Mastering Longitudinal Deficiencies and the Krukenberg Reconstruction

Key Takeaway
The Nathan and Trung modification of the Krukenberg reconstruction transforms a forearm stump into a functional, sensate pincer. By meticulously separating the radius and ulna and dividing the flexor and extensor muscle groups, surgeons can create opposing rays. This technique eliminates the need for skin grafts by utilizing strategically designed S-shaped flaps, providing bilateral amputees with invaluable tactile feedback and independent prehension.
CONGENITAL ANOMALIES OF THE UPPER EXTREMITY: LONGITUDINAL DEFICIENCIES
The management of profound upper extremity anomalies—whether congenital or acquired—demands a rigorous understanding of embryology, pathoanatomy, and advanced reconstructive biomechanics. Congenital limb malformations are broadly categorized into failures of formation, failures of differentiation, duplication, overgrowth, undergrowth, and congenital constriction band syndrome. Within the failure-of-formation category, longitudinal deficiencies represent a complex spectrum of dysplasias that challenge the reconstructive orthopedic surgeon.
Longitudinal deficiencies encompass all failure-of-formation anomalies that do not fit the criteria for transverse deficiencies. In this distinct category are conditions such as phocomelia, radial ray dysplasia (radial clubhand), ulnar ray dysplasia, and central dysplasia (cleft hand).
Nomenclature Pearl: To accurately identify and classify these malformations, all absent or deficient bones must be explicitly named. Any bone that is not specifically named in the diagnosis is assumed to be anatomically present and fully formed.
Epidemiologically, longitudinal deformities constitute approximately 9.3% of all reported congenital upper limb malformations, making them slightly more prevalent than transverse deficiencies, which account for 7.1%.
Phocomelia: Pathoanatomy and Historical Context
The term phocomelia is derived from the Greek words phoke (seal) and melos (limb), translating literally to “seal limb” or “flipper.” It represents the most profound and devastating expression of longitudinal reduction of a limb, characterized by the absence of an intercalated segment.
Crucially, from an embryological and anatomical standpoint, the defect does not represent a true intercalary defect (where proximal and distal segments are normal but the middle is missing). Rather, it is a proximal continuum of severe radial or ulnar longitudinal dysplasia. Clinically, the term describes a condition in which a severely hypoplastic or deformed hand is suspended directly from the body near the shoulder girdle. The hand itself is usually anomalous, typically containing only three or four digits.
Historically, no definite genetic inheritance pattern was established for isolated phocomelia, and the anomaly was considered extremely rare, accounting for merely 0.8% of all congenital hand malformations. However, this changed dramatically in the late 1950s and early 1960s with the widespread use of thalidomide, a sedative and antiemetic prescribed to pregnant women.
Clinical Warning: Thalidomide acts as a potent teratogen by inhibiting angiogenesis during critical periods of limb bud development. Approximately 60% of infants born to mothers who ingested thalidomide between days 38 and 54 after conception developed phocomelia.
Frantz and O’Rahilly established the definitive anatomical classification for phocomelia, dividing the condition into three distinct types:
1. Complete Phocomelia: Characterized by the absolute absence of all limb bones proximal to the hand. The hand attaches directly to the trunk.
2. Proximal Phocomelia: Characterized by the absence or extreme hypoplasia of the proximal limb bones (humerus), with a relatively intact forearm and hand attached to the trunk.
3. Distal Phocomelia: Characterized by the hand attaching directly to the humerus, with complete absence of the radius and ulna.
Associated systemic deformities are common. In thalidomide-related phocomelia, radial ray deficiencies are frequently observed. In genetic variants, such as Robert syndrome, phocomelia presents alongside cleft lip and cleft palate. Furthermore, orthopedic surgeons must screen these patients for associated scoliosis, as well as cardiac, dermatological, chromosomal, and calcification aberrations.
Radial Ray Dysplasia (Radial Clubhand)
Radial ray dysplasia encompasses a spectrum of failure-of-formation anomalies ranging from mild hypoplasia of the thumb to complete absence of the radius. The classic presentation of severe radial dysplasia is the "radial clubhand," characterized by a shortened forearm, severe radial deviation of the wrist, and volar subluxation of the carpus relative to the distal ulna.
Management of the radial clubhand is highly complex and typically involves a staged approach. Initial treatment consists of serial casting and stretching. However, surgical intervention is usually required to centralize the carpus over the distal ulna. In severe cases with significant soft tissue contracture, acute centralization can lead to neurovascular compromise or excessive pressure on the distal ulnar physis.
To mitigate these risks, modern reconstructive techniques utilize gradual soft tissue distraction using thin-wire circular external fixators (Ilizarov principles) prior to formal centralization.
FIGURE 79-6 A: Pre-correction clinical photograph of a 9-year-old girl with severe radial clubhand deformity. A thin-wire circular external fixator has been applied to initiate gradual distraction of the contracted radial-sided soft tissues.
