Operative Management of Congenital Hand and Forearm Anomalies

Key Takeaway
Congenital upper extremity anomalies require meticulous surgical planning to optimize function and prevent progressive deformity. This guide details the operative techniques for ulnar anlage excision, the Straub one-bone forearm creation, and syndactyly release. Emphasizing precise soft-tissue handling, neurovascular protection, and strategic flap design, these procedures are essential for pediatric orthopedic surgeons aiming to restore biomechanical alignment and functional prehension in the developing hand.
INTRODUCTION TO CONGENITAL UPPER EXTREMITY RECONSTRUCTION
The surgical management of congenital upper extremity anomalies demands a profound understanding of altered pathoanatomy, biomechanics, and the natural history of the developing pediatric skeleton. Conditions such as ulnar longitudinal deficiency and syndactyly present unique reconstructive challenges. The primary goals of intervention are the prevention of progressive angular deformities, the restoration of functional prehension, and the optimization of cosmetic appearance. This masterclass details the advanced operative techniques for the excision of an ulnar anlage, the creation of a one-bone forearm, and the comprehensive management of syndactyly.
EXCISION OF AN ULNAR ANLAGE (FLATT TECHNIQUE)
Ulnar longitudinal deficiency (ulnar clubhand) is frequently associated with a fibrocartilaginous band known as the ulnar anlage. This structure acts as a non-yielding tether during longitudinal growth, leading to progressive bowing of the radius, dislocation of the radial head, and severe ulnar deviation of the carpus and hand. Early excision of this tether is biomechanically critical to allow the radius to grow without restriction and to centralize the carpus.
Indications and Preoperative Planning
Excision is indicated in patients with progressive ulnar deviation of the hand or worsening radial bowing. Surgery is typically performed in the first year of life (often between 6 and 12 months) to maximize the remodeling potential of the radius.
💡 Clinical Pearl
The absence of extrinsic flexor muscles in severe ulnar longitudinal deficiency fundamentally alters the volar anatomy. The ulnar neurovascular bundle is not protected by muscle bellies and lies directly adjacent to the anlage in the subcutaneous tissue. Meticulous superficial dissection is mandatory.
Surgical Technique Step-by-Step
- Positioning and Approach:
- Place the patient supine with the affected arm on a radiolucent hand table.
- Exsanguinate the limb and inflate a pneumatic tourniquet.
- Design a lazy-"S" incision along the postaxial (ulnar) border of the forearm. Carry the incision distally across the wrist crease to the midcarpal level to allow full exposure of the ulnocarpal articulation.
- Neurovascular Dissection:
- Carefully incise the subcutaneous tissues. Identify the ulnar neurovascular bundle early.
- Because of the hypoplasia or complete absence of the flexor carpi ulnaris and other extrinsic flexors, the bundle will be intimately associated with the fibrocartilaginous anlage.
- Free the neurovascular bundle using blunt dissection and retract it radially with vessel loops for absolute protection.
- Resection of the Anlage:
