Operative Management of Lateral Ankle Ligament Instability
Key Takeaway
Lateral ankle ligament injuries frequently result in chronic mechanical or functional instability if managed inadequately. This comprehensive surgical guide details the evidence-based operative management of both acute ruptures and chronic instability. It covers anatomical repairs, such as the Broström procedure, and non-anatomical tenodesis reconstructions, including the Chrisman-Snook and Sammarco modifications. Step-by-step surgical techniques, biomechanical principles, and postoperative rehabilitation protocols are provided to optimize patient outcomes and restore tibiotalar and subtalar joint kinematics.
INTRODUCTION TO LATERAL ANKLE INSTABILITY
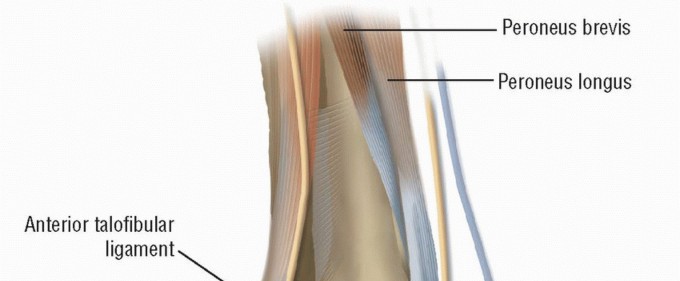
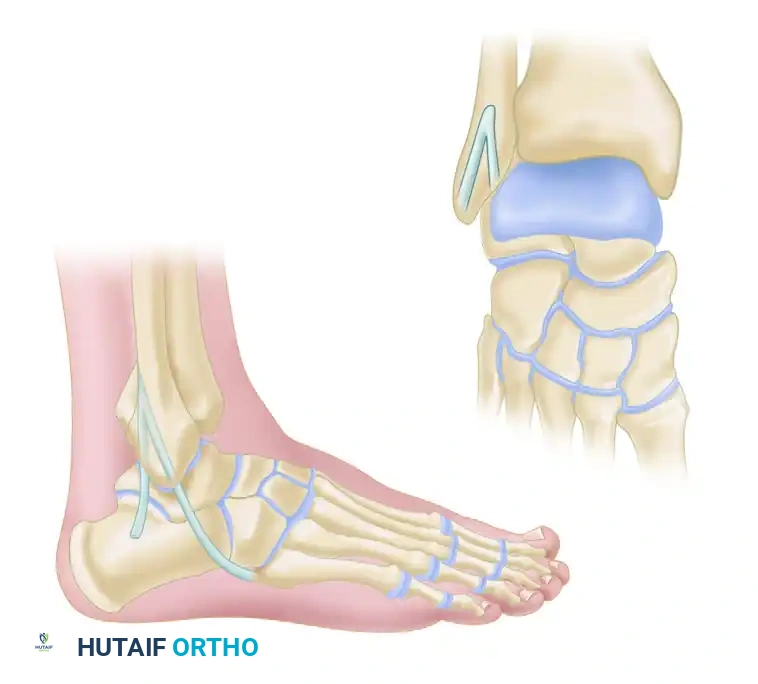
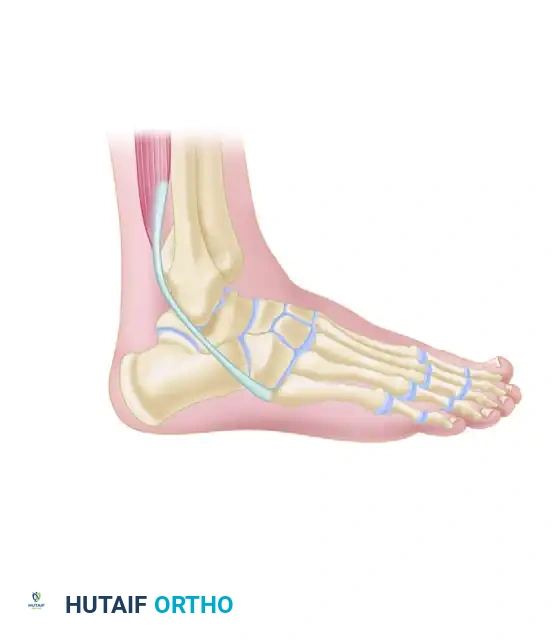
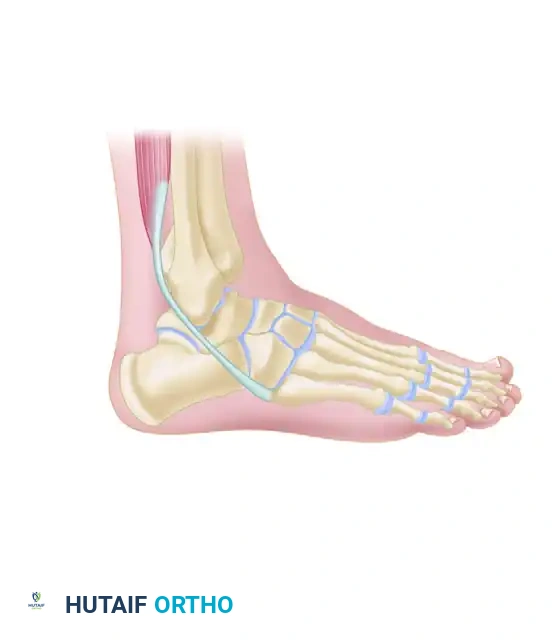
Lateral ankle sprains are among the most ubiquitous injuries encountered in orthopedic practice. While the majority of these injuries resolve with structured functional rehabilitation, a significant subset of patients will develop chronic mechanical or functional instability. The lateral ligamentous complex of the ankle consists of the anterior talofibular ligament (ATFL), the calcaneofibular ligament (CFL), and the posterior talofibular ligament (PTFL). The ATFL is the primary restraint to inversion in plantar flexion, while the CFL restrains inversion in neutral and dorsiflexion, crossing both the tibiotalar and subtalar joints.