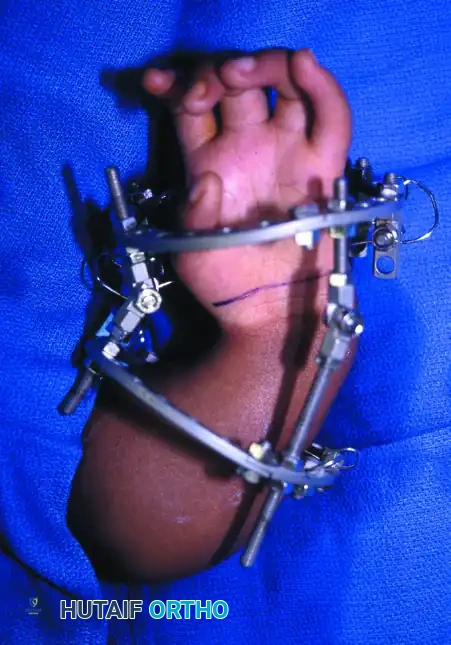
FIGURE 79-6 B: Progressive distraction achieved via the circular external fixator. This gradual elongation protects the neurovascular structures and prepares the wrist for subsequent ulnar centralization.
THE KRUKENBERG RECONSTRUCTION: BIOMECHANICS AND INDICATIONS
While congenital anomalies like phocomelia and radial clubhand require centralization or lengthening, severe transverse deficiencies or bilateral acquired amputations of the forearm present a different reconstructive challenge. For these patients, the Krukenberg procedure remains a masterclass in functional salvage.
Originally described by Hermann Krukenberg in 1917, the procedure converts a standard forearm amputation stump into a functional, sensate pincer by surgically separating the radius and the ulna. The pronator teres muscle acts as the primary motor for the radial ray (closing the pincer), while the supinator and remaining extensors open the pincer.
Indications and Patient Selection
The primary indication for a Krukenberg reconstruction is bilateral below-elbow amputation. It is particularly invaluable in:
* Visually Impaired Patients: Where tactile feedback (proprioception and stereognosis) is absolutely critical for interacting with the environment, rendering standard myoelectric prostheses inadequate.
* Developing Nations: Where access to, and maintenance of, advanced prosthetic devices is economically or logistically unfeasible.
* Severe Congenital Transverse Deficiencies: Where the child lacks functional hands bilaterally.
Surgical Pitfall: The Krukenberg procedure is generally contraindicated in unilateral amputees, as the cosmetic appearance of the separated rays is often unacceptable to patients who have one normal, functioning hand. Furthermore, the procedure requires a minimum forearm stump length (typically at least 10 cm distal to the olecranon) to ensure adequate lever arm mechanics for the pincer grasp.
The Nathan and Trung Modification
The original Krukenberg technique was fraught with soft tissue complications. The massive surgical defect created by separating the radius and ulna routinely required extensive split-thickness skin grafting. These grafts were often insensate, prone to breakdown, and lacked the durability required for a functional prehensile surface.
The Nathan and Trung Modification revolutionized the procedure by utilizing meticulously designed local fasciocutaneous flaps. By strategically excising redundant muscle bulk (while preserving primary motors) and utilizing S-shaped incisions, this modification allows for primary skin closure over the newly created radial and ulnar rays, entirely eliminating the need for skin grafts and ensuring that the tactile surfaces of the pincers possess normal, durable, sensate skin.
SURGICAL TECHNIQUE: NATHAN AND TRUNG MODIFICATION
The following is a comprehensive, step-by-step guide to the Nathan and Trung modification of the Krukenberg reconstruction. Meticulous handling of soft tissues and precise neurovascular preservation are paramount.
1. Preoperative Preparation and Incision Design
- Positioning: The patient is positioned supine with the affected limb extended on a radiolucent hand table.
- Hemostasis: A well-padded pneumatic tourniquet is applied to the proximal arm. Exsanguination is performed, and the tourniquet is inflated to standard upper extremity pressures.
- Incision: The success of the Nathan and Trung modification relies entirely on the flap design.
- Begin the incision on the dorsoulnar aspect of the forearm at the junction of the proximal and middle thirds.
- Continue this incision distally in a sweeping S-shaped fashion to create a proximal ulnar-based flap and a distal radial-based flap.
- Continue the incision palmarward (volarly) and proximally to create opposing distal ulnar-based and proximal radial-based flaps, again mirroring the S-shaped geometry.
2. Fascial Dissection and Neural Preservation
- Sharply incise the underlying antebrachial fascia directly in line with the skin incisions.
- Critical Step: Extreme care must be taken during fascial elevation to identify and preserve the medial and lateral antebrachial cutaneous nerves. These nerves provide the essential tactile sensation to the newly formed pincers; their transection defeats the primary purpose of the operation.