- Trace the anlage distally to its carpal attachments (often the pisiform or triquetrum) and proximally to the ulnar remnant.
- Resect at least one-third of the distal forearm length of the anlage. Inadequate resection risks recurrent tethering through scar tissue formation.
- Soft Tissue Release and Realignment:
- Incise the contracted soft tissues on the ulnar aspect of the wrist joint. This release must be extensive enough to allow the carpus to translate radially and seat squarely on the distal radial articular surface.
- Biomechanical Check: The hand should passively "flop" into neutral alignment or slight radial deviation. If the surgeon must actively push the hand into neutral, the soft tissue release is insufficient, and further ulnar-sided structures must be divided.
- Closure:
- Deflate the tourniquet and achieve meticulous hemostasis.
- Close the skin with interrupted nonabsorbable sutures (e.g., 5-0 or 6-0 nylon) to accommodate postoperative swelling.
Postoperative Protocol
- Apply a well-molded, long-arm cast with the wrist held in neutral to slight radial deviation and the elbow at 90 degrees of flexion.
- 3 Weeks: Remove sutures and apply a new long-arm cast.
- 6 Weeks: Discontinue cast immobilization. Initiate a gradual return to normal activities and range-of-motion exercises over the subsequent 4 to 6 weeks. Night splinting may be required to maintain alignment.
CREATION OF A ONE-BONE FOREARM (STRAUB TECHNIQUE)
In cases of severe radioulnar synostosis, profound forearm instability, or advanced ulnar longitudinal deficiency where the radial head is dislocated and the forearm is functionally useless, the creation of a one-bone forearm (radioulnar fusion) provides a stable, single osseous strut. This sacrifices pronosupination but restores a stable lever arm for hand function.
Surgical Technique Step-by-Step
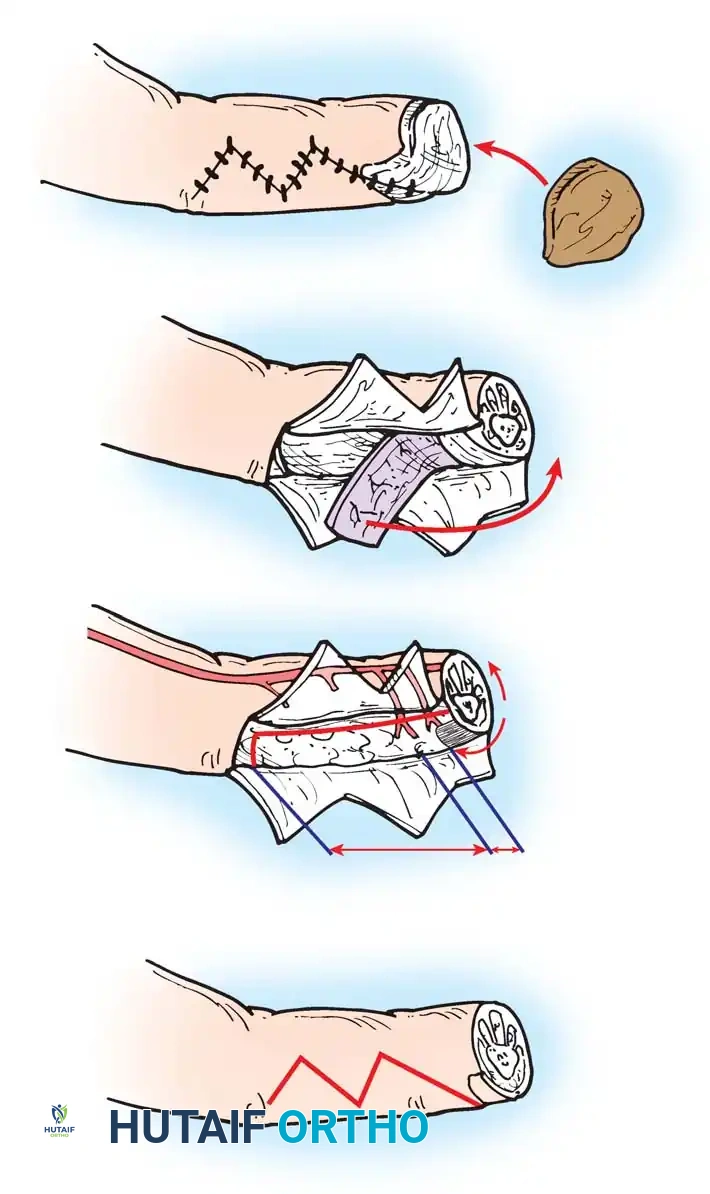
- Incision and Exposure:
- Make a curved longitudinal dorsoradial incision, beginning just proximal to the elbow joint and extending distally to the middle or distal third of the forearm.
- Anlage Excision (If Present):
- Expose and excise the fibrocartilaginous band extending distally from the proximal ulnar fragment.
- Free the proximal end of this band by performing a transverse osteotomy at the distal end of the ulnar fragment.
- Nerve Identification (Critical Step):
- Expose the radial nerve at the level of the elbow.
- Trace the nerve distally to its bifurcation, paying special attention to the posterior interosseous nerve (PIN).
- Surgical Warning: The PIN and the supinator muscle are often grossly displaced anteriorly or medially due to the congenital dislocation of the proximal radius.
- Muscle Cleavage and Osteotomy:
- Develop the internervous cleavage plane between the dorsal and volar muscle compartments of the forearm. Protect all antecubital neurovascular structures.
- At the exact level of the distal end of the ulnar fragment, divide the radial shaft.
- Excise the proximal portion of the radius, including the dislocated radial head.
Figure A: Resection of the distal ulnar anlage and the proximal radius (shaded areas).
- Osseous Alignment and Fixation:
- Transpose the proximal end of the distal radial fragment and abut it directly against the distal end of the proximal ulnar fragment.

