Clinical Evaluation and Surgical Management of Upper Extremity Peripheral Nerve Injuries
Key Takeaway
Accurate clinical assessment of upper extremity peripheral nerve injuries is paramount for determining surgical indications and predicting functional outcomes. This guide details the precise motor, sensory, and autonomic evaluations required for the median, ulnar, and radial nerves. It further outlines evidence-based surgical approaches, intraoperative decision-making, and standardized postoperative assessment protocols endorsed by the American Society for Surgery of the Hand to optimize patient recovery.
Introduction to Peripheral Nerve Assessment
The precise evaluation of peripheral nerve injuries in the upper extremity requires a profound understanding of neuroanatomy, muscle biomechanics, and anomalous innervation patterns. Foundational texts, notably the work of MacKinnon and Dellon, emphasize that accurate clinical diagnosis dictates both the timing and the nature of surgical intervention. A meticulous physical examination must isolate individual muscle functions, eliminating the confounding effects of synergistic muscles and trick movements.
This comprehensive guide delineates the postgraduate-level assessment of the median, ulnar, and radial nerves, followed by the standardized protocols for surgical exploration, microsurgical repair, and postoperative rehabilitation.
The Median Nerve: Clinical and Biomechanical Evaluation
The median nerve is the primary motor nerve for the flexor compartment of the forearm and the precision pinch mechanics of the hand.
Proximal and Distal Motor Innervation
In the forearm, the median nerve innervates the pronator teres, flexor carpi radialis (FCR), palmaris longus, and flexor digitorum sublimis (FDS). The anterior interosseous nerve (AIN) branch supplies the index and middle flexor digitorum profundus (FDP), the flexor pollicis longus (FPL), and the pronator quadratus.
In the hand, the usual median-innervated muscles of critical concern include:
* The lumbricals to the index and long fingers.
* The opponens pollicis.
* The abductor pollicis brevis (APB).
* The superficial head of the flexor pollicis brevis (FPB).
Clinical Testing of the Median Nerve
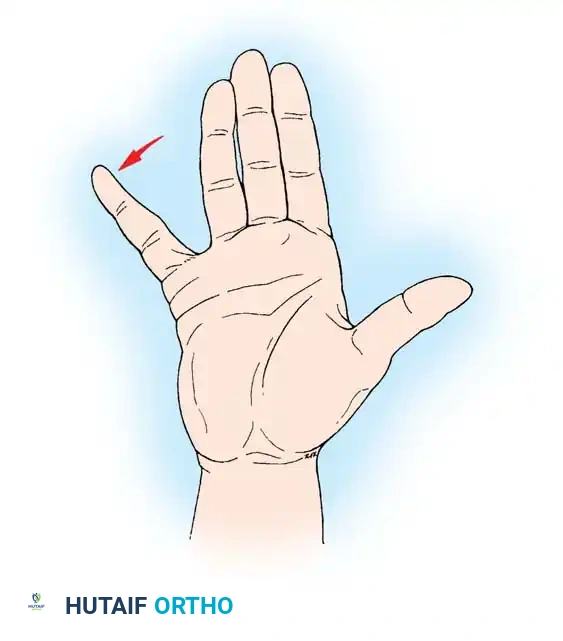
The single most reliable median nerve–mediated motor function to evaluate is the apposition of the tip of the thumb to the pulp of the ring or little finger.
Clinical Pearl: Visual inspection of thumb opposition is insufficient. The examiner must simultaneously palpate the active contraction of the abductor pollicis brevis (APB) muscle belly. This ensures the motion is not a "trick movement" generated by the adductor pollicis (ulnar nerve) or the flexor pollicis longus (AIN).
Anomalous Innervation Patterns
Surgeons must maintain a high index of suspicion for anatomical variations that cause cross-innervation.
* Martin-Gruber Anastomosis: Present in up to 15% of the population, involving a crossover of motor fibers from the median to the ulnar nerve in the forearm.
* Riche-Cannieu Anastomosis: A connection between the deep branch of the ulnar nerve and the recurrent motor branch of the median nerve in the palm, which can result in ulnar innervation of the APB or median innervation of the adductor pollicis.
The Ulnar Nerve: Clinical and Biomechanical Evaluation
The ulnar nerve governs the intrinsic power and synchronized digital motion of the hand. Its evaluation requires careful isolation of the intrinsic muscles from the extrinsic long flexors and extensors.
