Traumatic Hip Dislocation: Epidemiology, Surgical Anatomy, and Clinical Principles
Key Takeaway
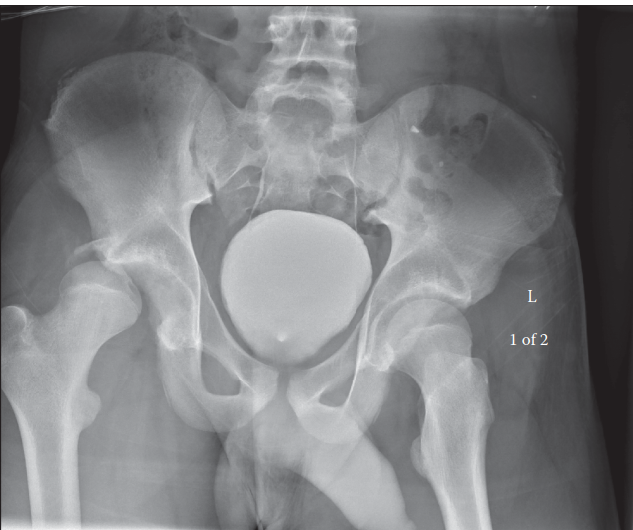
Traumatic hip dislocation is a profound orthopedic emergency where the femoral head forcefully separates from the acetabulum, typically due to high-energy trauma. Predominantly posterior (85-90%), it demands immediate recognition and reduction within 6 hours to prevent severe complications like avascular necrosis and post-traumatic osteoarthritis, critical for patient outcomes.
Hip Dislocation Due to Injury: Causes, Symptoms & Urgent Care
Introduction & Epidemiology
Traumatic hip dislocation represents a profound orthopedic emergency, demanding immediate recognition and expeditious management to optimize patient outcomes and mitigate the risk of severe complications. The hip joint, a diarthrodial enarthrodial (ball-and-socket) joint, is inherently stable due to its deep acetabular socket, robust capsuloligamentous structures, and surrounding powerful musculature. Consequently, dislocation typically necessitates the application of substantial kinetic energy, most commonly observed in high-energy trauma mechanisms such as motor vehicle collisions (MVCs), falls from significant height, or high-impact sports injuries.

A hip dislocation occurs when the femoral head is forcefully expelled from its normal articulation within the acetabular fossa. The direction of dislocation is critical for classification and management strategies. Posterior dislocations constitute the vast majority (85-90%) of traumatic hip dislocations, typically resulting from an axial load applied to a flexed, adducted, and internally rotated hip (e.g., dashboard injury in MVCs). Anterior dislocations are far less common (5-10%), usually occurring with the hip in abduction and external rotation, often associated with a direct blow to the posterior aspect of the hip or a hyperabduction injury. Central dislocations, characterized by an impaction fracture of the acetabular floor, involve medial protrusion of the femoral head into the pelvis and are technically a type of acetabular fracture rather than a true dislocation, though they share some clinical features.
The epidemiology of traumatic hip dislocation reflects its high-energy etiology. It predominantly affects young, active individuals involved in MVCs. The widespread adoption of seatbelt use has demonstrably reduced the incidence of posterior hip dislocations in MVCs, though injuries remain significant when they occur, often in conjunction with other severe polytrauma. Prompt reduction, ideally within 6 hours of injury, is universally recognized as a critical determinant in reducing the incidence of debilitating sequelae, particularly avascular necrosis (AVN) of the femoral head and post-traumatic osteoarthritis (PTOA). The severity of force required frequently leads to concomitant injuries, including acetabular fractures, femoral head fractures (Pipkin classification), femoral shaft fractures, ipsilateral knee injuries, and neurovascular compromise, most notably sciatic nerve palsy.
Surgical Anatomy & Biomechanics
A comprehensive understanding of the hip joint's complex surgical anatomy and biomechanics is fundamental for effective management of traumatic dislocations.
Bony Structures
-
Acetabulum:
A hemispherical socket formed by the fusion of the ilium, ischium, and pubis. Key features include:
- Lunate Surface: The articular cartilage-lined, C-shaped weight-bearing portion of the acetabulum.
- Acetabular Fossa: The non-articular central depression containing the ligamentum teres and fat pad.
- Acetabular Rim: The bony circumference defining the opening of the socket, discontinuous inferiorly at the acetabular notch.
- Anterior and Posterior Columns: Structural buttresses of the pelvis. The anterior column extends from the anterior superior iliac spine (ASIS) to the pubic symphysis, while the posterior column extends from the ischial tuberosity to the posterior iliac crest. Fractures of these columns are critical in acetabular fracture classifications.
- Anterior and Posterior Walls: Segments of the acetabular rim. Posterior wall fractures are common associated injuries with posterior hip dislocations.
-
Femoral Head:
A spherical structure comprising approximately two-thirds of a sphere, articulating with the lunate surface of the acetabulum.