Figure B: Alignment of the distal radius and proximal ulna to create a single osseous strut.
- Fix the construct rigidly. Pass a stout Kirschner wire (or Steinmann pin) antegrade through the olecranon, across the osteotomy site, and distally into the radial segment and carpus to ensure absolute stability.
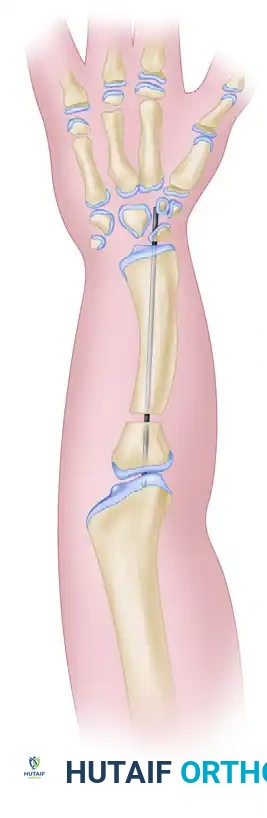
Figure C: Kirschner wire extending into the carpals, used to stabilize the newly created radioulnar segment.

Composite Diagram: Creation of a one-bone forearm demonstrating resection, alignment, and K-wire fixation.
- Closure:
- Close the deep fascia loosely to prevent compartment syndrome. Close the skin with absorbable or nonabsorbable sutures.
Postoperative Protocol
- Apply a long-arm cast with the elbow flexed to approximately 90 degrees and the forearm in neutral rotation.
- 2 Weeks: Perform a cast change and remove any remaining nonabsorbable sutures.
- 8 Weeks: The long-arm cast and the Kirschner wire/Steinmann pin are removed once radiographic evidence of solid bony union is confirmed.
- Rehabilitation: Normal activities are resumed gradually over the next 6 to 8 weeks, focusing on shoulder and hand therapy to compensate for the fused forearm.
SYNDACTYLY RECONSTRUCTION
Syndactyly is one of the most common congenital hand anomalies, characterized by the failure of digital separation during embryogenesis. It occurs most frequently between the long and ring fingers (>50% of cases) and is bilateral in approximately half of affected patients. Males are affected more frequently than females.
Classification and Pathoanatomy
- Simple Syndactyly: Digits are bridged only by skin and soft tissue.
- Complex Syndactyly: Digits share common bony elements (e.g., fused phalanges).
- Acrosyndactyly: Lateral fusion of adjacent digits at their distal ends, with proximal fenestrations (epithelialized tracts) between the joined digits.
- Brachysyndactyly: Syndactyly associated with abnormal shortening of the involved digits.

Figure: Simple syndactyly, palmar view. Fingers are bridged only by skin and soft tissues.

Figure: Simple syndactyly, dorsal view.
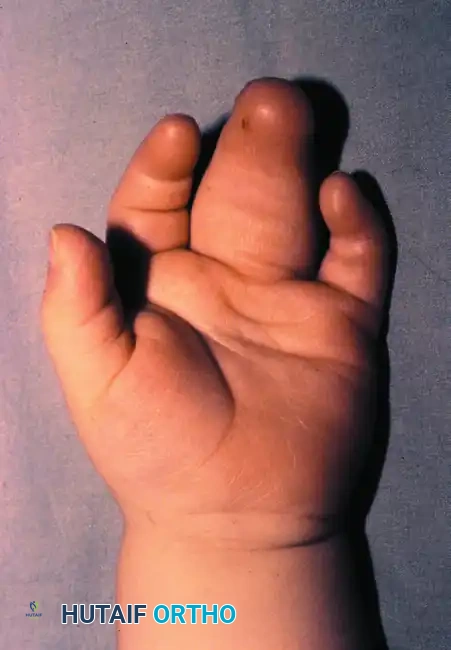
Figure: Radiograph of simple syndactyly. Note the angular deformity beginning to develop in the ring finger.
Syndromic Associations
Syndactyly is frequently associated with systemic syndromes.
* Poland Syndrome: Characterized by unilateral brachysyndactyly, hypoplasia of the hand, and the pathognomonic absence of the sternocostal portion of the ipsilateral pectoralis major muscle.
* Apert Syndrome: Characterized by complex, multiple syndactylies (often a "rosebud" or "mitten" hand) associated with craniosynostosis.

Figure: Poland syndrome in an 18-month-old child.

Figure A: Brachysyndactyly associated with Poland syndrome.

Figure B: Palmar view of brachysyndactyly.