3. Volar Muscle Excision and Division
To allow for primary skin closure without tension, significant muscle bulk must be excised. The goal is to leave only the essential motors required for pincer function.
* Excision: Systematically identify and excise the palmaris longus (PL), the flexor carpi radialis (FCR), and the entire flexor digitorum superficialis (FDS) muscle belly.
* Preservation: The flexor digitorum profundus (FDP) must be preserved to assist in the motor function of the rays.
* Vascular Warning: Be exceptionally careful to preserve the segmental blood supply to the FDP during the excision of the overlying FDS.
* Division: Using blunt dissection, carefully divide the preserved flexor digitorum profundus into distinct radial and ulnar halves.
4. Deep Volar Dissection
- Proceed to the deep volar compartment. Identify the pronator quadratus muscle spanning the distal radius and ulna.
- Excision: Excise the pronator quadratus completely to allow for the physical separation of the distal bones.
- Neurovascular Preservation: During the excision of the pronator quadratus, meticulously identify, dissect, and preserve the anterior interosseous artery (AIA) and the anterior interosseous nerve (AIN). Ligation or injury to these structures will result in devastating ischemic and motor complications to the deep flexor remnants.
5. Dorsal Muscle Management
- Transition to the dorsal aspect of the forearm.
- Preservation: Identify and strictly preserve the brachioradialis muscle. This muscle is a critical stabilizer and secondary motor for the radial ray.
- Optional Excision: Depending on the circumference of the forearm and the tension of the skin flaps, the extensor carpi radialis longus (ECRL), extensor carpi radialis brevis (ECRB), abductor pollicis longus (APL), and extensor pollicis brevis (EPB) may be excised. This excision is often necessary to reduce dorsal bulk and allow for tension-free primary skin closure.
- Division: Identify the extensor digitorum communis (EDC). Similar to the FDP, make a longitudinal opening and bluntly divide the EDC into radial and ulnar halves.
6. Separation of the Radius and Ulna
- With the volar and dorsal musculature appropriately divided or excised, the interosseous membrane is now exposed.
- Gently divide the interosseous membrane from distal to proximal.
- This is achieved by physically pulling apart the stumps of the radius and ulna, splitting the ligamentous fibers longitudinally.
- Surgical Pearl: Do not extend the division of the interosseous membrane too proximally, as this can destabilize the proximal radioulnar joint (PRUJ) and compromise the function of the pronator teres, which is the primary motor for the new pincer grasp.
7. Closure and Perfusion Assessment
- The S-shaped flaps are now wrapped around their respective bony rays.
- Close the wound over small rubber drains.
- Begin the closure distally, closing the soft tissues over the radial stump first, followed by the ulnar stump.
- Because of the strategic S-shaped flap design and the excision of redundant muscle bulk, a skin flap or split-thickness skin graft should not be necessary for closure.
- Tourniquet Release: Deflate the tourniquet immediately after skin closure.
- Observe the flaps meticulously. Ensure that the skin of both the radial and ulnar rays blanches and fills briskly, confirming adequate microvascular perfusion.
POSTOPERATIVE CARE AND REHABILITATION PROTOCOL
The success of the Krukenberg reconstruction relies heavily on strict postoperative management and intensive, specialized rehabilitation.
Immediate Postoperative Phase (0 - 2 Weeks)
- Dressing: Apply a bulky, non-constricting compressive dressing. It is absolutely critical to physically separate the tips of the newly formed radial and ulnar rays by 6 cm or more using sterile fluffs or a custom foam wedge within the dressing. Failure to maintain this separation can lead to soft tissue contracture and loss of pincer width.
- Elevation: The reconstructed limb must be elevated continuously for the first 48 hours to minimize edema and protect the viability of the fasciocutaneous flaps.
- Drain Management: The rubber drains are removed in a routine fashion, typically at 24 to 48 hours postoperatively, once output has minimized.
- Suture Removal: Skin sutures are removed at exactly 2 weeks, provided the incisions have healed without marginal necrosis.
Rehabilitation Phase (2 Weeks and Beyond)
- Rehabilitation is initiated 2 to 3 weeks after surgery, once the soft tissue envelope is stable.
- Motor Retraining: The primary focus of physical therapy is to develop strong, independent abduction and adduction of the rays.
- Adduction (Pinch): The patient must learn to fire the pronator teres to bring the radial ray toward the ulnar ray.
- Abduction (Release): The patient must learn to fire the supinator and remaining extensors to open the pincer.
- Sensory Re-education: Because the native antebrachial cutaneous nerves were preserved, the patient will have immediate tactile feedback. Occupational therapy focuses on stereognosis training, allowing the patient to identify objects by texture, size, and temperature without visual input.
- Strengthening: Progressive resistance exercises are introduced at 6 weeks to maximize the pinch strength of the new prehensile organ, enabling the patient to perform activities of daily living (ADLs) such as feeding, dressing, and personal hygiene independently.
You Might Also Like


