Operative Management of the Paralytic Hand: Principles and Tendon Transfers
Key Takeaway
The paralytic hand presents a complex biomechanical challenge characterized by the loss of synergistic muscle balance, leading to profound functional deficits such as the intrinsic minus deformity. Successful surgical reconstruction relies on meticulous preoperative planning, restoration of joint suppleness, and the strategic execution of synergistic tendon transfers to restore essential functions including pinch, grasp, and hook. This guide details the operative management and rehabilitation protocols for restoring hand kinematics.
Introduction to the Paralytic Hand
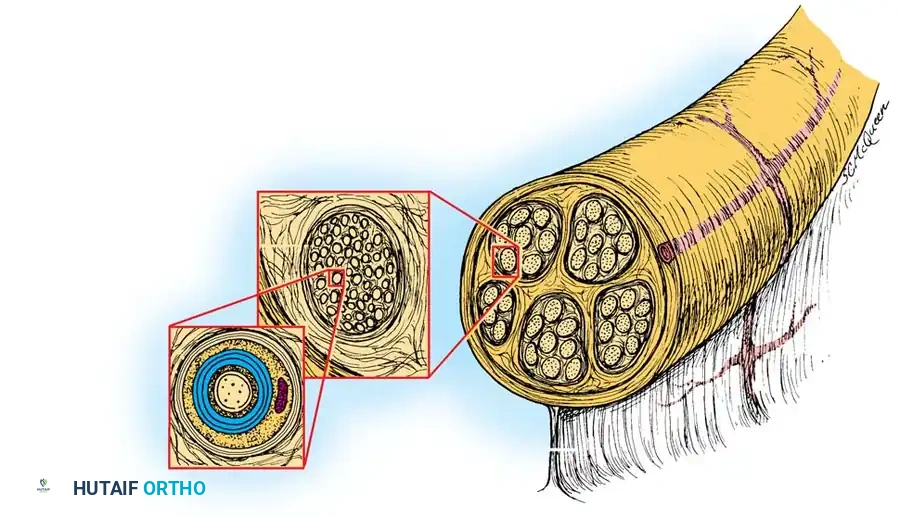
The human hand is a structure of tremendous sensibility and intricate biomechanical design. However, tactile feedback alone is insufficient for function; purposeful motion and dynamic strength are absolute prerequisites for the highly adaptive functions of pinch, grasp, and hook. The kinematic chain of the hand, wrist, and forearm relies on the precise articulation of 29 bones, mobilized and stabilized by an intricate network of 50 muscles acting as motors and dynamic restraints.
To achieve purposeful motion, joint movement must be exquisitely controlled. Joints crossed by moving tendons must be stabilized by balanced antagonistic muscles. When a major motor unit in the hand is paralyzed—whether due to peripheral nerve injury, brachial plexus trauma, spinal cord injury (tetraplegia), or systemic neuropathies (e.g., Hansen’s disease)—the delicate equilibrium of the hand is catastrophically disrupted. The resulting condition, broadly termed the "paralytic hand," requires profound anatomical knowledge and meticulous surgical planning to reconstruct.
Biomechanics and Synergistic Muscle Function
An outstanding example of dynamic stabilization in the normal hand is the maintenance of wrist extension by the extensor carpi radialis brevis (ECRB), extensor carpi radialis longus (ECRL), and extensor carpi ulnaris (ECU). These extensors prevent the wrist from being pulled into flexion by the powerful extrinsic finger flexors when a forceful fist is made. Conversely, the antagonists of the wrist extensors—the wrist flexors—contribute to the stabilization of the wrist during forceful digital extension.
In a physiologically normal hand, the transition from one stable position to another is rhythmic and fluid. Muscle groups act in proper phase, cooperating with one another through unconscious proprioceptive feedback and conscious effort. Patterns of muscle group movement that act in endless, coordinated repetition are termed synergistic.
