Excision of Extra Digit & Polydactyly Reconstruction
Key Takeaway
The surgical management of polydactyly requires meticulous preoperative planning to optimize both aesthetic and functional outcomes. Excision of an extra digit involves careful neurovascular dissection, preservation of essential tendinous insertions, and precise ligamentous reconstruction. Complex presentations, such as central polydactyly or ulnar dimelia (mirror hand), necessitate advanced reconstructive techniques including pollicization, osteotomies, and targeted tendon transfers to restore functional prehension and joint stability.
INTRODUCTION TO POLYDACTYLY AND DIGIT DUPLICATION
Polydactyly is one of the most common congenital anomalies of the upper extremity, presenting with a wide spectrum of morphological variations ranging from a rudimentary soft-tissue skin tag to complete duplication of a ray, including complex syndromic associations. The overarching goal of surgical intervention is to create a functional, stable, and aesthetically acceptable hand.
Surgical management is dictated by the anatomical classification of the duplication: preaxial (radial/thumb), central (index, long, ring fingers), and postaxial (ulnar/small finger). The excision of an extra digit is rarely a simple amputation; it demands a comprehensive understanding of the shared neurovascular anatomy, tendinous insertions, and collateral ligament complexes to prevent postoperative angular deformities and functional deficits.
EXCISION OF EXTRA DIGIT (POSTAXIAL POLYDACTYLY)
Postaxial polydactyly involves the duplication of the small finger (ulnar border of the hand). It is broadly categorized into two primary types based on the presence of osseous and articular involvement:
* Type 1 Duplication: A rudimentary soft-tissue appendage lacking skeletal articulation, often connected by a narrow cutaneous pedicle.
* Type 2 Duplication: A fully or partially developed digit with osseous components articulating with a bifurcated metacarpal or phalanx.
Preoperative Planning and Biomechanics
In Type 2 duplications, the extra digit often shares a common joint capsule, collateral ligament complex, and tendinous insertions with the dominant digit. The abductor digiti minimi (ADM) frequently inserts into the ulnar-most (duplicated) digit. Simple amputation without reconstruction of the ADM and the ulnar collateral ligament (UCL) will inevitably lead to a progressive radial deviation deformity of the retained small finger due to unopposed radial intrinsic forces.
Surgical Technique: Step-by-Step Approach
🔪 Surgical Pearl: Incision Design
Never discard skin prematurely. Always design your incisions to leave excess skin flaps during the initial exposure. The complex three-dimensional contour of the web space and lateral digit often requires more skin for tension-free closure than initially anticipated. Excess skin can be easily trimmed at the time of final closure.
- Positioning and Hemostasis:
- The patient is positioned supine with the arm extended on a radiolucent hand table.
- General anesthesia is administered.
- A well-padded pediatric pneumatic tourniquet is applied to the upper arm. Exsanguination is performed using an Esmarch bandage, and the tourniquet is inflated to the appropriate weight-based pressure.
- Incision:
- Make an elliptical (racquet-shaped) incision around the base of the extra digit.
- Ensure the apex of the incision extends proximally enough to expose the underlying metacarpophalangeal (MCP) or interphalangeal joint.
- Neurovascular Dissection:
- Carefully dissect through the subcutaneous tissue.
- Identify the neurovascular bundle supplying the extra digit. It is critical to trace the digital nerve proximally to its bifurcation from the common digital nerve to ensure the branch to the retained digit is not inadvertently injured.
- Ligate and divide the neurovascular bundle dedicated to the extra digit.
- Management of Type 1 Duplication:
- If the duplication is purely soft tissue (Type 1), complete the excision at the fascial level.
- Perform a simple layered closure of the skin.
- Management of Type 2 Duplication (Osseous Involvement):
- Identify and meticulously dissect the abductor digiti minimi (ADM) tendon. If it inserts into the extra digit, detach it with a generous periosteal sleeve for later reattachment.
- Expose the area of bone bifurcation subperiosteally.
* Identify and preserve the **ulnar collateral ligament (UCL)** if the bifurcation occurs at the level of the joint.
