Preparation: The recipient tendon is slit longitudinally using a #15 blade.
- First Pass: The donor tendon is passed through the slit. Tension is provisionally set.
- Subsequent Passes: The donor tendon is woven back and forth through the recipient tendon at 90-degree alternating angles for a minimum of three to four passes.
- Suturing: Each pass is secured with a core suture of 3-0 or 4-0 braided non-absorbable material (e.g., Ethibond or Ticron). A running epitendinous suture (e.g., 5-0 Prolene) can be added to smooth the construct and reduce adhesions.
Surgical Warning: The strength of the Pulvertaft weave comes from the multiple passes and the friction between the tendons, not just the sutures. Ensure the weaves are tight and the tendon ends are buried to prevent catching on surrounding paratenon or fascia.
Postoperative Rehabilitation
The success of a tendon transfer is equally dependent on meticulous surgical technique and rigorous postoperative rehabilitation.
Phase 1: Immobilization (0-3 Weeks)
The limb is immobilized in a custom orthosis that removes all tension from the transfer. For example, following a radial nerve transfer, a long-arm cast or rigid splint is applied with the wrist in 30-45 degrees of extension, MCP joints in neutral, and the thumb in maximum extension and abduction.
Phase 2: Early Protected Motion (3-6 Weeks)
The rigid cast is replaced with a removable thermoplastic splint.
* Active motion of the transferred muscle is initiated within the safe zone.
* Passive motion in the direction of the transfer is permitted.
* Strict avoidance of passive stretching against the transfer is enforced to prevent elongation of the healing weave.
Phase 3: Cortical Re-education and Strengthening (6-12 Weeks)
Biofeedback and mirror therapy are utilized to help the patient isolate the new function of the transferred muscle. For instance, a patient with a PT to ECRB transfer must be trained to attempt forearm pronation to achieve wrist extension. Resistance exercises are gradually introduced after 8 weeks, once the tendon weave has achieved sufficient tensile strength.
Conclusion
Tendon transfer surgery remains a cornerstone of reconstructive orthopedics for the paralyzed upper extremity. By mastering the biomechanical principles of excursion, tensioning, and synergistic phase, and by executing precise surgical techniques such as the Pulvertaft weave, the orthopedic surgeon can predictably restore critical functions—transforming a severely compromised limb into a functional tool for activities of daily living. Strict adherence to postoperative protocols ensures the longevity and efficacy of these elegant reconstructive procedures.
📚 Medical References
- Tendon transfers in surgery of the rheumatoid hand, Hand Clin 4:309, 1988.
- Mannerfelt L, Malmsten M: Arthrodesis of the wrist in rheumatoid arthritis: a technique without external fi xation, Scand J Plast Reconstr Surg 5:124, 1971.
- Mikkelsen OA: Arthrodesis of the wrist joint in rheumatoid arthritis, Hand 12:149, 1980.
- Millender LH, Nalebuff EA: Arthrodesis of the rheumatoid wrist: functional evaluation of a modifi ed technique, Orthop Rev 1:13, 1972.
- Nalebuff EA, Garrod KJ: Present approach to the severely involved rheumatoid wrist, Orthop Clin North Am 15:368, 1984.
- Wrist Arthroplasty Albright JA, Chase RA: Palmar-shelf arthroplasty of the wrist in rheumatoid arthritis: a report of nine cases, J Bone Joint Surg 52A:896, 1970.
- Beckenbaugh RD: Total joint arthroplasty—the wrist, Mayo Clin Proc 54:513, 1979.
- Beckenbaugh RD, Linscheid RL: Arthroplasty in the hand and wrist. In Green DP, ed: Operative hand surgery, 2nd ed, New York, 1988, Churchill Livingstone. Biyani A, Simison JM: Fibrous stabilization of the rheumatoid wrist, J Hand Surg 20B:143, 1995.
- Carlson JR, Simmons BP: Total wrist arthroplasty, J Am Acad Orthop Surg 6:308, 1998.
- Cobb TK, Beckenbaugh RD: Biaxial long-stemmed multipronged distal components for revision/bone defi cit total-wrist arthroplasty, J Hand Surg 21A:764, 1996.
- Cobb TK, Beckenbaugh RD: Biaxial total wrist arthroplasty, J Hand Surg 21A:1011, 1996.
- Comstock CP, Louis DS, Eckenrode JF: Silicone wrist implant: long-term follow-up study, J Hand Surg 13A:201, 1988.
- Cooney WP III, Beckenbaugh RD, Linscheid RL: Total wrist arthroplasty: problems with implant failure, Clin Orthop Relat Res 187:121, 1984.
- Courtman NH, Sochart DH, Trail IA, et al: Biaxial wrist replacement: initial results in the rheumatoid patient, J Hand Surg 24B:32, 1999.
- Divelbiss BJ, Sollerman C, Adams BD: Original communications. Early results of the universal total wrist arthroplasty in rheumatoid arthritis, J Hand Surg 27A:195, 2002.
- Fatti JF, Palmer AK, Greenky S, et al: Long-term results of Swanson interposition wrist arthroplasty: II, J Hand Surg 16A:432, 1991.
- Ferlic DC: Implant arthroplasty of the rheumatoid wrist, Hand Clin 3:169, 1987.
- Ferlic DC, Clayton ML, Mills MF:
You Might Also Like