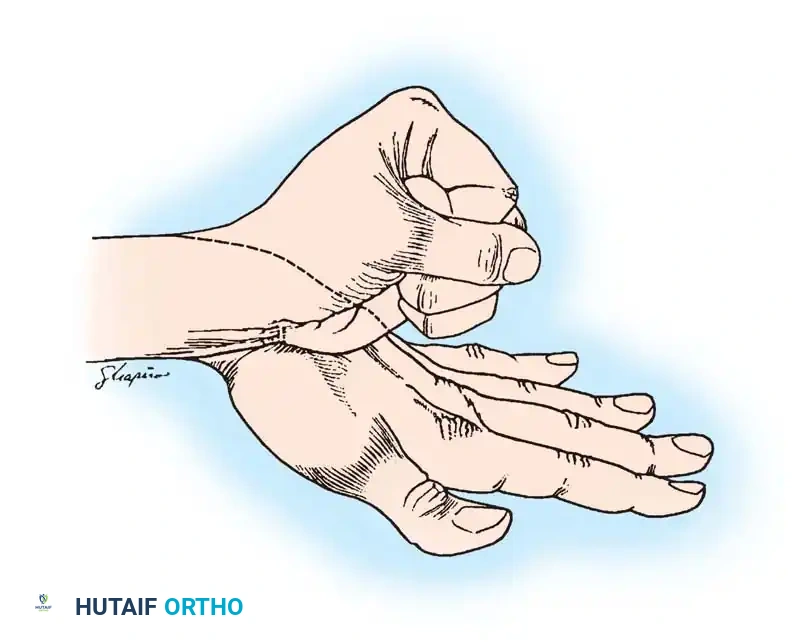
Fig 1: Synergistic muscles of the hand. The wrist extensors, finger flexors, and digital adductors act together in a coordinated kinematic chain.
The Rules of Synergy
- Flexion Synergy: The wrist extensors, finger flexors, and digital adductors act together with ease.
- Extension Synergy: The wrist flexors, finger extensors, and digital abductors are synergistic.
Beginning with the wrist flexed and the fingers extended and abducted, the wrist can be extended and the fingers flexed, returning to the original position with effortless fluidity. However, attempting to flex the wrist and fingers simultaneously involves slower, awkward movements that require conscious cortical override.
Clinical Pearl: In treating muscle imbalance via tendon transfer, the surgeon's first choice for a donor tendon should always be a muscle that is normally synergistic with the weakened or paralyzed muscle. Synergistic transfers require significantly less postoperative cortical re-education and yield more predictable functional outcomes.
Pathophysiology of Muscle Imbalance
When a major muscle in the hand is paralyzed, the loss of direct motor power is only the primary deficit. The secondary, and often more debilitating, consequence is the disruption of the hand's resting balance.
Any muscle whose antagonist is paralyzed will contract unopposed. Over time, this unopposed resting tone leads to myostatic contracture of the muscle and secondary capsular contractures of the joints it crosses. While contractures may occasionally increase the passive stability of a flail hand, they overwhelmingly increase its functional disability.
The Intrinsic Minus (Clawhand) Deformity
The most dramatic and classic presentation of muscle imbalance is the intrinsic minus, or clawhand, deformity, resulting from paralysis of the intrinsic muscles (interossei and lumbricals).
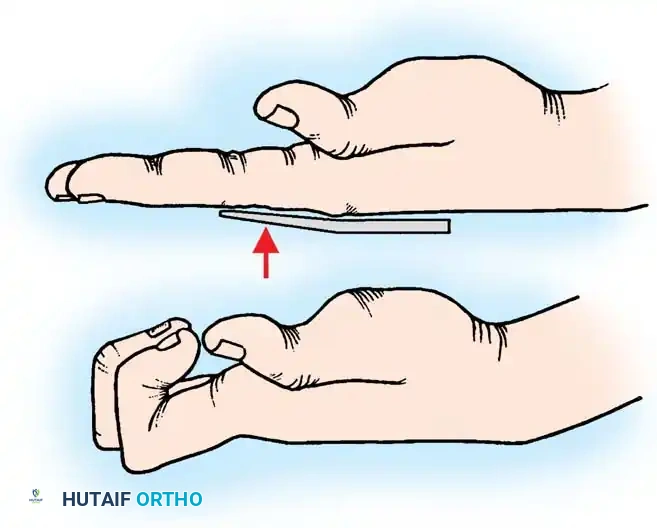
Fig 2: Clawing of the hand caused by paralysis of intrinsic muscles. (A) The long finger extensors cannot extend the interphalangeal joints because the metacarpophalangeal joints are hyperextended. (B) When MCP hyperextension is prevented, the long extensors can successfully extend the IP joints.
Biomechanics of the Clawhand:
Paralysis of the intrinsic metacarpophalangeal (MCP) joint flexors and interphalangeal (IP) joint extensors leads to unopposed MCP joint extension by the extrinsic digital extensors (EDC) and IP joint flexion by the extrinsic digital flexors (FDP and FDS).
Because the EDC inserts primarily on the proximal phalanx, its unopposed pull hyperextends the MCP joint. Once the MCP joint hyperextends, the EDC's line of pull shifts dorsal to the joint's axis of rotation, rendering it mechanically incapable of transmitting extensor force to the proximal and distal interphalangeal (PIP and DIP) joints. Consequently, the IP joints remain flexed by the resting tone of the extrinsic flexors.
Furthermore, the wrist is eventually pulled into flexion by the strong finger flexors. This wrist flexion creates a tenodesing effect on the long finger extensors, which exacerbates the hyperextension of the MCP joints.