* Amputate the extra digit at the level of the bifurcation.
* Using a rongeur or oscillating saw, trim any excess bone or prominent condyles at the bifurcation site to create a smooth, anatomic contour. Failure to adequately reduce the condylar flare will result in a cosmetically unacceptable bony prominence.
- Ligamentous and Tendinous Reconstruction:
- Reconstruct the collateral ligament by advancing it and suturing it to the periosteum or using bone anchors at the base of the retained phalanx.
- Reattach the ADM tendon to the base of the proximal phalanx of the retained digit to restore dynamic ulnar stability and abduction.
- Closure:
- Deflate the tourniquet and achieve meticulous hemostasis.
- Trim any redundant skin flaps to ensure a smooth contour without dog-ears.
- Close the skin with simple interrupted absorbable sutures (e.g., 5-0 or 6-0 chromic gut or fast-absorbing plain gut).
Postoperative Care
- Apply a bulky, soft compressive bandage.
- In very young, active children, a short-arm cast or rigid splint may be applied for 10 to 14 days to protect the ligamentous reconstruction.
- Generally, prolonged immobilization is unnecessary. Sutures are removed (or allowed to dissolve) at 2 weeks, after which unlimited activity and gentle range of motion (ROM) are encouraged.
CENTRAL POLYDACTYLY
Central polydactyly is defined as the duplication of the index, long, or ring finger. It is a rare anomaly when presenting as a solitary deformity and is most frequently associated with complex syndactyly (polysyndactyly).
Pathoanatomy and Genetics
The most typical morphological pattern is a Type 2 central polydactyly that is entirely concealed within a syndactyly web between the long and ring fingers. The duplicated osseous structures are often dysplastic, sharing tendons and neurovascular elements with the adjacent digits.
Genetically, polydactyly of the index finger and polysyndactyly of the long and ring fingers are frequently inherited as autosomal dominant traits with variable penetrance. A thorough clinical evaluation must be performed, as these anomalies are highly associated with concomitant polydactyly and syndactyly of the toes.
Surgical Management Principles
Treatment of isolated central polydactyly involves the excision of the most hypoplastic and non-functional digit.
🚨 Surgical Warning: Central Ray Excision
Excision of a central digit is fraught with the risk of creating a divergent web space or angular deformity of the adjacent digits. Meticulous reconstruction of the deep transverse metacarpal ligament and collateral ligaments is mandatory to prevent postoperative digital divergence.
- Incision: Complex zigzag (Bruner) or dorsal/volar triangular flap incisions are utilized to simultaneously address the syndactyly release and the digit excision.
- Reconstruction: Following the excision of the dysplastic central ray, the adjacent digits must be stabilized. This often requires the transfer of collateral ligaments and the reconstruction of the intermetacarpal ligaments.
- Web Space Deepening: Local advancement flaps or full-thickness skin grafts are frequently required to reconstruct the commissure and deepen the web space appropriately.
ULNAR DIMELIA (MIRROR HAND)
Ulnar dimelia, commonly referred to as "mirror hand," is an extremely rare and complex congenital anomaly characterized by the duplication of the ulnar axis and the complete absence of the radial axis.
Pathoanatomy and Kinematics
The classic presentation of ulnar dimelia includes:
* Forearm: Complete duplication of the ulna and ulnar carpal bones. The radius is entirely absent.
* Carpus: The scaphoid and trapezium are replaced by duplicated ulnar-sided carpal bones (e.g., triquetrum, hamate). The distal ulnar epiphysis is significantly broadened.
* Hand: Symmetrical duplication of the digits, typically resulting in seven or eight fingers. There is a complete absence of the thumb (preaxial digits) and the first web space.
* Elbow: The elbow joint is highly abnormal. Each of the duplicated ulnae articulates separately with the distal humerus, and they tend to face each other. The capitellum is absent from the distal humerus, leading to severe restrictions in elbow flexion, extension, pronation, and supination.