Surgical intervention is indicated when conservative measures fail, and patients experience recurrent giving-way, persistent pain, or objective mechanical laxity. The surgical management of lateral ankle instability is broadly categorized into the direct anatomical repair of acute or chronic ruptures (e.g., the Broström procedure and its modifications) and non-anatomical tenodesis reconstructions utilizing autograft or allograft tissue.
REPAIR OF ACUTE RUPTURE OF LATERAL LIGAMENTS
Direct anatomical repair of acute lateral ligament ruptures is typically reserved for high-demand athletes, patients with severe multi-ligamentous trauma, or those with massive avulsion injuries where conservative management is deemed insufficient to restore native joint kinematics. The classic direct repair techniques, pioneered by Staples, Black, and Broström, focus on restoring the native anatomy without sacrificing dynamic stabilizers like the peroneal tendons.
Surgical Anatomy and Preoperative Considerations
Before proceeding with an acute repair, the surgeon must carefully evaluate the soft tissue envelope. Severe edema and fracture blisters must resolve to minimize the risk of wound dehiscence and deep infection.
🔪 Surgical Warning: The lateral surgical approach places two critical sensory nerves at risk: the superficial peroneal nerve (SPN) anteriorly and the sural nerve posteriorly. Meticulous blunt dissection and the preservation of superficial veins are mandatory to prevent painful postoperative neuromas and venous stasis.
Surgical Technique (Staples, Black; Broström)
The goal of the acute repair is the direct end-to-end approximation of the torn ligaments or their reattachment to bone.