Figure C: Hypoplasia of the pectoralis major muscle, a hallmark of Poland syndrome.
Epidemiology of Web Space Involvement
The incidence of syndactyly follows a predictable pattern across the web spaces:
* Third Web (Long-Ring): >50%
* Fourth Web (Ring-Small): ~27%
* Second Web (Index-Long): ~14%
* First Web (Thumb-Index): ~3-9%
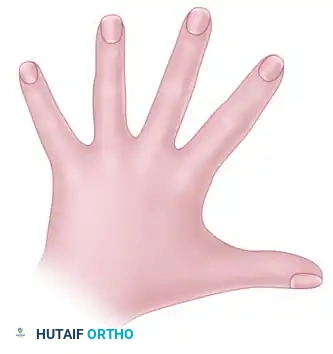
Figure A: Percentage incidence of pure syndactyly (simple or complex).
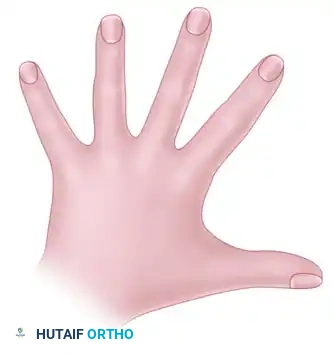
Figure B: Total count incidence including all associated webbed digit conditions.
Timing of Surgical Intervention
Surgical timing is a delicate balance between preventing angular deformity and minimizing the risk of postoperative web creep (distal migration of the commissure).
- Border Digits (Urgent - 6 to 12 Months): Syndactyly involving digits of unequal length (e.g., thumb-index or ring-small fingers) must be released early. The tethering effect of the shorter digit will rapidly cause flexion, lateral deviation, and rotational contractures in the longer digit.
- Central Digits (Elective - 18 to 36 Months): If the syndactyly involves the second or third web space without other deformities, surgery is delayed until the child is at least 18 months old. Delaying surgery reduces the incidence of scar contracture and distal web migration.
- Multiple Digits (Staged): When multiple digits are involved, release must be staged. Never release both sides of a single digit simultaneously. Doing so severely compromises the digital blood supply and risks ischemic necrosis. Staged procedures should be separated by a minimum of 6 months.
🚨 Surgical Warning
The surface area of two conjoined digits is significantly less than the surface area of two separate digits. Primary closure is almost never possible without inducing severe tension and subsequent ischemia. Skin grafting is a mandatory component of syndactyly release.
Surgical Principles and Technique
Reconstruction involves three critical steps: separation of the digits, commissure reconstruction, and resurfacing of the intervening borders.
1. Separation of the Digits
- Incision Design: Straight linear incisions are strictly contraindicated as they lead to longitudinal scar contracture. Use interdigitating zigzag incisions (Pieri principle) to create volar and dorsal triangular flaps.
- Neurovascular Dissection: Shared digital nerves must be carefully split longitudinally under loupe magnification to preserve innervation to both digits. Common digital arteries that bifurcate distally may require ligation of one branch; ensure the dominant vessel to the adjacent digit is preserved.
- Nail Matrix: If the nail is shared, a longitudinal strip of the nail and underlying matrix must be excised to create two appropriately sized, separate nail beds.
2. Commissure Reconstruction
The normal web commissure slopes from proximal-dorsal to distal-palmar. Recreating this slope is the most critical factor in preventing web creep. Local flaps are vastly superior to skin grafts for the base of the commissure.
* Dorsal Rectangular Flap: The workhorse flap. It begins at the transverse metacarpal ligament and extends distally. Vekris et al. demonstrated that dorsal rectangular flaps have a significantly lower revision rate (3%) compared to triangular flaps (63%).
* Butterfly Flap (Woolf and Broadbent): Highly effective for partial simple syndactyly ending proximal to the PIP joint. Flaps are designed in the web space to form a dorsal rectangle, which is then rotated to deepen the web.
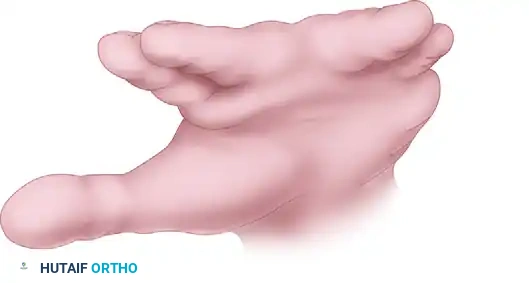
Figure: Woolf and Broadbent butterfly flap technique. Flaps are designed in the web space.
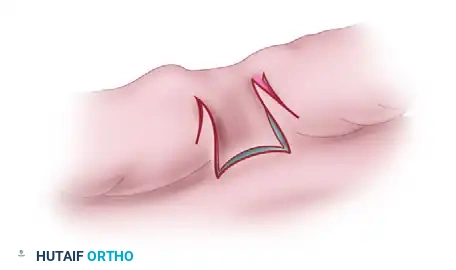
Figure: The butterfly flaps are rotated and interdigitated to deepen the web and recreate the commissure slope.
3. Resurfacing and Skin Grafting
- The zigzag incisions are designed so that the flaps interdigitate to close one digit primarily, while the adjacent digit requires skin grafting
Associated Surgical & Radiographic Imaging


You Might Also Like