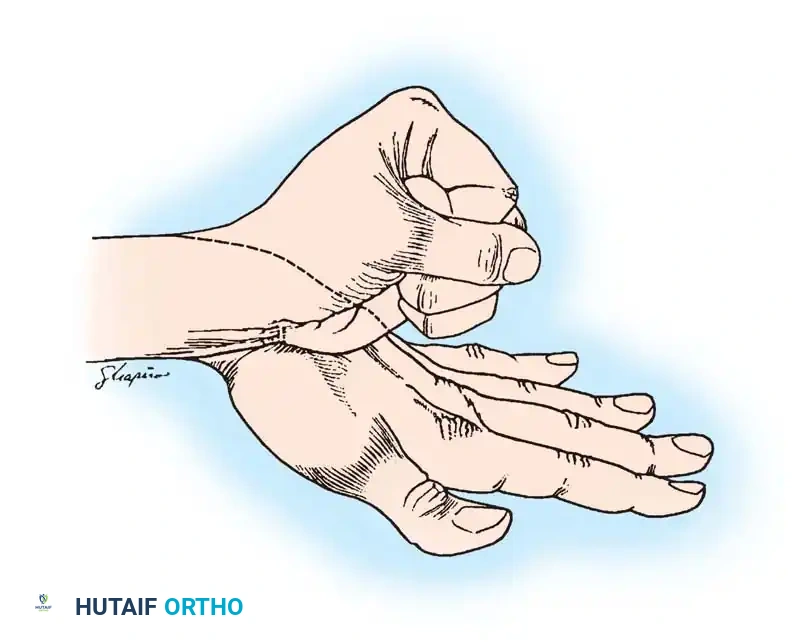
FIGURE 1: Appearance of mirror hand with extra digits. The anatomy reveals a radial ulna, duplicated ulnar carpus, and multiple postaxial digits (Digits I through VII).
Preoperative Management
Surgical reconstruction is complex and staged. Prior to surgical intervention, parents must be instructed to perform rigorous passive range of motion (ROM) exercises. Gentle stretching of the fingers, wrist, elbow, and shoulder should be maintained daily until the child reaches the appropriate age for reconstruction (typically around 2 years of age).
During this observational period, the surgeon must carefully evaluate the child during play to determine which of the radial-sided digits exhibits the best independent function and mobility. This digit will be selected for pollicization.
Surgical Reconstruction: The Entin and Buck-Gramcko Principles
Surgical intervention should be performed early to optimize cortical neuroplasticity and prevent psychological trauma. The reconstructive goals include reducing the number of digits, creating a functional thumb (pollicization), establishing a first web space, and improving wrist and elbow kinematics.
1. Digit Deletion and Pollicization
The most widely accepted approach is the Entin reconstruction, modified by the pollicization principles of Buck-Gramcko.
- Digit Selection: The most functional radial digit (often Digit II) is retained for pollicization. The excess radial digits (typically Digits I and III) are amputated, including their respective metacarpals and carpal bones.
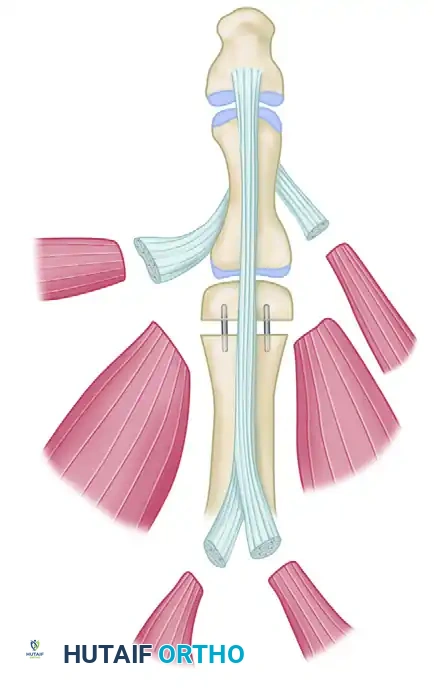
- Osteotomy and Positioning: The retained digit (Digit II) must be shortened and rotated to simulate a thumb. An osteotomy is performed through the base of its metacarpal. To achieve the correct length and palmar abduction, an intermetacarpal bone graft—harvested from the discarded metacarpal of Digit III—is utilized to stabilize the pollicized digit in its new position.