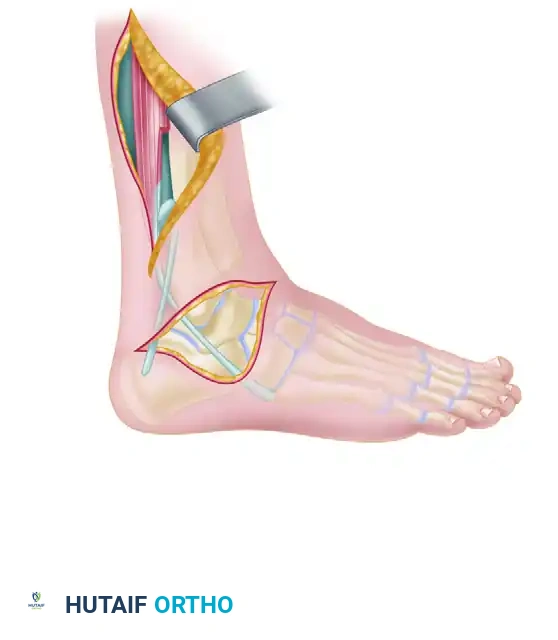
- Incision and Exposure:
Begin a curved incision 5 cm proximal to the distal tip of the fibula and 1.5 cm anterior to its margin. Curve the incision distally and posteriorly, ending distal to the fibula at a point half the distance from the tip of the fibula to the tip of the heel. - Nerve and Vein Preservation:
Carefully identify and retract the branches of the superficial peroneal nerve anteriorly and the sural nerve distally. Preserve as many superficial veins as possible to avoid postoperative venous stasis, skin edge necrosis, and delayed wound healing. - Deep Dissection:
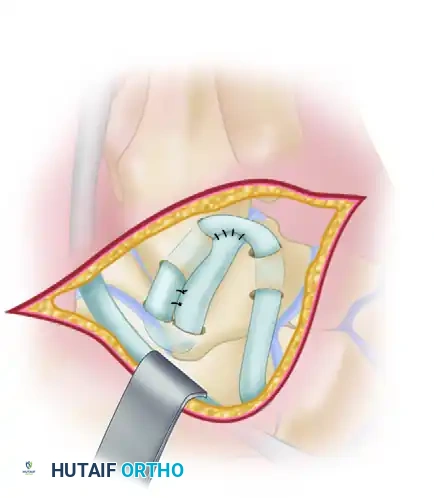
Section the aponeurotic tissue overlying the tibiofibular joint and the ankle joint capsule. Expose the areas of capsular and ligamentous tearing via blunt dissection. Incise the peroneal sheath and gently retract the peroneal tendons posteriorly to expose the calcaneofibular ligament (CFL) and the anterior portion of the posterior talofibular ligament (PTFL).




- Stress Testing and Assessment:
With the ligaments exposed, manually stress the lateral ligaments to assess stability at both the ankle and subtalar joints by forcibly inverting the foot. - Ligamentous Repair:
Using appropriate nonabsorbable suture material (e.g., 0 or 2-0 braided polyester or ultra-high-molecular-weight polyethylene), approximate the torn ends of the ligaments. If the ligaments are avulsed directly from the bone (fibula, talus, or calcaneus), suture the ends to adjacent robust aponeurotic tissue or secure them through small drill holes (or suture anchors) placed into the anatomical footprint on the bone. - Subtalar Stabilization:
If the talocalcaneal ligament is torn and subtalar instability is present, stabilize the subtalar joint by suturing the calcaneofibular ligament. If the native tissue is attenuated, reinforce the repair with a local flap of adjacent aponeurotic tissue (extensor retinaculum). - Closure:
Repair the joint capsule and the peroneal sheath anatomically. Close the subcutaneous tissue and skin. Apply a well-padded plaster posterior splint with a U-shaped stirrup. The ankle must be immobilized in a neutral position in the sagittal plane and mildly everted to remove tension from the lateral repair.
Postoperative Care and Rehabilitation
Strict adherence to the postoperative protocol is vital to prevent stretching of the repaired tissues while avoiding debilitating arthrofibrosis.
- Immediate Post-Op: Sitting is allowed with the leg dependent for 30 to 60 seconds each half hour. Once dependency is tolerated without throbbing pain, crutch walking (non-weight-bearing) is instituted.
