Congenital Hand Reconstruction: Apert Syndrome & Polydactyly

Key Takeaway
Surgical management of congenital hand anomalies requires a profound understanding of altered biomechanics and pathoanatomy. This comprehensive guide details the staged reconstruction of the complex syndactyly seen in Apert syndrome, alongside evidence-based protocols for managing preaxial polydactyly. From the Flatt technique for border digit release to the Bilhaut-Cloquet procedure for bifid thumbs, master the critical steps to optimize functional and aesthetic outcomes in pediatric hand surgery.
RECONSTRUCTION OF THE HAND IN APERT SYNDROME
Apert syndrome (acrocephalosyndactyly type I) is a rare autosomal dominant disorder characterized by craniosynostosis, midface hypoplasia, and complex, symmetric syndactyly of the hands and feet. The hand deformity is uniquely challenging, often presenting as a "mitten" or "rosebud" hand due to complex syndactyly involving both soft tissue and osseous synostosis of the central digits.
The primary goal of surgical intervention is to provide a functional, sensate hand with a prehensile pinch and grasp. Because there is an absolute deficiency of skin, attempting to reconstruct a five-digit hand often results in severe scar contractures, compromised vascularity, and stiff, non-functional digits. The Flatt approach advocates for the creation of a functional three-fingered hand (plus a thumb) by sacrificing the central (long) digit to provide adequate soft tissue coverage for the adjacent index and ring fingers.
Stage I: Release of the Border Digits
Stage I focuses on liberating the border digits (the thumb and the small finger) to establish early grasp and pinch mechanics. This stage is strictly indicated before the child reaches 1 year of age to facilitate normal motor development and cortical mapping.
Surgical Pearl: Early release of the border digits is critical. Delaying this stage beyond 12 months can lead to irreversible angular deformities due to the differential growth rates between the tethered digits.
Surgical Technique (Flatt Approach - Stage I)
- Preparation and Positioning: The patient is positioned supine with the arm extended on a radiolucent hand table. A pediatric pneumatic tourniquet is applied to the proximal arm and inflated after exsanguination.
- Incision Design: Incise the border syndactylies utilizing the dorsal and volar zigzag flap techniques described by Bauer et al. This approach releases the small, ring, and index fingers, as well as the thumb.
- Thumb Web Space Deepening: The first web space is often severely contracted. If the thumb is not directly incorporated into the complex syndactyly mass, the web space must be deepened aggressively. Utilize a four-part Z-plasty (or a dorsal rotational flap) to release the adduction contracture.
- Neurovascular Dissection: Carefully identify and protect the neurovascular bundles. In Apert syndrome, the neurovascular anatomy is frequently anomalous, with distal bifurcations that may require microvascular separation.
- Closure and Grafting: Close the interdigitating skin flaps with fine absorbable interrupted sutures (e.g., 5-0 or 6-0 chromic gut). Because of the inherent skin deficiency, primary closure is rarely sufficient. Cover all remaining secondary defects with full-thickness skin grafts (FTSG) harvested from the groin or lower abdomen to minimize secondary contracture.
Stage II: Central Digit Management
Stage II is performed 6 to 9 months following Stage I. This interval is mandatory to allow for complete revascularization, graft maturation, and softening of the previously operated tissues.
Surgical Technique (Flatt Approach - Stage II)
- Flap Design: Make precise incisions on the long finger to create robust fasciocutaneous flaps, as described by Bauer et al. The objective is to harvest all viable skin overlying the middle digit.
- Digital Amputation: After the flaps are elevated and the neurovascular bundles to the long finger are ligated, amputate the long digit at the level of the metacarpophalangeal (MCP) joint.
- Commissure Reconstruction: Utilize the harvested overlying skin from the amputated long finger to reconstruct the new commissure between the index and ring fingers. This tissue is also used to provide tension-free coverage for the medial aspect of the index finger and the lateral aspect of the ring finger.
- Closure: Close the flaps in a routine, tension-free fashion. If residual defects persist despite the use of the long finger skin, supplement with additional full-thickness skin grafts.
- Immobilization: Apply sterile dressings consisting of moistened cotton batting carefully packed between the newly created webs to prevent maceration and maintain separation. Apply a long-arm plaster splint to maintain the digits in extension and the thumb in abduction.
Postoperative Care
The splint and bulky dressings are maintained for exactly 4 weeks. Following cast removal, active motion of the hand is aggressively encouraged, often requiring the involvement of a specialized pediatric hand occupational therapist to maximize functional integration.
DUPLICATION (POLYDACTYLY) OF THE HAND
Polydactyly is one of the most common and conspicuous congenital anomalies of the upper extremity, with an incidence of 9,000 to 10,000 new cases recorded annually. The condition is broadly classified into three main anatomical categories:
1. Preaxial Polydactyly: Duplication of the thumb (bifid thumb).
2. Central Polydactyly: Duplication involving the index, long, or ring fingers (often associated with syndactyly).
3. Postaxial Polydactyly: Duplication of the small finger (most common in populations of African descent).
A highly complex and exceedingly rare variant included in this category is ulnar dimelia, or "mirror hand," characterized by duplication of the ulna, absence of the radius, and multiple postaxial digits.
PREAXIAL POLYDACTYLY (BIFID THUMB)
Preaxial polydactyly, or the bifid thumb, represents a complete or partial duplication of the first ray. It is the most common duplication pattern observed in white and Asian populations, occurring in approximately 1 per 3,000 live births.
Etiology and Genetics
The exact etiology of the sporadic bifid thumb remains elusive, though it is largely attributed to environmental factors affecting the apical ectodermal ridge during embryogenesis. Experimental models have successfully reproduced preaxial polydactyly in the offspring of rats via the administration of cytarabine during pregnancy.
While typically an isolated, unilateral deformity, when thumb duplication is associated with a triphalangeal thumb, an autosomal dominant inheritance pattern (often linked to the ZRS enhancer of the SHH gene) is frequently identified. Visceral anomalies are rare but must be ruled out; the presence of a bifid thumb warrants screening for hand-heart syndromes, most notably Holt-Oram syndrome.
Wassel Classification
The Wassel classification system is the universally accepted framework for categorizing thumb polydactyly, based on the level of skeletal duplication from distal to proximal.
- Type I: Partial duplication of the distal phalanx with a common epiphysis.
- Type II: Complete duplication of the distal phalanx, including its epiphysis.
- Type III: Duplication of the distal phalanx and bifurcation of the proximal phalanx.
- Type IV: Complete duplication of both the distal and proximal phalanges. (Most common)
- Type V: Complete duplication of the distal and proximal phalanges with bifurcation of the metacarpal.
- Type VI: Complete duplication of the distal and proximal phalanges, as well as the metacarpal.
- Type VII: Variable degrees of duplication associated with a triphalangeal thumb.
In Wassel’s original series, Type IV was the most prevalent pattern (47%), followed by Type VII (20%) and Type II (15%). Wood later expanded on this, noting that Type IV and Type VII deformities require further subdivision based on the exact extent of triphalangism and soft tissue tethering.
Clinical and Biomechanical Presentation
The clinical appearance of a bifid thumb ranges from a mildly broadened thumb tip to a completely duplicated, fully formed digit.