- Fovea Capitis: A small depression on the femoral head for the attachment of the ligamentum teres, which houses a branch of the obturator artery (artery to the head of the femur).
Ligamentous Structures
These ligaments contribute significantly to the static stability of the hip joint, particularly in extension.
*
Iliofemoral Ligament (Y-ligament of Bigelow):
The strongest ligament of the hip, situated anteriorly, originating from the anterior inferior iliac spine (AIIS) and acetabular rim, bifurcating to insert onto the intertrochanteric line of the femur. It resists hyperextension and external rotation.
*
Pubofemoral Ligament:
Located anteroinferiorly, originating from the superior ramus of the pubis and blending with the capsule and iliofemoral ligament. It limits abduction and external rotation.
*
Ischiofemoral Ligament:
Positioned posteriorly, arising from the ischium posterior to the acetabulum and spiraling superolaterally to the greater trochanter and zona orbicularis. It limits internal rotation and extension.
*
Ligamentum Teres (Ligament of the Head of the Femur):
Intracapsular, connecting the fovea capitis to the acetabular fossa. Its primary role in stability is debated, but it contains a small arterial branch (artery to the head of the femur), which contributes to the vascular supply of the femoral head, particularly in pediatric patients. It can be a source of blood supply for the femoral head after fracture or dislocation.
Joint Capsule
A robust, fibrous capsule encircles the hip joint, attaching proximally to the acetabular rim and distally to the intertrochanteric line anteriorly and the femoral neck posteriorly. The capsular fibers, particularly the zona orbicularis, contribute to stability by constricting the femoral neck.
Musculature
Dynamic stability is provided by the powerful musculature surrounding the hip:
*
Gluteal Muscles (Maximus, Medius, Minimus):
Major abductors and extensors.
*
Adductor Group (Longus, Brevis, Magnus, Pectineus, Gracilis):
Adduct and flex the hip.
*
Hamstrings (Semimembranosus, Semitendinosus, Biceps Femoris):
Extend the hip and flex the knee.
*
Quadriceps Femoris:
Extends the knee, rectus femoris flexes the hip.
*
Short External Rotators (Piriformis, Superior and Inferior Gemelli, Obturator Internus, Quadratus Femoris):
Deep to the gluteus maximus, these muscles are often injured or avulsed in posterior dislocations.
Neurovascular Structures
Critical structures in close proximity to the hip joint include:
*
Sciatic Nerve:
Exits the pelvis through the greater sciatic notch, deep to the piriformis muscle. It is highly vulnerable in posterior hip dislocations and posterior acetabular fractures.
*
Femoral Nerve:
Lies anterior to the hip joint, typically safe in posterior dislocations but at risk in anterior approaches.
*
Obturator Nerve:
Medial to the hip joint, generally protected.
*
Vascular Supply:
The femoral head receives its primary blood supply from the medial and lateral circumflex femoral arteries, which form an extracapsular ring around the femoral neck and give rise to retinacular arteries. Disruption of these retinacular vessels, particularly in the superior and posterior aspects, is a major contributing factor to AVN following dislocation.
Biomechanics of Stability and Dislocation
The inherent stability of the hip joint is a function of:
1.
Bony Congruence:
Deep acetabular socket encompassing a large portion of the femoral head.
2.
Labrum:
The fibrocartilaginous rim enhances socket depth and creates a suction seal.
3.
Capsuloligamentous Restraints:
Provide passive stability, especially at end-range motions.
4.
Muscular Dynamics:
Active stabilization during movement and weight-bearing.
Mechanisms of Dislocation:
*
Posterior Dislocation:
Occurs with the hip flexed, adducted, and internally rotated, and an axial load directed through the femur. This drives the femoral head posteriorly, tearing the posterior capsule and often avulsing the short external rotators. Associated injuries frequently include posterior acetabular wall fractures, Pipkin fractures (femoral head fractures), or sciatic nerve injury.
*
Anterior Dislocation:
Less common, typically involves forced abduction and external rotation of the hip, often with extension. The femoral head is driven anteriorly, tearing the anterior capsule and iliofemoral ligament. Associated injuries can include anterior acetabular rim fractures or femoral head impression fractures.
*
Central Dislocation (Acetabular Impaction Fracture):
A direct lateral blow to the greater trochanter or an axial load on an abducted hip can drive the femoral head medially, fracturing the acetabular floor.
Indications & Contraindications
The management of traumatic hip dislocations prioritizes prompt reduction. The decision between closed and open reduction, and whether surgical fixation of associated injuries is required, is based on a meticulous assessment of the injury pattern and joint stability.
Non-Operative Indications
Closed reduction under adequate sedation or general anesthesia is the primary management for the vast majority of traumatic hip dislocations.
*
Isolated Simple Hip Dislocation:
No associated fractures of the femoral head or acetabulum that significantly compromise joint stability or require surgical fixation.
*
Concentric Reduction Achieved:
Radiographic confirmation (post-reduction AP pelvis and lateral views) demonstrating that the femoral head is fully seated within the acetabulum with appropriate joint space.
