Degenerative Disc Disease and Internal Disc Derangement: Comprehensive Surgical Guide
Key Takeaway
Internal disc derangement (IDD) is a primary source of discogenic axial spine pain, distinct from radiculopathy. Diagnosis requires a rigorous exclusion of structural instability and psychosocial confounders. Management begins with targeted nonoperative protocols. For refractory cases, surgical interventions such as lumbar fusion or disc arthroplasty may be indicated, though careful patient selection using psychological screening and diagnostic blocks is paramount to achieving optimal clinical outcomes.
PATHOPHYSIOLOGY OF DEGENERATIVE DISC DISEASE AND IDD
The degenerative process is fundamental to the development of various spinal pathologies, including disc herniations and axial back pain. Historically, mechanical wear and tear were considered the primary culprits; however, contemporary molecular and epidemiological research unequivocally demonstrates that genetic factors (such as polymorphisms in the aggrecan and collagen IX genes) play a far more dominant role than mechanical stresses.
The development of a frank disc herniation is merely one pathway a degenerating disc may follow. Alternatively, the intervertebral disc itself may become the primary nociceptive source—a condition distinct from the nerve root compression seen in herniations. This discogenic pain is primarily attributed to Internal Disc Derangement (IDD), a pathological cascade accompanying the degenerative process.
Current understanding defines IDD as a pathological condition resulting in axial spine pain with minimal to no deformation of spinal alignment or disc contour. This must be strictly distinguished from measurable instability caused by fractures, traumatic ligamentous disruptions, degenerative spondylolisthesis, or adult spinal deformity. While those conditions generate pain, they present with defined anatomical alterations and overt imaging abnormalities. IDD, conversely, lacks pathognomonic macroscopic findings, making it a diagnosis of exclusion that requires a meticulous compilation of clinical data.
NEUROANATOMY AND BIOMECHANICS OF DISCOGENIC PAIN
The anatomical basis for discogenic pain has been elucidated through the identification of nociceptive receptors within the outer annulus fibrosus. The intervertebral disc is innervated anteriorly and laterally by the sympathetic trunk, and posteriorly by the sinuvertebral nerve (of Luschka) and the basivertebral nerves.
As the disc degenerates, the molecular structure of the extracellular matrix degrades, leading to altered mechanical properties and aberrant cellular activities. This degradation stimulates neo-innervation and neo-vascularization deep into the inner annulus and nucleus pulposus, areas that are normally aneural and avascular. Inflammatory mediators, such as interleukins (IL-1, IL-6) and tumor necrosis factor-alpha (TNF-α), sensitize these nociceptors, converting normal mechanical loading into a painful stimulus.
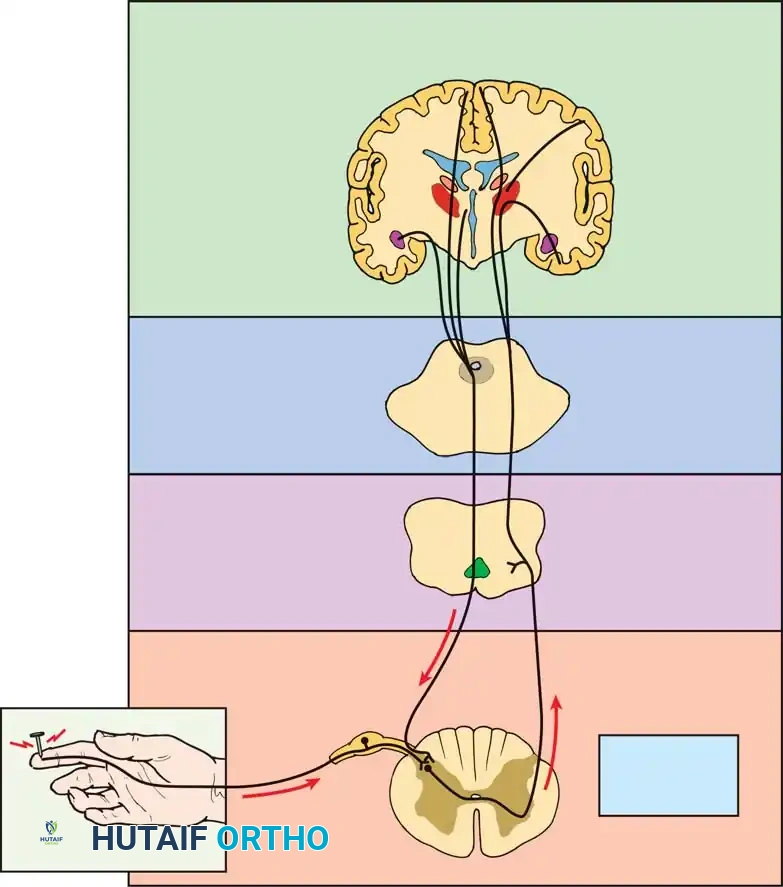
Understanding the complex interplay between peripheral nociception and central pain modulation is critical for rational treatment. Pain signals travel via C-fibers and A-delta fibers to the dorsal horn, ascending through the spinothalamic tract to supraspinal centers where complex psychosocial modulation occurs.
