Carpal Tunnel Syndrome: Comprehensive Treatment and Surgical Release
Key Takeaway
Carpal tunnel syndrome (CTS) management ranges from conservative splinting and corticosteroid injections for mild cases to surgical decompression for advanced neuropathy. Prognostic factors such as age, symptom duration, and constant paresthesia dictate nonoperative success. When conservative measures fail or thenar atrophy is present, open or limited-incision carpal tunnel release is indicated to divide the transverse carpal ligament, restoring median nerve hemodynamics and preventing irreversible motor loss.
Introduction to Carpal Tunnel Syndrome Management
The management of Carpal Tunnel Syndrome (CTS), the most prevalent compressive neuropathy of the upper extremity, requires a stratified approach based on symptom severity, duration, and the presence of motor or sensory deficits. Treatment modalities range from conservative biomechanical modifications and pharmacological interventions to surgical decompression of the median nerve. The overarching goal of any intervention is to reduce the interstitial hydrostatic pressure within the fibro-osseous carpal canal, thereby restoring microvascular perfusion to the median nerve and preventing irreversible axonal degeneration and thenar muscle atrophy.
Nonoperative Management
Conservative management is the first-line treatment for patients presenting with mild to moderate symptoms, intermittent paresthesia, and an absence of thenar muscle atrophy or profound sensory loss.
Splinting and Corticosteroid Injections
The foundation of nonoperative treatment involves nocturnal wrist splinting in a neutral position. Biomechanical studies demonstrate that carpal tunnel pressure is minimized when the wrist is at neutral (0 degrees of flexion/extension). Flexion and extension significantly elevate intracanalicular pressure, exacerbating nerve ischemia.
When splinting alone is insufficient, the injection of corticosteroid preparations into the carpal tunnel can provide substantial, albeit often temporary, relief. Corticosteroids act by reducing nonspecific synovial edema and suppressing inflammatory cascades within the flexor tenosynovium.
CLINICAL PEARL:
Long-term benefit from corticosteroid injection and splinting is achieved in only about 10% of patients. However, the response to injection is typically faster and more robust in men and in patients older than 40 years.
Care must be taken to avoid intraneural injection, which can cause catastrophic iatrogenic nerve injury. The injection should be directed ulnar to the palmaris longus tendon to safely bypass the median nerve.
Beyond its therapeutic role, a corticosteroid injection serves as a powerful diagnostic tool. In patients lacking obvious space-occupying lesions (e.g., osteophytes, ganglion cysts, or tumors), a favorable response to injection strongly confirms the diagnosis of CTS, effectively ruling out proximal compression neuropathies such as cervical radiculopathy or thoracic outlet syndrome. Some patients may elect to undergo two or three serial injections before committing to surgical intervention. If symptoms and physical findings improve without the development of muscle atrophy, continued conservative management is entirely reasonable.
Prognostic Factors in Nonoperative Treatment
Patient selection is critical for the success of conservative management. In a landmark study of 331 patients, Kaplan, Glickel, and Eaton identified five critical prognostic factors that predict the failure of nonoperative treatment:
- Age older than 50 years
- Symptom duration longer than 10 months
- Constant (rather than intermittent) paresthesia
- Coexisting stenosing flexor tenosynovitis (trigger digit)
- A positive Phalen test result in less than 30 seconds
The success of medical management is inversely proportional to the number of these factors present. When none of these factors are present, approximately two-thirds of patients are cured by conservative measures. The presence of a single factor reduces the success rate to 59.6%. Crucially, conservative treatment is almost universally ineffective in advanced cases: 93.2% of patients with three factors experience no improvement, and no patient with four or five factors is cured by medical management alone.
Diagnostic Modalities and Nerve Compression Testing
Accurate diagnosis and staging of CTS rely on a combination of provocative clinical tests and objective neurophysiological measurements.
Provocative Clinical Testing
- Phalen's Test (Wrist Flexion): Numbness or tingling in the radial digits within 60 seconds indicates probable CTS (Sensitivity 0.75, Specificity 0.47). A positive result in under 30 seconds correlates with advanced disease.
- Tinel's Sign: Percussion over the median nerve at the wrist eliciting an "electric" tingling response in the fingers (Sensitivity 0.60, Specificity 0.67).
- Durkan's Carpal Compression Test: Direct hydrostatic compression over the carpal tunnel eliciting paresthesia within 30 seconds (Sensitivity 0.87, Specificity 0.90).
Objective Sensory and Motor Evaluation
- Hand Volume Stress Test: An increase in hand volume by ≥ 10 mL after a 7-minute stress test and 10-minute rest indicates probable dynamic CTS.
- Two-Point Discrimination (Innervation Density): Failure to distinguish separation of at least 5 mm (slow-adapting fibers) or 4 mm (fast-adapting fibers) indicates advanced nerve dysfunction and axonal loss.
- Semmes-Weinstein Monofilaments: A threshold value > 2.83 for slowly adapting fibers indicates median nerve impairment (Sensitivity 0.83).