- 2 Weeks: The initial surgical splint is removed, sutures are extracted, and the limb is transitioned to a short-leg cast.
- 4 Weeks: The cast is removed. Weight-bearing in a controlled walking boot with crutches is initiated. Dorsiflexion and plantar flexion exercises are prescribed as soon as practical to nourish the articular cartilage and align collagen fibers.
- 6 Weeks: The patient progresses to full weight-bearing without crutches. Range-of-motion exercises and manual resistive exercises to gain peroneal eversion strength are aggressively pursued.
- 8 Weeks: Inversion past neutral is strictly prohibited until 8 weeks post-surgery to protect the healing ATFL and CFL.
CHRONIC INSTABILITY AFTER INJURY
Chronic instability of the ankle following an earlier ligamentous rupture presents as either mechanical instability (objective laxity on stress testing) or functional instability (the subjective feeling of the ankle giving way due to neuromuscular or proprioceptive deficits).
Clinical Evaluation and Diagnostics
When disabling pain and instability persist despite conservative measures, a thorough diagnostic workup is required.
- Stress Radiography: Mechanical instability is confirmed when stress radiographs demonstrate 8 to 10 degrees of increased talar tilt in the ankle mortise compared with the contralateral normal ankle.
- Advanced Imaging: If stress radiographs are negative but pain persists, other etiologies such as stress fractures, osteochondral lesions of the talus (OCDs), or peroneal tendinopathy must be ruled out.


Clinical Note: Dixon et al. described a symptomatic anterolateral exostosis (an excrescent lesion) at the insertion of the ATFL, identifiable via CT scan in patients with chronic ankle pain following inversion injuries. Surgical excision combined with a Broström repair is often curative.
💡 Clinical Pearl: The Role of Arthroscopy
Arthroscopic examination at the time of ligament reconstruction is highly recommended by many surgeons to identify and treat concomitant intra-articular pathology (e.g., chondral lesions, synovitis, loose bodies). However, some authors argue that if advanced imaging (MRI) is negative for intra-articular pathology, arthroscopy may be unnecessary and can complicate the open procedure by causing fluid extravasation into the lateral soft tissues, obscuring surgical planes.
Conservative Management
Symptomatic chronic instability should initially be managed conservatively.
* Footwear Modifications: Symptoms in women may be decreased by broadening and lowering the heel of the shoe. In men, applying a lateral flare or wedge to the shoe heel can resist inversion moments.
* Bracing and Orthoses: A laced leather or polychloroprene (Neoprene) ankle corset or a rigid stirrup brace provides excellent proprioceptive feedback and mechanical support during strenuous activity. Greene et al. demonstrated that semi-rigid orthoses are more effective than traditional taping in providing initial ankle protection and preventing reinjury, yielding higher satisfaction rates among athletes.
* Taping: Larsen’s evaluation of taped versus untaped ankles in chronic instability patients revealed that taping significantly decreased measurable instability initially. However, after 20 minutes of exercise, the adhesive bandages loosened, providing only limited protection, though talar tilt remained somewhat controlled.
SURGICAL RECONSTRUCTION FOR CHRONIC INSTABILITY
When a minimum of 3 to 6 months of aggressive muscle-strengthening and proprioceptive rehabilitation fails, surgical reconstruction is indicated. Procedures are divided into anatomical shortening/imbrication repairs and non-anatomical tenodesis reconstructions.
Anatomical Shortening and Imbrication Procedures
Reconstruction of chronically lax lateral ligaments by shortening procedures attacks the basic anatomical defect without sacrificing the dynamic stability of the peroneal tendons.