Fig. 39-44 Main anatomical areas of pain modulation. The interplay between peripheral nociception and supraspinal modulation dictates the clinical perception of discogenic pain.
CLINICAL EVALUATION AND DIAGNOSTIC CRITERIA
Because there are no definitive, universally accepted criteria for IDD, the diagnosis relies heavily on a consistent clinical history and the systematic elimination of other pathologies.
Patient History
Patients presenting with IDD are typically in their third to sixth decades of life. The pain is usually chronic, often present for several years, though it may have escalated to a constant or highly frequent state in recent months.
* Pain Character: Primarily axial low back pain.
* Referral Pattern: Often radiates to the buttock and posterior thigh (sclerotomal pain).
* Mechanical Exacerbation: Positions that increase intradiscal pressure—such as sitting, forward flexion, or lifting—markedly exacerbate symptoms.
* Relieving Factors: Recumbency, particularly in the fetal position, often decreases pain by unloading the disc.
Clinical Pearl: Pain radiating distal to the knee strongly indicates coexistent nerve root pathology (radiculopathy) rather than isolated IDD. Furthermore, pain that is entirely constant with absolutely no mechanical variation in intensity is rarely discogenic and warrants investigation for infectious, neoplastic, or visceral etiologies.
Physical Examination
If IDD is the sole diagnosis, the neurological examination (motor strength, sensory testing, and deep tendon reflexes) will be entirely normal.
* Range of Motion: Lumbar ROM is mildly limited, particularly in flexion, secondary to lumbosacral pain and hamstring tightness. Extension often provides temporary relief.
* Provocative Testing: Straight leg raising (SLR) may provoke back and buttock pain (due to dural tension transmitting force to the disc), but it will not produce sharp pain radiating below the knee.
* Palpation: Paraspinal muscle spasm is typically absent. The hip joints must be thoroughly examined to rule out intra-articular hip pathology as a source of buttock and thigh pain.
PSYCHOSOCIAL ASSESSMENT AND PATIENT SELECTION
The most critical phase in managing IDD, particularly when considering surgical intervention, is the evaluation of psychosocial factors. Patients with severe, debilitating axial spine pain without objective structural instability are at high risk for poor surgical outcomes if underlying psychological distress is ignored.
Waddell Signs of Abnormal Illness Behavior
Waddell et al. defined abnormal illness behavior as maladaptive overt behavior out of proportion to the underlying physical disease. The presence of three or more of the following signs suggests a nonorganic component to the pain:
1. Superficial/Nonanatomical Tenderness: Skin tenderness to light touch or widespread tenderness not localized to a single structure.
2. Simulation: Axial loading of the skull or en bloc rotation of the shoulders and pelvis eliciting severe lower back pain.
3. Distraction: Inconsistent findings, such as a positive supine SLR but a negative seated SLR (flip test).
4. Regional Disturbances: Widespread sensory changes or weakness diverging from accepted neuroanatomy (e.g., "stocking" numbness or giving way of the entire leg).
5. Overreaction: Disproportionate verbalization, facial expression, collapsing, or sweating during the exam.
Formal Psychological Testing
Before invasive diagnostic studies or surgery, formal psychological screening is mandatory.
* MMPI (Minnesota Multiphasic Personality Inventory): Patients with depressed-pathological profiles or a "conversion V" profile report significantly greater dissatisfaction with surgical outcomes.