*
Stable Reduction:
Clinical assessment of the hip's stability after reduction, although this can be challenging to reliably determine in the acute setting without fluoroscopy or further imaging.
*
No Incarcerated Fragments:
Absence of intra-articular bony fragments, labral tissue, or capsular interposition preventing concentric reduction, as confirmed by post-reduction imaging (CT scan).
Operative Indications
Surgical intervention, typically open reduction with or without internal fixation (ORIF), is indicated in specific scenarios:
*
Irreducible Dislocation:
Failure to achieve concentric reduction after one or two attempts at closed reduction. This often suggests soft tissue interposition (labrum, capsule, ligamentum teres, piriformis, rectus femoris) or incarcerated bony fragments.
*
Non-Concentric Reduction:
Post-reduction imaging (especially CT) reveals a persistent joint space abnormality, indicating incomplete reduction or intra-articular debris.
*
Associated Acetabular Fractures Requiring ORIF:
*
Posterior Wall Fractures:
Especially those involving >40% of the posterior wall, or cases with instability after reduction.
*
Posterior Column Fractures:
Particularly if they compromise weight-bearing dome integrity or result in instability.
*
Anterior Wall/Column Fractures:
Depending on displacement and stability.
*
Transverse/T-type Fractures:
Often require ORIF.
*
Associated Femoral Head Fractures (Pipkin Classification):
*
Pipkin Type II:
Femoral head fracture involving the weight-bearing portion of the head, requiring anatomical reduction and stable fixation to prevent PTOA.
*
Pipkin Type III/IV:
Femoral head fracture with associated acetabular fracture.
*
Delayed Presentation:
While not a direct indication for open reduction, a prolonged time to reduction (e.g., >6-8 hours) increases the risk of AVN, and some surgeons may advocate for open reduction in certain delayed cases to ensure complete debridement and inspection, though closed reduction should still be attempted if feasible.
*
Associated Neurovascular Injury Requiring Exploration:
Rarely, vascular injury (e.g., femoral artery) may necessitate immediate surgical exploration. Sciatic nerve palsy is typically managed expectantly but can sometimes accompany complex injuries requiring open reduction.
*
Recurrent Dislocations:
Although rare after an initial traumatic event, recurrent dislocations may necessitate surgical stabilization, including capsular repair/plication, or even total hip arthroplasty in elderly patients with poor tissue quality.
Contraindications
- Absolute Contraindications: There are no absolute contraindications to reduction of a traumatic hip dislocation. The urgency of reduction outweighs nearly all other concerns.
- Relative Contraindications to Closed Reduction: Obvious large bony fragment blocking reduction (often necessitating open reduction), or severe patient comorbidities that preclude general anesthesia (though local nerve blocks can facilitate reduction).
- General Medical Instability: While reduction is urgent, the patient's overall medical status must be optimized. Polytrauma patients may require initial stabilization of life-threatening injuries before proceeding with reduction, though this should not significantly delay hip reduction.
Operative vs. Non-Operative Indications for Traumatic Hip Dislocation
| Indication Type | Non-Operative (Closed Reduction Primary) | Operative (Open Reduction &/or ORIF) |
|---|---|---|
| Dislocation Status | Isolated simple dislocation | Irreducible dislocation after failed closed attempts |
| Concentric reduction achieved post-attempt | Non-concentric reduction (e.g., incarcerated fragment) | |
| Associated Fractures | No significant associated fractures | Acetabular fracture (e.g., >40% posterior wall, displaced column fracture) requiring fixation |
| Femoral head fracture (Pipkin Type II, III, IV) | ||
| Femoral neck fracture (rarely co-occurs, but would necessitate fixation) | ||
| Timing | Early presentation (<6-8 hours) | Delayed presentation (though closed reduction should still be attempted) |
| Neurovascular Status | No acute neurovascular deficit | Acute vascular injury requiring exploration |
| Stability | Stable after closed reduction | Gross instability after reduction (e.g., due to significant soft tissue/bony defect) |
| Recurrence | First-time dislocation | Recurrent traumatic dislocations (may require capsular repair/bone grafting) |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is essential for successful management, especially when surgical intervention is anticipated. This phase extends beyond immediate reduction to potential definitive fixation.
Diagnostic Workup
- Clinical Assessment: Rapid assessment for neurovascular deficits (particularly sciatic nerve palsy) and associated injuries. Limb position is a crucial diagnostic clue (flexed, adducted, internally rotated for posterior; flexed, abducted, externally rotated for anterior).
-
Radiographs:
- AP Pelvis: Initial view to identify dislocation direction, associated acetabular or femoral head fractures.
- Judet Views (Obturator Oblique, Iliac Oblique): Essential for detailed evaluation of acetabular columns and walls, guiding fracture classification and surgical planning if fractures are present.
- Lateral Hip View: Confirms dislocation direction and assesses for any anterior/posterior displacement.