Thumb Involvement in Intrinsic Paralysis:
The thumb is profoundly affected. It is pulled into adduction by the extensor pollicis longus (EPL), which is unopposed by the paralyzed intrinsic muscles of opposition and abduction (abductor pollicis brevis, opponens pollicis). This adducted posture is accompanied by extension of the carpometacarpal (CMC) joint, increasing tension on the flexor pollicis longus (FPL) tendon. The IP joint of the thumb falls into flexion because the FPL is unopposed by the paralyzed intrinsic IP joint extensors (adductor pollicis and abductor pollicis brevis).
Surgical Warning: Never perform a tendon transfer on a hand with fixed joint contractures. The primary prerequisite for any tendon transfer is a supple joint. Preoperative serial casting, dynamic splinting, or surgical release (e.g., capsulotomy) must be completed before tendon transfer is attempted.
Etiology of the Paralytic Hand
The surgical approach to the paralytic hand must be tailored to the underlying etiology, as the presence or absence of sensation and the potential for spasticity drastically alter the surgical algorithm.
- Poliomyelitis: Sensation is entirely normal. The paralysis is purely motor, flaccid, and non-progressive.
- Peripheral Nerve Lesions: Sensation is variable depending on the specific nerve (Radial, Median, Ulnar) and the level of the lesion.
- Hansen’s Disease (Leprosy): Sensation is absent, often in a glovelike distribution. Patients are at high risk for unrecognized trauma and ulceration.
- Syringomyelia: Sensation is dissociated (loss of pain and temperature with preserved light touch and proprioception).
- Cerebral Palsy / Upper Motor Neuron Lesions: Characterized by spasticity. Muscle tension is constantly or intermittently increased, leading to dynamic imbalances that can cause severe joint subluxation or dislocation. Tendon transfers in spastic hands are highly unpredictable and require specialized algorithms.
Core Principles of Tendon Transfer
Before executing any tendon transfer, the orthopedic surgeon must adhere to strict biomechanical and physiological principles:
- Tissue Equilibrium: The soft tissue bed must be completely healed. There should be no active inflammation, edema, or induration. Tendons routed through scarred beds will inevitably form adhesions.
- Joint Suppleness: As previously stated, all joints to be moved by the transferred tendon must have full passive range of motion.
- Donor Muscle Strength: A muscle loses approximately one grade of strength (on the MRC 0-5 scale) following transfer. Therefore, only muscles with a preoperative strength of Grade 4 or 5 should be utilized as donors.
- Amplitude of Excursion: The donor tendon must possess an excursion amplitude similar to the paralyzed muscle it is replacing. For example, wrist flexors/extensors have an excursion of ~33 mm, while finger flexors have an excursion of ~70 mm.
- Straight Line of Pull: The transferred tendon should be routed as directly as possible to its new insertion. Acute angles or multiple pulleys decrease mechanical efficiency and increase friction.
- One Tendon, One Function: A single transferred tendon cannot be expected to perform multiple, disparate functions simultaneously.
Surgical Management of Specific Nerve Palsies
Radial Nerve Palsy
Radial nerve palsy results in the loss of wrist extension, finger extension at the MCP joints, and thumb extension/abduction. The hand is severely disabled due to the inability to stabilize the wrist for a forceful grip.
Standard Transfer Algorithm (Modified Boyes or Jones):
* Wrist Extension: Pronator Teres (PT) transferred to the Extensor Carpi Radialis Brevis (ECRB). The ECRB is preferred over the ECRL because its central insertion on the third metacarpal provides pure wrist extension without radial deviation.
* Finger Extension: Flexor Carpi Ulnaris (FCU) or Flexor Carpi Radialis (FCR) transferred to the Extensor Digitorum Communis (EDC).
* Thumb Extension: Palmaris Longus (PL) transferred to the Extensor Pollicis Longus (EPL). The EPL is typically rerouted out of Lister's tubercle and transposed radially to provide both extension and abduction.
Low Ulnar Nerve Palsy
Low ulnar nerve palsy paralyzes the interossei, the ulnar two lumbricals, the adductor pollicis, and the deep head of the FPB. This results in a classic claw deformity of the ring and small fingers, profound weakness of key pinch (Froment's sign), and loss of finger abduction/adduction.
Surgical Correction of Ulnar Clawing:
The goal is to prevent MCP hyperextension, thereby allowing the extrinsic EDC to extend the IP joints.
* Zancolli Lasso Procedure: The Flexor Digitorum Superficialis (FDS) of the affected fingers is divided at its insertion, looped around the A1 pulley, and sutured back onto itself. This creates a dynamic tenodesis that flexes the MCP joint.