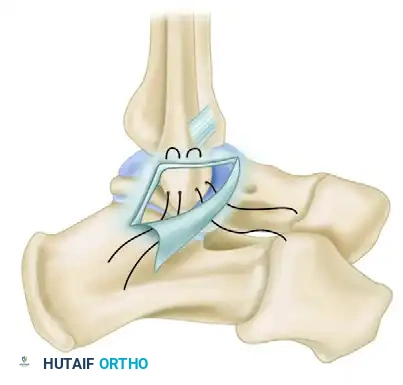
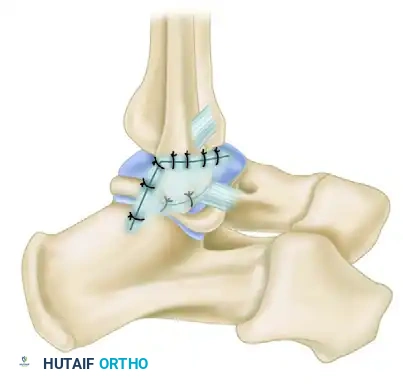
The Broström and Karlsson Techniques:
A simple reconstructive procedure, originally described by Broström, involves subperiosteal release of the distal lateral malleolus. The released flap, containing the attenuated insertions of the ATFL and CFL, is advanced and reattached to the malleolus more proximally.
Karlsson et al. modified this by transecting the lateral ligaments, imbricating the ATFL, and frequently the CFL, and securing them through osseous drill holes. This restores mechanical stability in over 80% of patients.
🚨 Surgical Pitfall: Anatomical imbrication procedures have a higher failure rate in patients with generalized joint hypermobility (e.g., Ehlers-Danlos syndrome), long-standing severe ligamentous laxity, or prior failed ankle surgeries. In these populations, a non-anatomical tenodesis or allograft reconstruction is preferred.




Non-Anatomical Tenodesis Reconstructions
When native tissue is insufficient for anatomical repair, tenodesis procedures utilizing the peroneus brevis tendon are employed. Historically, the Watson-Jones, Evans, and Elmslie operations were the gold standards.
- Watson-Jones Procedure: Attempts to reconstruct both the ATFL and CFL. However, it presents technical difficulties, including challenging drill angles in the talar neck and insufficient peroneus brevis tendon length. Furthermore, Chrisman and Snook demonstrated experimentally that subtalar instability often persists because the line of pull of the routed tendon is at a right angle to the native CFL fibers.
- Evans Procedure: Designed to overcome the technical difficulties of the Watson-Jones technique, the Evans procedure reconstructs only the CFL. While it controls talar tilt effectively, it is less effective at controlling anteroposterior translation (anterior drawer). Kaikkonen and Rosenbaum noted that the Evans procedure permanently alters ankle joint kinematics, potentially contributing to long-term arthrosis. It is now generally reserved as a salvage procedure when anatomical reconstruction is impossible.
The Elmslie Procedure
The Elmslie procedure utilizes a strip of fascia or tendon routed through the fibula, talus, and calcaneus to recreate the lateral complex.


The Chrisman-Snook Modification
To address the persistent subtalar instability seen in the Watson-Jones procedure, Snook, Chrisman, and Wilson modified the Elmslie procedure. This technique uses a split half of the peroneus brevis tendon to reconstruct both the ATFL and CFL, restoring a more anatomical line of pull.
Key Modifications (1985 Update):
1. Calcaneal Tunnel: A direct tunnel is drilled in the calcaneus, which is biomechanically stronger and technically easier to create than the original "trapdoor" technique.
2. Graft Fixation: The end of the graft is sutured in front of the lateral malleolus rather than at the base of the fifth metatarsal, providing a significantly stronger repair.
3. Positioning: The foot and ankle are held in mild rather than forced eversion while the graft is tensioned and sutured.
Biomechanical cadaveric studies confirm that the Chrisman-Snook reconstruction provides superior stability to the ankle joint complex compared to the Evans and Watson-Jones procedures, though it does result in a slight, permanent reduction in physiologic inversion motion.