- Post-Reduction Radiographs: Absolutely critical to confirm concentric reduction.
-
Computed Tomography (CT) Scan:
-
Mandatory Post-Reduction:
Even after apparently successful closed reduction, a CT scan is imperative to:
- Confirm perfect concentricity of reduction.
- Identify any incarcerated intra-articular fragments (labrum, capsule, bony fragments) that might impede healing or predispose to AVN or PTOA.
- Precisely characterize any associated acetabular or femoral head fractures, including fracture morphology, displacement, and joint involvement, which will dictate the need for and approach to ORIF.
- Assess for occult fractures not evident on plain radiographs.
-
Mandatory Post-Reduction:
Even after apparently successful closed reduction, a CT scan is imperative to:
- Magnetic Resonance Imaging (MRI): Not typically indicated in the acute setting. May be used later for evaluating soft tissue injuries (labrum, cartilage), assessing for early AVN, or identifying post-traumatic complications.
Timing
The overarching principle is expeditious reduction . The risk of femoral head AVN increases significantly with every hour of dislocation. Aim for reduction within 6 hours. If closed reduction fails, urgent open reduction should follow.
Anesthesia
- Closed Reduction: Requires adequate muscle relaxation and analgesia. General anesthesia is preferred. In an emergency setting, deep conscious sedation (e.g., procedural sedation) with appropriate monitoring can be employed. Regional nerve blocks (femoral nerve block, fascia iliaca block) can provide effective analgesia but usually do not provide sufficient muscle relaxation alone.
- Open Reduction/ORIF: General anesthesia is typically used, allowing for full muscle relaxation and surgical access.
Patient Positioning
-
For Closed Reduction:
- Allis Maneuver: Patient supine. An assistant stabilizes the pelvis (e.g., applying countertraction to ASIS). The surgeon flexes the hip and knee to 90 degrees, applies gentle axial traction to the femur, and then performs external/internal rotation or gentle adduction/abduction as needed. For posterior dislocation, often gentle internal rotation and slight adduction may be used to clear the acetabular rim, followed by gentle traction and external rotation.
- Stimson Maneuver: Patient prone with the injured leg hanging over the edge of the table. A weight (e.g., 10-20 lbs) is applied to the ankle. After several minutes, the surgeon gently rotates the hip or applies direct pressure to the greater trochanter. This technique relies on gravity and muscle fatigue.
-
For Open Reduction/ORIF:
- Posterior Approach (e.g., Kocher-Langenbeck): Patient typically placed in the lateral decubitus position with the injured hip superior, stabilized with bolsters or a beanbag. This allows excellent exposure of the posterior acetabulum and proximal femur. Alternatively, a prone position can be used.
- Anterior Approach (e.g., Iliofemoral, Smith-Petersen): Patient supine. May utilize a traction table or specific bolsters to aid exposure and manipulation.
- Surgical Draping: Ensure sufficient sterile field to allow for full range of motion of the hip during reduction attempts and for fluoroscopic imaging.
Surgical Team & Equipment
- Surgical Team: Experienced orthopedic surgeon, residents, surgical assistants, anesthesia provider.
-
Equipment:
- Fluoroscopy: Essential for confirming reduction, assessing fracture fragments, and guiding screw placement during ORIF.
- Standard Orthopedic Instrument Set: Including various retractors (e.g., Hohmann, cobra, blunt), reduction clamps (e.g., Verbrugge, Farabeuf), bone hooks, periosteal elevators, osteotomes.
- Specific Implants for ORIF: Lag screws, buttress plates (e.g., reconstruction plates), appropriate drill bits, depth gauges, and screwdrivers.
- Neurophysiological Monitoring: Consider intraoperative neuromonitoring for sciatic nerve function during posterior approaches, especially in complex cases or those with pre-existing neuropraxia.
Detailed Surgical Approach / Technique
When closed reduction fails or associated injuries necessitate open reduction and internal fixation (ORIF), the surgical approach is dictated by the direction of dislocation and the specific fracture pattern. The most common scenario requiring open intervention is irreducible posterior dislocation, often with an associated posterior wall or femoral head fracture.

Posterior Dislocation - Kocher-Langenbeck Approach (Posterior Approach)
This is the workhorse approach for posterior acetabular fractures and irreducible posterior hip dislocations.
- Incision: A curvilinear or straight longitudinal incision is made, centered over the greater trochanter. It typically extends approximately 8-10 cm proximally from the tip of the greater trochanter along the line of the gluteus maximus fibers towards the posterior superior iliac spine, and 8-10 cm distally along the line of the femoral shaft.
-
Superficial Dissection:
- The skin and subcutaneous tissues are incised.
- The fascia lata is identified and incised longitudinally in line with the skin incision, exposing the underlying gluteus maximus muscle.
- The gluteus maximus muscle fibers are then split bluntly in line with their orientation.