* Modified Stiles-Bunnell Transfer: A donor tendon (e.g., FDS of the middle finger or ECRB prolonged with tendon grafts) is routed volar to the deep transverse metacarpal ligament and inserted into the lateral bands of the extensor mechanism.
Restoration of Key Pinch (Adductorplasty):
* The ECRB or FDS (ring finger) can be transferred to the insertion of the adductor pollicis on the proximal phalanx of the thumb. If the ECRB is used, it must be prolonged with a tendon graft and routed through the second intermetacarpal space.
Low Median Nerve Palsy
The hallmark of low median nerve palsy is the loss of thumb opposition due to paralysis of the abductor pollicis brevis, opponens pollicis, and superficial head of the FPB. The thumb rests in the plane of the palm (simian hand).
Restoration of Opposition (Opponensplasty):
To restore opposition, the transferred tendon must pull the thumb in palmar abduction, pronation, and flexion. The ideal vector of pull is directed toward the pisiform.
* FDS Transfer (Burkhalter/Bunnell): The FDS of the ring finger is harvested, looped around the FCU tendon (which acts as a pulley), and routed subcutaneously across the palm to insert on the APB tendon and the dorsal capsule of the thumb MCP joint.
* Extensor Indicis Proprius (EIP) Transfer (Burkhalter): The EIP is harvested at the index MCP joint, withdrawn at the wrist, and routed subcutaneously around the ulnar border of the wrist (using the extensor retinaculum as a pulley) to insert on the thumb. This avoids sacrificing a flexor tendon.
Management of the Tetraplegic Hand
Severe paralysis resulting from cervical spinal cord injury (tetraplegia) presents a unique reconstructive challenge. The goal is not to restore a "normal" hand, but to provide functional independence through the restoration of key pinch and grasp.
Classification and Evaluation
The International Classification for Surgery of the Hand in Tetraplegia is based on the number of sensate, motor-functioning muscle groups available below the elbow (graded MRC 4 or 5).
* Group 0: No muscles available.
* Group 1: Brachioradialis (BR) available.
* Group 2: BR, ECRL available.
* Group 3: BR, ECRL, ECRB available.
* Group 4: BR, ECRL, ECRB, PT available.
Principles of Tetraplegia Reconstruction
- Elbow Extension: Restoration of triceps function is paramount. Without elbow extension, the patient cannot reach overhead or propel a wheelchair effectively. The posterior deltoid is commonly transferred to the triceps insertion using a fascia lata or tendon graft.
- Wrist Extension: If the ECRB is paralyzed but the BR is functional (Group 1), the BR is transferred to the ECRB to provide active wrist extension. This is critical, as active wrist extension allows for passive finger flexion via the tenodesis effect.
- Key Pinch: In Group 2 or 3 patients, the BR or PT can be transferred to the FPL to restore active thumb flexion against the index finger.
- Active Grasp: In higher-functioning patients (Group 4), the ECRL can be transferred to the FDP to provide active finger flexion, while the PT is transferred to the FPL for pinch.
Postoperative Rehabilitation Protocols
The success of a tendon transfer is equally dependent on the surgical execution and the postoperative rehabilitation.
Phase 1: Immobilization (0-3 or 4 weeks)
The hand and wrist are immobilized in a custom orthosis that removes all tension from the transferred tendon. For example, following an opponensplasty, the thumb is immobilized in maximum palmar abduction and opposition.
Phase 2: Early Protected Motion (3-6 weeks)
The cast is removed, and a removable thermoplastic splint is fabricated. Active, gravity-eliminated motion is initiated. The patient is instructed to fire the donor muscle. Biofeedback and mirror therapy are highly effective during this phase to facilitate cortical remapping. Passive stretching of the transfer is strictly prohibited.
Phase 3: Strengthening and Integration (6-12 weeks)
Progressive resistance exercises are introduced. The focus shifts from isolated firing of the transferred tendon to integrating the new movement into functional, synergistic patterns (e.g., grasping objects, pinching).
Pitfall: Premature aggressive passive stretching or heavy resistance before 8 weeks can lead to attenuation or rupture of the tendon repair site, resulting in catastrophic failure of the transfer.
Conclusion
The operative management of the paralytic hand represents one of the most intellectually and technically demanding disciplines within orthopedic surgery. By adhering to the strict biomechanical principles of tissue equilibrium, joint suppleness, and synergistic tendon selection, the surgeon can predictably restore the kinematic chain. Whether addressing an isolated peripheral nerve palsy or the profound deficits of tetraplegia, meticulous surgical execution coupled with rigorous postoperative rehabilitation can transform a flail, non-functional appendage back into an organ of purposeful interaction with the environment.
You Might Also Like