The Larsen Technique
Larsen described a transfer of the distal part of the peroneus brevis tendon to address chronic instability. The tendon is detached proximally, pulled through two converging canals bored into the lateral malleolus, and fixed into a blind hole in the calcaneus. The specific routing direction of the tendon in relation to the calcaneus and talus can be customized based on the predominant plane of instability.
The Sammarco and DiRaimondo Modification
For high-demand athletes, patients with long-standing combined ankle and subtalar instability, or those undergoing revision for a failed primary reconstruction, Sammarco and DiRaimondo developed a robust modification of the Elmslie technique.
Surgical Steps:
1. Graft Harvest: A split peroneus brevis tendon graft is harvested proximally from the musculotendinous junction and pulled beneath the skin into the distal incision.
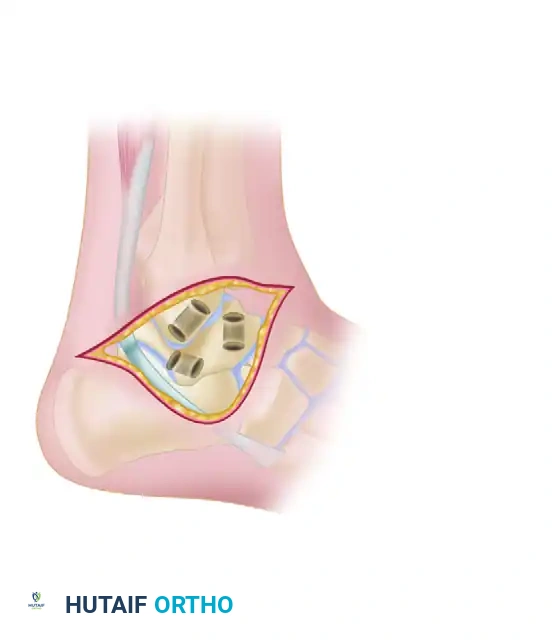
2. Osseous Tunnels: Drill holes are placed in the talar neck, the lateral malleolus, and the calcaneus. These tunnels are connected beneath 1.0- to 1.5-cm bony bridges to prevent cortical blowout.
3. Graft Routing and Reinforcement: The split tendon graft is passed through the bony tunnels,
Associated Surgical & Radiographic Imaging
📚 Medical References
- lateral ankle instability, Clin Orthop Relat Res 422:180, 2004.
- Baltzer AW, Arnold JP: Bone-cartilage transplantation from the ipsilateral knee for chondral lesions of the talus, Arthroscopy 21:159, 2005.
- [
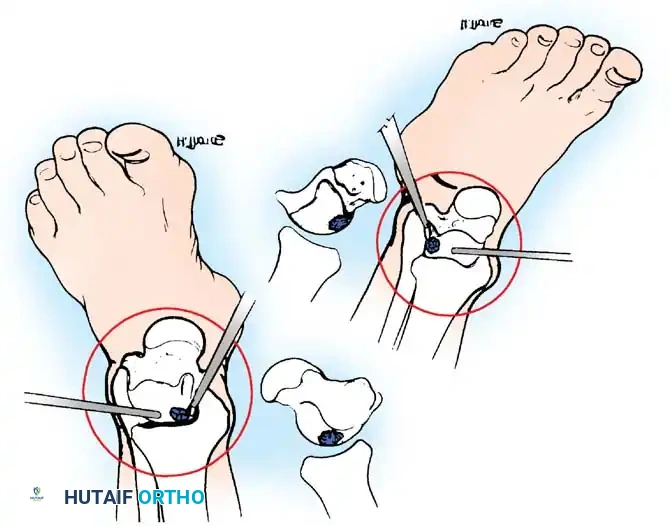
A
B
Fig. 42-48 Anterolateral (A) and anteromedial (B) portals for arthroscopic excision of osteochondritis dissecans of ankle. (Redrawn from Parisien JS: Diagnostic and surgical arthroscopy of the ankle: technique and indications, Bull Hosp Jt Dis 45:38, 1985.)

You Might Also Like