-
Deep Dissection & Exposure:
- Deep to the gluteus maximus, the short external rotators (piriformis, superior gemellus, obturator internus, inferior gemellus, quadratus femoris) are identified. The piriformis is typically the most superior and largest of these muscles, exiting the greater sciatic notch.
- Sciatic Nerve Protection: Paramount importance. The sciatic nerve emerges from the pelvis deep to the piriformis muscle. It is identified, carefully protected, and gently retracted, usually medially, throughout the entire procedure. A blunt retractor or umbilical tape can be used to isolate it.
- The tendons of the short external rotators (excluding the quadratus femoris, which lies more distally) are carefully detached from their insertions on the greater trochanter. These tendons are tagged with heavy non-absorbable sutures to facilitate later repair. The interval between the piriformis and gluteus medius is developed superiorly.
- The posterior hip capsule is now exposed.
-
Reduction & Inspection:
- If the hip is still dislocated, the capsule will often be torn. The surgeon can directly visualize the femoral head and the acetabular socket.
- Identify and Remove Incarcerated Fragments: Crucially, any incarcerated soft tissue (labrum, capsule) or bony fragments (from the femoral head or acetabulum) blocking reduction must be identified and meticulously removed. A small osteotome or curette may be needed for bony fragments.
- Femoral Head Reduction: Using bone hooks placed in the fovea or reduction clamps on the femoral neck, combined with appropriate traction and rotation, the femoral head is maneuvered back into the acetabulum under direct vision. Ensure a smooth reduction without excessive force to prevent iatrogenic injury.
- Assessment of Associated Fractures: Once reduced, the acetabular posterior wall and any femoral head fractures are thoroughly inspected. If a posterior wall fracture is present, its size, comminution, and displacement are assessed.
-
Internal Fixation (if indicated):
- Posterior Wall Fractures: Fragments are anatomically reduced using reduction clamps (e.g., Farabeuf, Matta, pointed reduction clamps). Provisional fixation with K-wires is often employed. Definitive fixation typically involves lag screws for larger fragments and/or a buttress plate (e.g., 3.5mm reconstruction plate) contoured to the posterior column, placed along the posterior aspect of the acetabulum to prevent posterior displacement. Ensure screws are bicortical where possible and do not penetrate the joint.
- Femoral Head Fractures (Pipkin Type II): Requires direct visualization. The fragment is reduced and fixed with headless compression screws (e.g., cannulated lag screws) placed from the non-articular part of the femoral head into the fragment. Care is taken to ensure the screw heads are countersunk below the cartilage surface to prevent impingement or cartilage damage.
-
Capsular & Rotator Repair:
- The posterior hip capsule, if torn, can be repaired with non-absorbable sutures to enhance stability.
- The short external rotator tendons are reattached to the greater trochanter using the previously placed sutures. This helps restore muscle function and contributes to posterolateral stability.
- Stability Testing: The hip is gently taken through a controlled range of motion (flexion, extension, abduction, adduction, internal/external rotation) to assess stability and identify any impingement. Dynamic fluoroscopy can be helpful here.
- Closure: Layered closure, ensuring meticulous hemostasis. The gluteus maximus fascia is closed, followed by subcutaneous tissue and skin. A drain may be placed, though its routine use is debated.
Anterior Dislocation - Iliofemoral (Smith-Petersen) or Modified Hueter Approach
Less common, but indicated for irreducible anterior dislocations or associated anterior acetabular fractures.
- Incision: A longitudinal incision centered over the anterior superior iliac spine (ASIS), extending distally along the anterior aspect of the thigh for 10-15 cm.
-
Superficial Dissection:
- Skin and subcutaneous tissues are incised.
- Lateral Femoral Cutaneous Nerve Protection: The nerve typically crosses the sartorius muscle approximately 2-3 cm distal to the ASIS and is highly variable. It should be identified and carefully protected, often retracted medially.
- The fascia over the sartorius muscle (medially) and tensor fascia lata (laterally) is incised.
-
Interval Development:
- The iliofemoral interval (between the sartorius and tensor fascia lata) is developed. The sartorius is retracted medially, and the tensor fascia lata is retracted laterally.
- The rectus femoris muscle is identified. Its direct head originates from the AIIS and its reflected head from the ilium just superior to the acetabulum. The ascending branch of the lateral femoral circumflex artery typically crosses the rectus femoris and needs to be ligated or cauterized.
- The rectus femoris muscle is released from its origin at the AIIS (and often its reflected head) and reflected distally, exposing the underlying hip capsule and anterior aspect of the acetabulum.
-
Reduction & Inspection:
- The anterior hip capsule is exposed. Any torn capsule or incarcerated fragments (e.g., labrum, femoral head impression fracture fragments) are identified and removed.
- Reduction is performed under direct visualization, often with gentle traction, slight flexion, and internal rotation to reduce the femoral head back into the acetabulum.
-
Internal Fixation (if indicated):
- If an anterior wall or column fracture is present, similar reduction and fixation principles apply, often using lag screws and/or reconstruction plates.