(Clinical presentation of a Wassel Type II Bifid Thumb, demonstrating divergence at the interphalangeal joint).


(Clinical presentation of a Wassel Type IV Bifid Thumb, the most common variant, showing complete duplication of the proximal and distal phalanges).
Pathoanatomy:
* Hypoplasia: Both duplicates are typically hypoplastic compared to a normal contralateral thumb. The radial duplicate is almost universally more hypoplastic than the ulnar duplicate.
* Tendon Eccentricity: The extrinsic flexor (FPL) and extensor (EPL) tendons are frequently bifurcated or eccentrically inserted, leading to a classic zigzag deformity.
* Intrinsic Muscle Anomalies: The ulnar-innervated intrinsic muscles (adductor pollicis, deep head of flexor pollicis brevis) typically insert onto the ulnarmost duplicate. Conversely, the median-innervated intrinsics (abductor pollicis brevis, opponens pollicis, superficial head of FPB) insert onto the radialmost duplicate.
* Ligamentous Sharing: The collateral ligaments of the duplicated joints are often shared, creating a severe insufficiency in the interdigital space once the supernumerary digit is excised.
Surgical Warning: Simple amputation of the hypoplastic radial digit is strictly contraindicated. Failure to reconstruct the collateral ligaments and centralize the eccentric tendons will inevitably result in progressive angular deformity (Z-collapse) and joint instability.
Surgical Management
Surgical correction is almost always indicated to improve both cosmesis and prehensile function. Reconstruction is optimally performed when the child is between 12 and 18 months of age, allowing for sufficient anatomical growth to facilitate meticulous tissue handling while preceding the development of fine motor pinch patterns.
The Bilhaut-Cloquet Procedure (For Types I and II)
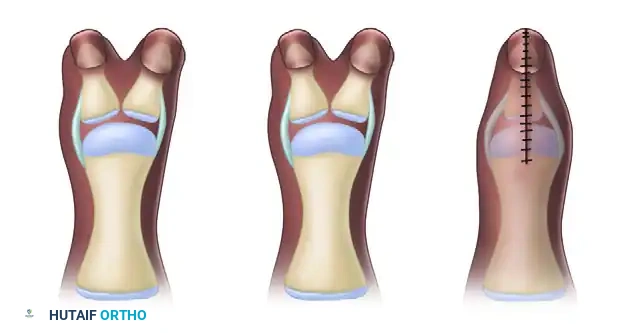
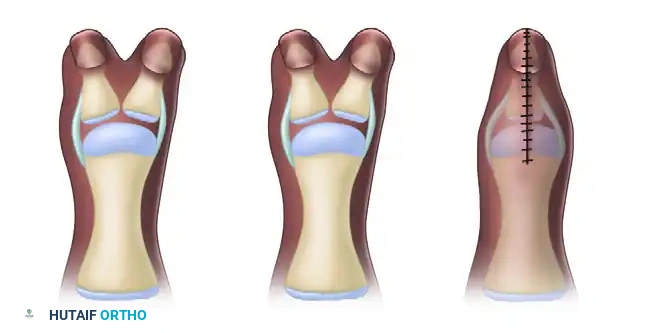
For Wassel Type I and symmetrical Type II bifid thumbs presenting with a conjoined nail, the Bilhaut-Cloquet combination procedure is highly effective. This technique involves excising the central wedge of bone and soft tissue and combining the lateral halves to form a single, appropriately sized thumb.