* DRAM (Distress and Risk Assessment Method): A simpler alternative combining the Modified Somatic Perception Questionnaire and the Zung Depression Index. Patients identified as psychologically distressed are three to four times more likely to fail surgical treatment.
Surgical Warning: The presence of untreated severe depression, active secondary gain issues, or multiple Waddell signs is a strong relative contraindication to surgical intervention for IDD. Surgery in these patients yields a success rate far below the standard 65%.
DIAGNOSTIC IMAGING AND ADVANCED MODALITIES
Standard Radiography and MRI
Imaging begins with weight-bearing orthogonal and dynamic (flexion-extension) lumbar radiographs to rule out deformities, measurable instability (spondylolisthesis), or destructive lesions.
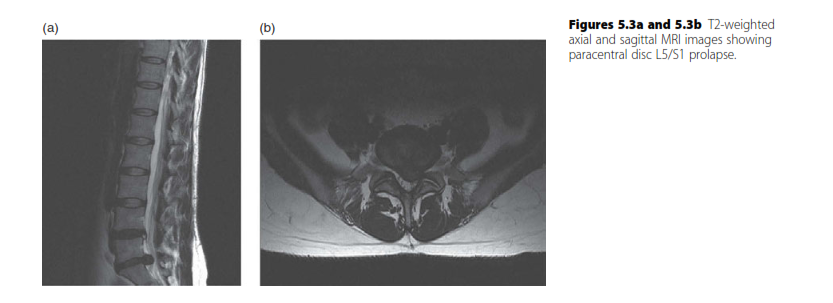
Magnetic Resonance Imaging (MRI) is the gold standard for evaluating disc hydration and morphology. In IDD, MRI typically reveals diminished water content in the nucleus pulposus, presenting as a "dark disc" on T2-weighted sagittal images. This may be accompanied by a loss of disc height and broad-based annular bulging.
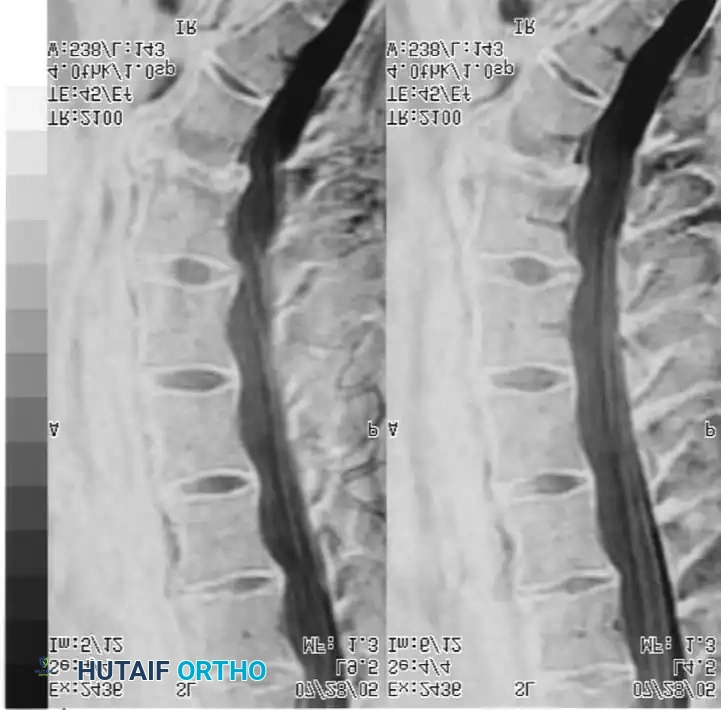
Fig. 39-45 MRI of a 51-year-old patient with chronic axial spine pain. Note the significant loss of signal intensity (dark disc) at the L5-S1 level on the T2-weighted sagittal image, indicative of severe desiccation and internal disc derangement.
It is imperative to understand that a dark disc on MRI has no diagnostic value in isolation. It must correlate perfectly with the clinical history and physical examination, as asymptomatic disc degeneration is highly prevalent in the general population.
Differential Spinal Anesthetic
When the diagnosis remains elusive, a differential spinal anesthetic can help isolate the pain generator. This technique relies on the relationship between nerve fiber size, myelination, and susceptibility to local anesthetics.