FIGURE 2: Pollicization of digit II. The digit is properly positioned via an osteotomy through the base of its metacarpal, supported by an intermetacarpal graft cut from the discarded metacarpal of digit III.
2. Soft Tissue and Web Space Reconstruction
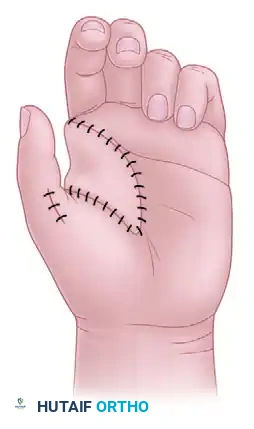
Creating an adequate first web space is critical for thumb function. The excess skin from the amputated digits is not discarded; rather, it is carefully elevated as a filleted flap.
- The filleted skin of the discarded Digit III is transposed to cover the large soft-tissue defect created by the pollicization and to construct a wide, supple first web space.
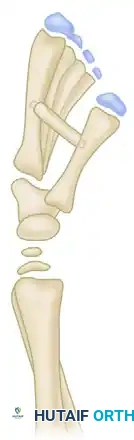
FIGURE 3: The filleted skin of digit III is utilized as a robust fasciocutaneous flap to cover the space created by the pollicization and establish the new first web space.
3. Tendon Transfers for Finger Extension
Patients with ulnar dimelia frequently suffer from inadequate finger and wrist extension due to the absence of the radial nerve-innervated extensor musculature.
* Tendon transfers are often necessary. Donor tendons from the amputated digits can be routed to augment extension.
* If the flexor carpi ulnaris (FCU) is duplicated, one slip can be transferred dorsally to improve wrist or digital extension.
Management of the Elbow and Wrist
The functional limitations of the elbow and wrist in ulnar dimelia are profound and require dedicated surgical strategies.
Elbow Flexion:
To improve severe restrictions in elbow flexion, Harrison et al. described a technique involving the excision of the upper 1-inch portion of the lateral (radial-sided) duplicated ulna.
* Outcomes: While this procedure can initially achieve up to 40 degrees of improved elbow flexion in a 1-year-old, long-term follow-up often reveals recurrent stiffness into extension as the child grows.
* Postoperative Protocol: Aggressive postoperative muscle strengthening and dynamic splinting are mandatory to maintain the gains achieved from the proximal ulnar excision.
Forearm Rotation:
Pronation and supination are virtually absent due to the parallel, facing ulnae. A rotational osteotomy of the forearm may be required to place the hand in a more functional, fixed position of slight pronation, optimizing the hand for activities of daily living.
Wrist Extension and Stability:
Limitation of wrist extension is common due to severe palmar and radial soft-tissue contractures.
* Soft Tissue Release: Z-plasty of the volar skin, combined with lengthening of the contracted flexor tendons and volar wrist capsule, is often required.
* Tendon Transfers: The flexor carpi radialis (FCR) muscle (if present/anomalous) or the flexor digitorum superficialis (FDS) of the pollicized finger can be transferred to the dorsum of the index metacarpal to provide active wrist extension.
* Salvage Procedures: For recurrent, intractable wrist instability or severe flexion contractures, a formal wrist arthrodesis is highly effective. This is typically delayed until skeletal maturity is approached, usually around 12 years of age, to avoid arresting carpal growth prematurely.
Conclusion
The surgical correction of polydactyly and complex duplications like ulnar dimelia represents one of the most challenging frontiers in pediatric hand surgery. Success relies not merely on the ablation of excess tissue, but on the meticulous, biomechanically sound reconstruction of the remaining skeletal, ligamentous, and musculotendinous architecture. Through staged interventions, precise pollicization techniques, and rigorous postoperative rehabilitation, surgeons can provide these patients with highly functional and aesthetically improved upper extremities.
You Might Also Like