Proximal and Distal Motor Innervation
Proximally, the ulnar nerve innervates the flexor carpi ulnaris (FCU) and the FDP tendons to the ring and little fingers.
In the hand, the ulnar-innervated muscles of interest include:
* The deep head of the flexor pollicis brevis (FPB).
* The adductor pollicis.
* The hypothenar group: abductor digiti minimi (ADM), flexor digiti minimi (FDM), and opponens digiti minimi (ODM).
* All dorsal and volar interosseous muscles.
* The lumbricals to the ring and little fingers.
Clinical Testing of the Ulnar Nerve
When testing for motor function of the ulnar nerve in the hand, the examiner must isolate the intrinsic muscles. The standard test involves active abduction of the middle finger from the ulnar to the radial side with the palm resting flat on a surface (Egawa's sign).
Surgical Warning: This motion must be observed carefully to exclude the function of the extrinsic tendons. The long flexor tendons tend to converge the digits (mimicking volar interossei), while the long extensor tendons tend to diverge the fingers (mimicking dorsal interossei). Keeping the hand flat neutralizes these extrinsic forces.
Thumb adduction is evaluated using Froment’s Sign. The patient is asked to hold a piece of paper tightly in the thumb-index web space, squeezing it between the thumb interphalangeal (IP) joint and the base of the index finger proximal phalanx. If the adductor pollicis is weak or paralyzed, the patient cannot hold the paper against resistance without hyperflexing the thumb IP joint (recruiting the FPL, innervated by the AIN).
The function of the abductor digiti minimi (ADM) is tested by having the patient abduct the little finger against resistance while the examiner palpates the muscle belly.
Pathomechanics of the Ulnar Claw Hand
Although clawing of the little and ring fingers may not be immediately apparent at the time of an acute injury, it frequently develops over time. Clawing results from the loss of intrinsic muscle function (which normally flexes the metacarpophalangeal [MCP] joints and extends the IP joints). Without the intrinsics, the extensor digitorum communis (EDC) hyperextends the MCP joints, and the FDP hyperflexes the IP joints.
Note on Anomalies: The first dorsal interosseous muscle may receive anomalous innervation from the median nerve in approximately 10% of hands.
The Radial Nerve: Clinical and Biomechanical Evaluation
The radial nerve is responsible for the extension of the elbow, wrist, and digits, providing the essential stable platform required for effective grip strength.
Proximal and Distal Motor Innervation
Proximal muscles innervated by the radial nerve include the triceps, brachioradialis, supinator, and anconeus.
The radially innervated muscles influencing the hand and wrist include:
* Extensor carpi radialis longus (ECRL) and brevis (ECRB).
* Extensor carpi ulnaris (ECU).
* Extensor digitorum communis (EDC).
* Extensor indicis proprius (EIP) and extensor digiti minimi (EDM).
* Abductor pollicis longus (APL), extensor pollicis longus (EPL), and extensor pollicis brevis (EPB).
Clinical Testing of the Radial Nerve
Motions mediated by the radial nerve include wrist dorsiflexion, radial/ulnar deviation in extension, and thumb abduction/extension.
Pitfall in Examination: Metacarpophalangeal (MCP) extension is strictly mediated by the radial nerve via the EDC. Examiners must evaluate this carefully and not be confused by extension of the proximal and distal interphalangeal (PIP and DIP) joints. IP joint extension is controlled by the intrinsic muscles (lumbricals and interossei) via the lateral bands, which are innervated by the median and ulnar nerves.
Autonomic Evaluation: Sudomotor Activity
Sympathetic nerve fibers travel with peripheral sensory nerves. Therefore, a complete nerve transection results in an immediate loss of sympathetic tone in the corresponding dermatome, leading to anhidrosis (loss of sweating).
Usually, a denervated area shows no sweating within about 30 minutes after a nerve injury. In the acute trauma bay, it is highly helpful to compare the normal and suspected injured areas by palpation with a dry fingertip. The denervated skin will feel smooth and lack the normal tactile friction (tackiness) provided by microscopic sweat droplets. Formal testing can be documented using the Ninhydrin test or the O'Riain wrinkle test (denervated skin does not wrinkle when submerged in warm water).