- Capsular Repair & Closure: The capsule can be repaired. The rectus femoris is reattached to its origin. Layered closure.
Complications & Management
Traumatic hip dislocations, even with prompt and successful reduction, are associated with a significant risk of long-term complications. Vigilant post-operative monitoring and timely intervention are crucial.
Common Complications & Salvage Strategies
| Complication | Incidence (%) | Risk Factors | Clinical Presentation | Management / Salvage Strategy |
|---|---|---|---|---|
| Avascular Necrosis (AVN) of Femoral Head | 5-40 | Delayed reduction (>6-8 hours), severity of initial trauma, multiple reduction attempts, associated femoral neck/head fractures | Persistent groin pain, limp, collapse of femoral head on imaging (late) | Early: Protected weight-bearing, core decompression, vascularized fibular graft. Late: Osteotomy, total hip arthroplasty (THA). |
| Post-Traumatic Osteoarthritis (PTOA) | 20-70 | Chondral damage at initial injury, AVN, inadequate reduction, associated acetabular/femoral head fractures, residual instability | Chronic hip pain, stiffness, reduced ROM, crepitus | Conservative: Activity modification, NSAIDs, physical therapy. Surgical: Arthroscopy (debridement), osteotomy, THA. |
| Sciatic Nerve Injury | 10-20 | Posterior dislocation, complex fracture, iatrogenic injury during reduction/surgery | Foot drop (peroneal division), sensory loss (dorsum of foot, lateral calf) | Acute: Observation, neurolysis if entrapped. Chronic: AFO for foot drop, tendon transfers for muscle imbalance. Prognosis variable. |
| Recurrent Dislocation | 2-5 | Inadequate initial reduction, severe soft tissue disruption, unaddressed bony defects, generalized ligamentous laxity, patient non-compliance | Sudden onset of hip pain and deformity after minor trauma | Conservative: Activity modification, bracing. Surgical: Capsular plication/repair, bony augmentation, conversion to THA (rare). |
| Heterotopic Ossification (HO) | 10-20 | Open reduction, head injury, prolonged immobilization, associated trauma | Reduced ROM, pain, palpable mass, radiographic ossification | Prophylaxis: NSAIDs (Indomethacin), single-dose radiation therapy. Management: Excision if symptomatic and mature. |
| Infection | <1-5 | Open reduction, prolonged surgery, patient comorbidities, wound contamination | Fever, redness, swelling, purulent discharge, pain | Debridement, irrigation, intravenous antibiotics. May require implant removal. |
| DVT/Pulmonary Embolism (PE) ** | Variable | Trauma, surgery, immobilization, obesity, smoking, hypercoagulable states | Swelling/pain in calf, chest pain, dyspnea, tachycardia | Prophylaxis: Chemical (LMWH/DOACs) & mechanical (SCDs). Management: Anticoagulation. |
| Femoral Head Fracture (Pipkin) | 5-10 | High-energy impact, direct impaction of femoral head against acetabulum | Hip pain, crepitus, mechanical symptoms | Anatomical reduction and internal fixation (headless compression screws) for displaced fragments. |
| Acetabular Fractures | 20-50 | Very high-energy trauma, often posterior wall or column | Hip pain, instability, crepitus | ORIF as per fracture classification and stability criteria. |
Note: Incidences vary widely across studies depending on patient population, mechanism of injury, and definition of complications.
Detailed Management Considerations
- Avascular Necrosis (AVN): This remains the most feared long-term complication. It results from disruption of the femoral head's vascular supply, particularly the retinacular vessels. Risk is directly correlated with time to reduction and the severity of initial trauma. Clinical presentation is often delayed, with groin pain and limp becoming apparent months to years post-injury. Early detection often relies on MRI (T1-weighted sequences showing low signal changes). Management depends on the stage of AVN. Early stages (pre-collapse) may be treated with protected weight-bearing, core decompression, or vascularized fibular grafting. Once collapse occurs, arthroplasty (THA) is typically the definitive treatment.
- Post-Traumatic Osteoarthritis (PTOA): Develops due to articular cartilage damage at the time of injury, inadequate reduction, or subsequent AVN. It can manifest even after successful reduction and healing. Management starts conservatively with pain management and activity modification. As symptoms progress and function declines, surgical options range from arthroscopic debridement to osteotomy and, ultimately, THA.
- Sciatic Nerve Injury: The sciatic nerve is vulnerable in posterior dislocations, particularly the peroneal division. It can be stretched, contused, or, rarely, transected. Most cases are neuropraxia or axonotmesis and resolve spontaneously over weeks to months. Management is typically expectant, with neurophysiological studies (EMG/NCS) aiding in prognosis and differentiation. Surgical exploration may be considered if nerve entrapment is suspected or for complete transection, though outcomes are variable. An ankle-foot orthosis (AFO) can manage foot drop.
- Recurrent Dislocation: Although rare, it indicates persistent instability. Causes include unaddressed posterior wall defects, insufficient capsular or muscular repair, or generalized ligamentous laxity. Surgical management may involve capsular plication, reconstruction of deficient bony structures, or conversion to THA in select cases.