By sequentially administering varying concentrations of a local anesthetic (e.g., procaine) into the subarachnoid space, the physician can achieve a predictable sequence of blockade:
1. Sympathetic Blockade (B fibers): Achieved with the lowest concentration. If pain resolves, it suggests a sympathetically mediated pain syndrome.
2. Sensory Blockade (A-delta and C fibers): Achieved with a moderate concentration. If pain resolves here, it confirms a somatic nociceptive source (such as IDD).
3. Motor Blockade (A-alpha and A-beta fibers): Achieved with the highest concentration.
4. Placebo: Administration of normal saline to rule out psychogenic pain.
NONOPERATIVE MANAGEMENT PROTOCOL
The vast majority of patients with IDD can and should be managed nonoperatively. The cornerstone of this approach is patient education. Patients must understand that IDD is not relentlessly progressive and that chronic pain does not equate to impending paralysis or total disability.
A structured, active rehabilitation program is superior to passive modalities. The protocol should include:
* Activity Modification: Avoiding repetitive flexion and heavy axial loading.
* Aerobic Conditioning: Low-impact activities such as walking, stationary cycling, or aquatic therapy to improve blood flow and endorphin release.
* Core Strengthening: Dynamic lumbar stabilization exercises focusing on the transversus abdominis, multifidus, and pelvic floor musculature to reduce micro-motion across the degenerated segment.
SURGICAL MANAGEMENT: INDICATIONS AND TECHNIQUES
Surgical intervention is reserved for a small subset of patients with persistent, debilitating axial spine pain who have failed a minimum of 6 to 12 months of comprehensive nonoperative care, possess a favorable psychological profile, and have concordant pain confirmed by advanced diagnostics (such as provocative discography).
Patients must be counseled frankly: surgery for IDD yields significant improvement in only about 65% of cases. Approximately 35% will experience no improvement or may worsen. Furthermore, even successful cases will likely retain some degree of stiffness or activity limitation.
Surgical Options
Treatment options include:
1. Lumbar Interbody Fusion: The gold standard for definitive immobilization of the painful segment. Approaches include ALIF (Anterior), TLIF (Transforaminal), and PLIF (Posterior).
2. Total Disc Arthroplasty (TDA): Indicated strictly for isolated, single-level symptomatic DDD without facet arthropathy, aiming to preserve motion.
3. Dynamic Stabilization: Pedicle screw-based systems that restrict, but do not eliminate, segmental motion.
Step-by-Step Surgical Approach: Transforaminal Lumbar Interbody Fusion (TLIF)
For single-level IDD requiring fusion, the TLIF approach is highly effective, allowing for complete discectomy, interbody grafting, and robust pedicle screw fixation through a single posterior approach.
1. Preoperative Positioning and Setup
- The patient is intubated and positioned prone on a radiolucent Jackson table with a Wilson frame or chest/hip pads.
- The abdomen must hang free to decrease intra-abdominal pressure, thereby reducing epidural venous engorgement and intraoperative bleeding.
- All pressure points are meticulously padded.
- Intraoperative fluoroscopy is brought in to confirm the correct surgical level prior to incision.
2. Surgical Approach and Exposure
- A midline longitudinal incision is made over the target spinous processes.
- Subperiosteal dissection of the paraspinal musculature is performed bilaterally out to the tips of the transverse processes.
- Self-retaining retractors are placed to maintain exposure.
3. Facetectomy and Decompression
- A unilateral total facetectomy (inferior articular process of the cephalad vertebra and superior articular process of the caudal vertebra) is performed on the more symptomatic side.
- This provides access to the intervertebral disc space via the neuroforamen while minimizing retraction on the thecal sac and traversing nerve root.
- The ligamentum flavum is excised, and the exiting and traversing nerve roots are identified and protected.
4. Discectomy and Endplate Preparation
- An annulotomy is performed, and the degenerative nucleus pulposus is aggressively removed using pituitary rongeurs and curettes.
- Crucial Step: The cartilaginous endplates must be meticulously scraped down to bleeding subchondral bone using ring curettes and rasps. Inadequate endplate preparation is the leading cause of pseudoarthrosis.