(A) Bilhaut-Cloquet technique for symmetrical thumb duplication.

(B) Planned central wedge resection.

(C) Wedge-shaped portion of central soft tissue and osseous structures removed.

(D) Final closure, demonstrating the combined extra-articular structures.
Clinical Execution:
(Preoperative marking of the planned central wedge resection).
(Intraoperative view following the excision of the central osseous and soft tissue wedge, preparing for approximation).
While the Bilhaut-Cloquet procedure provides excellent skeletal alignment, it carries a high risk of postoperative nail ridging (due to germinal matrix scarring) and potential physeal growth arrest if the epiphyseal plates are not perfectly aligned.
The Baek Modification
To mitigate the risk of physeal arrest inherent in the classic Bilhaut-Cloquet procedure, Baek et al. introduced a critical modification for Wassel Type II thumbs.


(Baek et al. modified Bilhaut-Cloquet procedure. The shaded area is resected, preserving one entire epiphysis with a portion of its diaphysis to prevent growth arrest).
By preserving the entire epiphysis of the dominant (usually ulnar) duplicate and combining the diaphyseal segments extra-articularly, longitudinal growth is safeguarded while still achieving a cosmetically acceptable thumb width.
Reconstruction of Proximal Duplications (Types III - VI)
More proximal duplications (Wassel Types III through VI) require a comprehensive reconstructive approach rather than a combination procedure. The standard protocol involves the ablation of the more hypoplastic digit (almost always the radial duplicate) and the reconstruction of the retained ulnar digit.
Key Surgical Steps:
1. Incision and Exposure: A racquet-shaped incision is made around the base of the radial duplicate, incorporating a zig-zag extension along the radial border of the retained ulnar thumb.
2. Intrinsic Muscle Transfer: The abductor pollicis brevis (APB) inserting into the radial duplicate is carefully detached with a periosteal sleeve. Following ablation of the radial digit, the APB is advanced and sutured into the radial aspect of the proximal phalanx of the retained ulnar thumb to restore abduction and opposition.
3. Ligamentous Reconstruction: The radial collateral ligament (RCL) of the MCP joint is frequently deficient. It must be reconstructed using a periosteal flap harvested from the excised radial digit or by advancing the joint capsule.
4. Tendon Centralization: The FPL and EPL tendons must be inspected. If they insert eccentrically, they must be centralized. This may require releasing the tendon insertions and reattaching them centrally on the distal phalanx, or performing a corrective closing-wedge osteotomy of the phalanx to realign the skeletal axis beneath the tendons.
5. Articular Contouring: The widened metacarpal head (in Type IV) must be shaved down longitudinally to match the articular base of the retained proximal phalanx, preventing late subluxation.
Complications and Salvage Procedures
Despite meticulous surgical technique, late angular deformity and joint instability remain the most frequent complications, particularly in Wassel Types IV, V, VI, and VII.
Z-Collapse Deformity:
Eccentric tendon forces or unrecognized collateral ligament insufficiency can lead to a progressive Z-collapse (MCP joint hyperextension and IP joint flexion, or vice versa).
Miura's Corrective Technique:
Miura described a highly effective salvage procedure for late Z-collapse at the thumb interphalangeal joint. This involves:
* A rotational skin flap on the concave side of the deformity to release the skin contracture.
* Excision of the radial half of the extensor tendon.
* Transfer of the flexor tendon into the ulnar side of the distal phalanx to dynamically correct the angulation.
* Concurrent closing-wedge osteotomies may be required if fixed osseous deformity is present.
Other reported complications include superficial infection, hypertrophic scar contracture, joint stiffness, inadequate tendon excursion, and a narrowed first web space. However, loss of sensibility or digit viability is exceedingly rare when meticulous microsurgical principles and tourniquet protocols are strictly observed. Overall, while the reconstructed thumb may possess a slightly narrowed nail compared to the contralateral side, functional outcomes and parental satisfaction remain high when angular deformities are successfully prevented.
You Might Also Like