Surgical Management of Peripheral Nerve Injuries
When clinical evaluation indicates a complete nerve transection (neurotmesis) or a failure of conservative management in closed injuries, surgical exploration is mandated.
Indications for Surgery
- Open Injuries: Sharp lacerations with corresponding distal deficits require early exploration and primary repair (within 72 hours).
- Closed Injuries: High-energy traction injuries or crush injuries are typically observed for 3 months. If clinical and electromyographic (EMG) evidence shows no signs of reinnervation, surgical exploration is indicated.
- Iatrogenic Injuries: Immediate exploration is required if a nerve deficit is noted immediately following an orthopedic procedure (e.g., radial nerve palsy after humeral plating where the nerve was not visualized).
Positioning and Approach
- Positioning: The patient is positioned supine with the affected extremity on a radiolucent hand table.
- Tourniquet: A pneumatic tourniquet is applied to the proximal arm and inflated to 250 mmHg (or 100 mmHg above systolic pressure) after exsanguination. This provides a bloodless field, which is absolute critical for microsurgery.
- Incisions: Surgical approaches must utilize extensile incisions. In the digits and palm, Brunner zig-zag incisions or lazy-S incisions are mandatory to prevent postoperative flexion contractures across flexion creases.
Microsurgical Repair Principles
- Preparation of Nerve Ends: The injured nerve ends must be resected back to healthy, viable fascicles (the "pouting" fascicle sign).
- Tension-Free Repair: The primary axiom of nerve surgery is that repairs must be completely tension-free. If primary end-to-end epineurial repair cannot be achieved without tension, a nerve graft (commonly the reversed sural nerve) or a nerve conduit must be utilized.
- Suturing: Under an operating microscope, the epineurium is approximated using 8-0 or 9-0 non-absorbable monofilament sutures (e.g., Nylon). Alignment of the superficial epineurial vascular markings helps prevent rotational malalignment of the fascicles.
Postoperative Assessment and Rehabilitation
In 1984, the Clinical Assessment Committee of the American Society for Surgery of the Hand (ASSH) recommended four standardized areas of importance in evaluating the progress of peripheral nerve injury and repair:
1. Sensibility testing
2. Motor testing
3. Subjective evaluation
4. Sudomotor function
Sensibility Evaluation
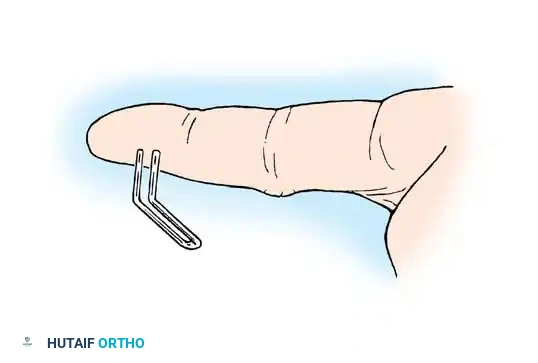
The basic minimum tests recommended for sensibility evaluation are stationary (static) two-point discrimination and moving two-point discrimination.
- Moving Two-Point Discrimination (Dellon): Evaluates the quickly adapting mechanoreceptors (Meissner corpuscles). It is typically the first to return following nerve repair.
- Static Two-Point Discrimination (Weber): Evaluates the slowly adapting mechanoreceptors (Merkel cells). Normal static two-point discrimination at the fingertip is 2 to 5 mm.
Functional tactile gnosis returns concurrently with the return of two-point discrimination. A formal statement relative to sweating (sudomotor function) should always be included in the longitudinal outpatient evaluation.
Postoperative Protocol
- Phase I (0-3 Weeks): The extremity is immobilized in a custom orthosis to protect the repair. For volar repairs (median/ulnar), the wrist and digits are placed in slight flexion.
- Phase II (3-6 Weeks): The orthosis is adjusted to allow protected, guided active range of motion (ROM) to prevent tendon adhesions while avoiding tension on the nerve repair.
- Phase III (6+ Weeks): Progressive strengthening and sensory re-education programs are initiated. Sensory re-education helps the cerebral cortex remap the altered afferent signals arriving from the regenerating nerve.
By adhering to these rigorous standards of clinical examination, precise microsurgical technique, and structured postoperative assessment, orthopedic surgeons can maximize functional recovery in patients sustaining complex peripheral nerve injuries.
You Might Also Like