- The disc space is sized, and an interbody cage packed with autograft (local bone from the facetectomy) and/or orthobiologics is impacted into the anterior third of the disc space to restore lordosis and foraminal height.
5. Pedicle Screw Instrumentation and Fluoroscopic Verification
- Pedicle screws are placed bilaterally into the cephalad and caudal vertebrae. The entry point is typically at the intersection of the pars interarticularis, the superior articular facet, and the transverse process.
- The pedicles are cannulated with a gearshift probe, palpated with a ball-tip feeler to ensure no cortical breaches, tapped, and the screws are inserted.
- Intraoperative fluoroscopy is absolutely critical during this phase to confirm trajectory and depth.

Intraoperative AP fluoroscopy demonstrating the initial placement and medial trajectory of the pedicle screws within the vertebral bodies.

Alternative AP fluoroscopic view confirming bilateral symmetry and appropriate convergence of the pedicle screws, ensuring they do not breach the medial pedicle wall into the spinal canal.
- Once screw placement is confirmed, titanium or cobalt-chrome rods are contoured to match the patient's natural lumbar lordosis and secured to the screw heads with set screws.
- Compression is applied across the construct to load the interbody cage, adhering to Wolff's Law to promote osteogenesis.
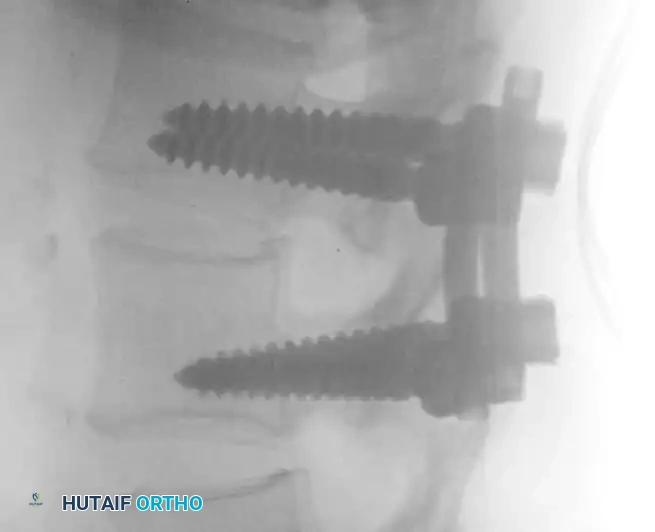
Lateral fluoroscopic view showing the depth of the pedicle screws. The screws should parallel the superior endplate and penetrate 50-80% into the vertebral body without breaching the anterior cortex.

Final lateral fluoroscopic image confirming excellent hardware placement, restoration of disc height, and appropriate sagittal alignment following final tightening of the construct.
6. Closure
- Posterolateral decortication of the transverse processes is performed, and remaining bone graft is laid down to encourage a posterolateral fusion mass.
- The wound is irrigated copiously with antibiotic saline.
- The fascia is closed tightly in a watertight fashion to prevent postoperative cerebrospinal fluid (CSF) leaks or fascial dehiscence. Subcutaneous tissues and skin are closed standardly.
POSTOPERATIVE PROTOCOL AND OUTCOMES
Postoperative management focuses on early mobilization and protecting the fusion construct.
* Day 0-1: Patients are mobilized out of bed with physical therapy. A rigid lumbar orthosis (TLSO) may be used for comfort and to restrict gross motion, though its necessity is debated in the era of rigid pedicle screw fixation.
* Weeks 2-6: Focus on walking and gentle nerve-gliding exercises. Bending, lifting (over 10 lbs), and twisting (BLT) are strictly prohibited.
* Months 3-6: Radiographs are obtained to assess fusion mass incorporation. Core stabilization exercises are initiated.
* Return to Work: Sedentary work may resume at 4-6 weeks. Heavy manual labor may require 6 months or longer, depending on radiographic evidence of solid arthrodesis.
Ultimately, the successful treatment of Internal Disc Derangement relies less on the specific surgical hardware utilized and more on the rigorous, evidence-based selection of the patient. By meticulously ruling out psychosocial confounders and confirming the disc as the primary pain generator, the orthopaedic surgeon can maximize the probability of a successful clinical outcome.
You Might Also Like