- Vibrometry: Asymmetry in the threshold of fast-adapting fibers (120 Hz) compared to the contralateral hand or the ipsilateral ulnar nerve indicates probable CTS (Sensitivity 0.87).
Electrodiagnostic Studies (EMG/NCS)
- Sensory Conduction: A latency > 3.5 ms across the wrist or an asymmetry of conduction velocity > 0.5 m/s compared to the opposite hand confirms probable CTS.
- Motor Conduction: A latency > 4.5 ms or an asymmetry > 1 m/s indicates motor fiber involvement.
- Electromyography (EMG): The presence of fibrillation potentials, positive sharp waves, or increased insertional activity in the thenar muscles signifies advanced motor median nerve compression and active denervation.
Surgical Indications and Patient Selection
Surgical division of the deep transverse carpal ligament is indicated for patients with persistent, progressive signs and symptoms that fail to respond to conservative measures.
SURGICAL WARNING:
The presence of thenar muscle atrophy or profound sensory loss (e.g., abnormal two-point discrimination) is an absolute indication for prompt surgical release to prevent irreversible axonal death.
Patients with intermediate and advanced (chronic) syndromes are best treated with early carpal tunnel release rather than prolonged, futile conservative therapy.
Special Clinical Scenarios
- Acute Carpal Tunnel Syndrome: Treatment must be individualized based on etiology. For acute CTS caused by a sudden increase in compartment pressure (e.g., following a Colles fracture treated with flexed wrist immobilization), immediate relief may be obtained simply by loosening constricting bandages and extending the wrist to a neutral position. If median nerve palsy persists despite positional changes, emergent surgical release is indicated.
- Rheumatoid Arthritis: Patients presenting with florid tenosynovitis secondary to rheumatoid arthritis or other systemic inflammatory arthropathies should undergo a formal flexor tenosynovectomy concurrently with carpal tunnel release.
- Severe Thenar Atrophy in the Elderly: In elderly patients with profound thenar wasting, weakness, and poor thumb opposition, a palmaris longus opponensplasty (Camitz procedure) performed at the time of carpal tunnel release can significantly improve functional pinch kinematics.
- Concurrent Trapeziometacarpal Osteoarthritis: Trapeziometacarpal arthroplasty and carpal tunnel release can be safely and effectively performed through two separate incisions during the same surgical setting.
Procedures Lacking Clinical Benefit
Evidence-based literature has definitively shown that extensive external neurolysis has no significant effect on outcomes. Furthermore, internal neurolysis does not improve the motor or sensory recovery following carpal tunnel release and risks iatrogenic intrafascicular scarring. Epineurotomy similarly offers no clinical benefit over simple ligamentous release and should be avoided.
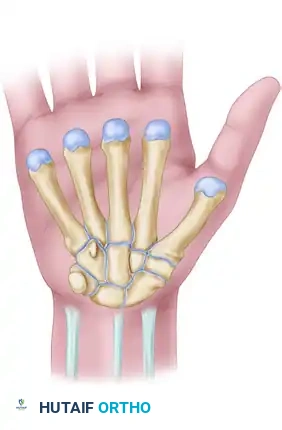
Surgical Anatomy of the Carpal Tunnel
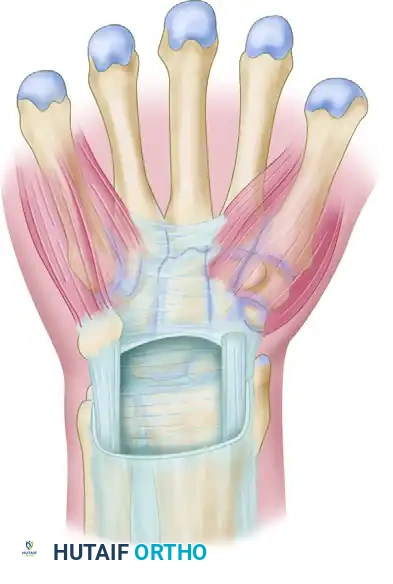
A profound understanding of the flexor retinaculum and its surrounding neurovascular structures is paramount for safe surgical execution. The classic flexor retinaculum is a complex, tripartite structure.
The proximal limit of the retinaculum aligns with the distal aspect of the pisiform, while the distal limit extends just beyond the hook of the hamate.

Anatomically, the flexor retinaculum consists of three distinct portions:
1. Proximal Portion: Deep fascia of the forearm that courses deep to the flexor carpi ulnaris and flexor carpi radialis.
2. Middle Portion (Transverse Carpal Ligament): The thick aponeurosis spanning between the thenar and hypothenar eminences. It attaches radially to the scaphoid tubercle and the trapezium ridge, and ulnarly to the pisiform and the hook of the hamate.