- Heterotopic Ossification (HO): The formation of mature lamellar bone in soft tissues where bone does not normally exist. Risk factors include open reduction, associated head injury, and certain genetic predispositions. Prophylaxis with NSAIDs (e.g., Indomethacin) or a single low dose of post-operative radiation therapy is effective. If symptomatic and mature, surgical excision may be performed.
- DVT/PE: The risk of venous thromboembolism is elevated in trauma patients, especially with lower extremity injuries and prolonged immobilization. Prophylaxis with low-molecular-weight heparin (LMWH) or direct oral anticoagulants (DOACs) combined with mechanical compression devices is standard.
- Associated Fractures: Femoral head (Pipkin) and acetabular fractures significantly complicate management and outcomes. Anatomical reduction and rigid internal fixation are paramount to restore joint congruity and stability and minimize the risk of PTOA.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following traumatic hip dislocation, particularly after open reduction or ORIF, is critical for optimizing functional recovery, protecting surgical repairs, and mitigating long-term complications. Protocols must be tailored to the specific injury (e.g., simple dislocation vs. associated acetabular/femoral head fracture) and the surgeon's preferences.
Phase I: Immediate Post-Op – Protection Phase (Weeks 0-6)
Goals:
* Protect surgical repair and reduction stability.
* Manage pain and swelling.
* Initiate gentle range of motion (ROM) within protected limits.
* Prevent complications (DVT, HO).
Key Interventions:
*
Weight-Bearing (WB) Restrictions:
*
Simple Dislocation (Closed Reduction Only):
Touch-down weight-bearing (TDWB) or weight-bearing as tolerated (WBAT) with crutches, often for 4-6 weeks, if no significant associated fracture and stability is confirmed.
*
Open Reduction/Associated Fractures (ORIF):
Typically non-weight bearing (NWB) or TDWB for 6-12 weeks to allow for bone/soft tissue healing and fracture consolidation. This is especially crucial for acetabular or femoral head fractures.
*
Range of Motion (ROM) Restrictions:
*
Posterior Dislocation/Approach:
Avoid hip flexion beyond 70-90 degrees, adduction past neutral, and internal rotation for 6-12 weeks. An abduction pillow or brace may be prescribed, particularly at night.
*
Anterior Dislocation/Approach:
Avoid excessive hip extension and external rotation.
*
Controlled Motion:
Gentle active-assisted and passive ROM within protected ranges. Continuous Passive Motion (CPM) devices may be used but have unproven efficacy for hip.
*
Exercises:
* Ankle pumps, quadriceps sets, gluteal sets to maintain muscle tone and prevent DVT.
* Gentle core stabilization exercises.
* Upper extremity conditioning for crutch ambulation.
*
Pain & Swelling Management:
Analgesics, cryotherapy, compression.
*
DVT Prophylaxis:
Continue pharmacological and mechanical prophylaxis.
*
HO Prophylaxis:
If used, continue NSAIDs or follow radiation protocol.
Phase II: Intermediate Phase – Gradual Progression (Weeks 6-12)
Goals:
* Gradually increase weight-bearing.
* Restore functional ROM.
* Initiate light strengthening exercises.
* Improve neuromuscular control.
Key Interventions:
*
Weight-Bearing Progression:
Progress from TDWB to partial weight-bearing (PWB) and then to full weight-bearing (FWB) as tolerated, guided by clinical signs of healing (pain, stability) and radiographic evidence of fracture consolidation (if applicable). Use of crutches or a walker gradually weaned.
*
Range of Motion:
Progressively increase hip ROM within pain limits, gradually removing previous restrictions.
*
Strengthening:
* Begin isometric hip strengthening (flexors, extensors, abductors, adductors) in all planes.
* Initiate isotonic exercises with light resistance (e.g., resistance bands, low weights) for hip and knee musculature.
* Light closed-chain exercises (e.g., mini-squats, lunges) as weight-bearing tolerance improves.
*
Proprioception/Balance:
Begin single-leg balance exercises.
*
Gait Training:
Focus on normal gait mechanics without assistive devices.
Phase III: Advanced Strengthening & Return to Activity (Weeks 12-24+)
Goals:
* Achieve full, pain-free ROM and strength.
* Improve endurance and power.
* Progress to sport-specific training (if applicable).
* Facilitate safe return to activities of daily living (ADLs) and recreational activities.
Key Interventions:
*
Weight-Bearing:
Full weight-bearing without assistive devices.
*
Strengthening:
* Progressive resistance exercises for all major hip muscle groups, increasing intensity and load.
* Eccentric strengthening.
* Plyometric exercises (jumping, hopping) for athletes.
* Functional exercises: Step-ups, lateral stepping, agility drills.
*
Cardiovascular Conditioning:
Cycling, swimming, elliptical trainer.
*
Sport-Specific Training:
Gradually introduce activities relevant to the patient's desired sport or occupation, focusing on proper mechanics and controlled movements.
*
Return to Activity:
Return to high-impact or demanding activities is highly individualized, generally not before 6 months, and often up to 12 months, depending on the severity of the injury, surgical intervention, and patient's recovery. Clinical assessment, strength testing, and functional performance metrics guide this decision.
Long-Term Considerations
- Monitoring for Complications: Patients must be educated about the signs and symptoms of AVN (groin pain, limp) and PTOA (chronic pain, stiffness) and followed clinically and radiographically for up to 2 years (or longer for AVN) to detect these late complications.
- Patient Education: Emphasize the importance of adherence to rehabilitation protocols, activity modification, and the potential for long-term sequelae.
Summary of Key Literature / Guidelines
The management of traumatic hip dislocations is largely guided by a robust body of literature emphasizing the critical role of prompt reduction and careful assessment for associated injuries.
1. Urgency of Reduction:
* Consensus is unequivocal:
Hip dislocations are orthopedic emergencies.
Numerous studies (e.g., those by Epstein, Mehlman, Hougaard and Thomsen) have consistently demonstrated a strong inverse correlation between the time to reduction and the incidence of avascular necrosis (AVN) of the femoral head. While various thresholds have been cited, reduction within
6 hours
is widely regarded as the target to significantly minimize AVN risk, with the risk escalating rapidly beyond this timeframe. Some literature suggests benefits even beyond 6 hours, advocating for reduction at any time if viable.
2. Imaging Protocols:
*
Initial Radiographs:
AP pelvis and Judet views are standard for evaluating the dislocation and any gross bony injuries. Lateral views confirm direction.
*
Post-Reduction CT Scan:
Strongly recommended and considered standard of care
following all closed hip reductions. The primary role of CT is to:
* Confirm absolute concentricity of the reduction.
* Identify incarcerated intra-articular fragments (bony, labral) that may impede healing, contribute to PTOA, or suggest the need for open reduction. Studies show a significant percentage of successfully reduced hips harbor intra-articular fragments detectable only on CT.
3. Indications for Open Reduction:
* The primary indications for open reduction include
failure of closed reduction
(suggesting soft tissue or bony interposition) and
non-concentric reduction
as confirmed by post-reduction CT.
*
Associated Fractures:
Displaced acetabular fractures (e.g., posterior wall fractures involving more than 40% of the wall, or unstable fragments) or femoral head fractures (Pipkin Type II, III, IV) often necessitate open reduction and internal fixation (ORIF) to restore articular congruity and stability, thereby reducing the risk of PTOA. The specific approach (e.g., Kocher-Langenbeck for posterior, iliofemoral for anterior) is dictated by the fracture pattern and dislocation direction.
4. Management of Associated Injuries:
*
Femoral Head Fractures (Pipkin):
Anatomical reduction and stable internal fixation of articular fragments (especially Pipkin Type II) are critical. Excision of small, non-weight-bearing fragments (Pipkin Type I) may be an option.
*
Acetabular Fractures:
ORIF aims for anatomical reduction and stable fixation to recreate a smooth articular surface and restore joint stability. The AO Foundation classification and surgical principles for acetabular fractures are foundational.
*
Sciatic Nerve Injury:
Most cases of post-traumatic sciatic nerve palsy are neurapraxia and resolve spontaneously. Conservative management with expectant observation is typically recommended, with neurophysiological studies used to monitor recovery. Surgical exploration is reserved for definitive evidence of nerve entrapment or complete transection, although its benefits are controversial.
5. Prophylaxis for Complications:
*
Heterotopic Ossification (HO):
The use of non-steroidal anti-inflammatory drugs (NSAIDs) such as indomethacin (post-operatively for 3-6 weeks) or a single dose of pre- or post-operative radiation therapy is highly effective in preventing HO, particularly after open reduction of hip dislocations or acetabular fractures.
*
Venous Thromboembolism (VTE):
Standard VTE prophylaxis (pharmacological with LMWH/DOACs and mechanical with SCDs) is indicated in these high-risk trauma patients.
6. Long-Term Outcomes:
* Long-term follow-up studies consistently highlight PTOA and AVN as the most common and debilitating sequelae. Even with optimal acute management, a significant percentage of patients may develop these complications, often necessitating total hip arthroplasty (THA) within 5-10 years post-injury, particularly in younger patients. The quality of initial reduction and promptness remain the most significant controllable factors influencing these long-term outcomes.
* Rehabilitation protocols emphasizing protected weight-bearing, gradual restoration of ROM, and progressive strengthening are crucial but must be individualized based on the injury's complexity and surgical intervention.
In summary, current literature and guidelines underscore the principles of urgent reduction, meticulous radiographic and CT assessment, appropriate surgical intervention for irreducible cases or associated complex fractures, comprehensive complication prophylaxis, and structured rehabilitation to optimize functional recovery and minimize long-term morbidity after traumatic hip dislocation.
You Might Also Like