3. Distal Portion: An aponeurotic extension between the thenar and hypothenar musculature.
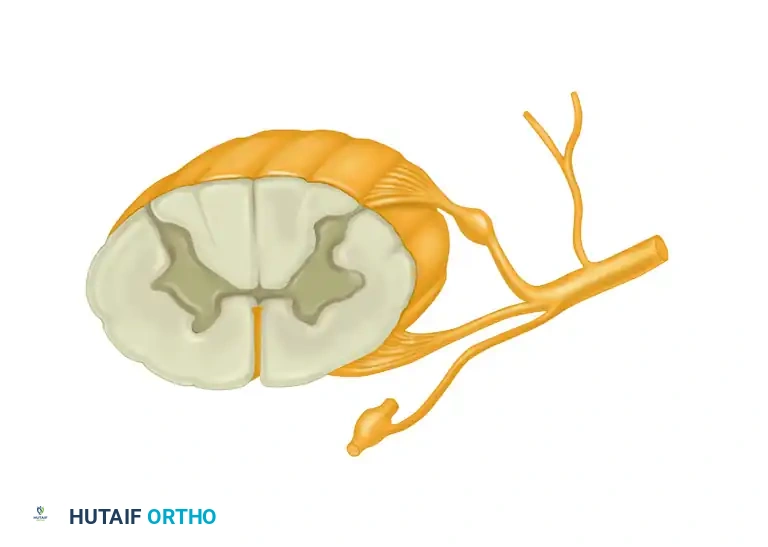
The median nerve lies superficial to the nine flexor tendons within the canal. The recurrent motor branch of the median nerve exhibits variable anatomy (extraligamentous, subligamentous, or transligamentous) and must be meticulously protected during the distal aspect of the release.
Surgical Techniques: Carpal Tunnel Release
Whether utilizing a standard open approach, a limited-incision technique, or an endoscopic method, the fundamental objective remains identical: complete division of the transverse carpal ligament under direct or endoscopic visualization.
Incision Planning and Approaches

The Standard Open Approach:
The traditional open technique provides unparalleled exposure. A longitudinal incision is made in the palm, typically starting just distal to the proximal palmar crease and extending proximally in line with the radial border of the ring finger (Kaplan's cardinal line). This axis safely parallels the median nerve while avoiding the palmar cutaneous branch, which lies more radially.
Limited and Minimal Incision Approaches:
Limited approaches, such as the "double incision" of Wilson or the "minimal incision" of Bromley, aim to reduce postoperative pillar pain and accelerate recovery, offering benefits similar to endoscopic techniques.
The use of specialized instruments like the "carpal tunnel tome" through a small palmar incision minimizes soft tissue trauma while providing adequate exposure.
Step-by-Step Surgical Execution
- Positioning and Anesthesia: The patient is positioned supine with the arm extended on a hand table. The procedure is typically performed under local anesthesia (WALANT - Wide Awake Local Anesthesia No Tourniquet) or regional block with a proximal pneumatic tourniquet.
- Incision and Superficial Dissection: The skin and subcutaneous tissues are incised. The palmar aponeurosis is identified and longitudinally divided.
- Identification of the Transverse Carpal Ligament: Blunt retractors are placed to expose the transverse fibers of the flexor retinaculum.
- Ligamentous Release: The ligament is carefully incised longitudinally, typically starting proximally and extending distally.
> PITFALL:
> Regardless of the technique selected, all structures to be incised must be clearly seen and identified. The safety of the median nerve must be visually verified before the final release of the transverse carpal ligament. Blind cutting is strictly contraindicated due to the risk of lacerating the median nerve, the recurrent motor branch, or the superficial palmar arch. - Exploration and Decompression: Once the ligament is divided, the median nerve is inspected for areas of pseudoneuroma or hourglass constriction. The canal is swept with a blunt dissector to ensure no distal fascial bands remain.
- Closure: The tourniquet is deflated, and meticulous hemostasis is achieved. Only the skin is closed; the flexor retinaculum is left open to allow for volumetric expansion of the carpal canal.
Postoperative Protocol and Outcomes
Postoperatively, a bulky soft dressing is applied to restrict wrist motion while allowing full digital flexion and extension. Early active finger mobilization is highly encouraged to prevent flexor tendon adhesions and promote nerve gliding.
Expected Prognosis
The results of surgical release are excellent in the vast majority of instances, and the benefits are highly durable.
- Timeline of Recovery: Maximal clinical improvement is typically observed within the first 6 months following carpal tunnel release. Beyond 6 months, there is generally no further statistically significant improvement in Tinel and Phalen tests, pinch strength, motor latency, symptom severity, or functional scoring.
- Resolution of Atrophy: While thenar atrophy may occasionally reverse, it resolves very slowly, and in many chronic cases, the muscle bulk never fully normalizes despite the return of functional strength.
- Age and Chronicity Factors: Surgical release might not achieve complete relief of all symptoms in patients older than 70 years or in those presenting with advanced, long-standing nerve compression. In these populations, the primary goal of surgery shifts from complete symptom resolution to the prevention of further neurological deterioration.
By adhering to strict diagnostic criteria, understanding the nuanced anatomy of the wrist, and executing a meticulous surgical decompression, orthopedic surgeons can reliably restore hand function and alleviate the debilitating symptoms of carpal tunnel syndrome.
You Might Also Like