Advanced Surgical Management of Lesser Toe Deformities: The Weil Osteotomy and Mallet Toe Correction
Key Takeaway
The Weil osteotomy is a highly effective shortening procedure for the lesser metatarsals, primarily indicated for central metatarsalgia, metatarsophalangeal joint subluxation, and crossover toe deformities. By creating a precise osteotomy parallel to the weight-bearing surface, surgeons achieve controlled metatarsal shortening while minimizing plantar pressure. Concurrently, distal interphalangeal joint pathologies, such as mallet toe, require targeted interventions ranging from percutaneous flexor tenotomies to terminal Syme amputations, depending on deformity rigidity and patient comorbidities.
INTRODUCTION TO LESSER RAY PATHOLOGY
The surgical management of lesser toe deformities requires a profound understanding of forefoot biomechanics, the metatarsal parabola, and the delicate balance between the intrinsic and extrinsic musculature of the foot. Pathologies of the lesser rays frequently present as a continuum of deformity, ranging from isolated distal interphalangeal (DIP) joint contractures (mallet toe) to complex, multi-planar metatarsophalangeal (MTP) joint dislocations with associated central metatarsalgia.
This comprehensive guide details the operative principles and step-by-step techniques for two critical procedures in the orthopaedic foot and ankle armamentarium: the Shortening Metatarsal (Weil) Osteotomy for MTP joint pathology, and the targeted surgical correction of Mallet Toe deformities.
PART I: THE SHORTENING METATARSAL (WEIL) OSTEOTOMY
The Weil osteotomy, popularized by L.S. Weil, is an intra-articular, extra-capsular shortening osteotomy of the distal metatarsal. It is the gold standard for addressing central metatarsalgia associated with a relatively long lesser metatarsal, plantar plate insufficiency, and dorsal subluxation or dislocation of the MTP joint.
Biomechanical Principles and Preoperative Planning
The primary goal of the Weil osteotomy is to decompress the MTP joint and restore the normal metatarsal cascade (the Maestro curve). By shortening the metatarsal, tension on the extrinsic tendons and the contracted plantar plate is relieved, allowing for spontaneous or surgically assisted reduction of the MTP joint.
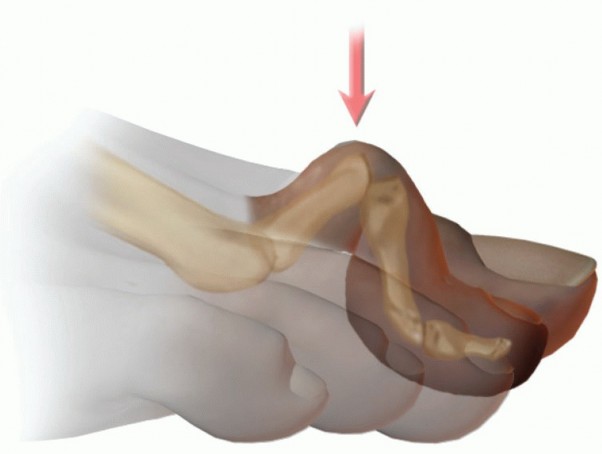
Surgical Pearl: The Plane of the Osteotomy
The most critical biomechanical aspect of the Weil osteotomy is the angle of the saw cut. The osteotomy must be made parallel to the weight-bearing surface (the ground), not parallel to the metatarsal shaft. If the cut is made parallel to the shaft, proximal translation of the capital fragment will result in plantar depression of the metatarsal head, paradoxically worsening the patient's metatarsalgia.
Preoperative weight-bearing dorsoplantar and lateral radiographs are mandatory. The required amount of shortening (typically ranging from 3 to 8 mm) is templated by comparing the length of the involved metatarsal to the adjacent metatarsals, factoring in the severity of the MTP joint dislocation. The objective is to equalize the functional lengths of the lesser metatarsals to ensure an even distribution of forefoot plantar pressures.
Step-by-Step Surgical Technique
1. Incision and Exposure
* Make a 3-cm dorsal longitudinal incision centered over the affected MTP joint. If multiple adjacent metatarsals are being addressed, a single incision placed in the intermetatarsal space (e.g., between the 2nd and 3rd metatarsals) can provide access to both rays while minimizing soft tissue stripping.
* Carefully retract the dorsal cutaneous nerves.
* Identify the extensor digitorum longus (EDL) and extensor digitorum brevis (EDB) tendons. Retract them laterally or perform a Z-lengthening if severe contracture is present.
2. Capsulotomy and Joint Preparation
* Incise the dorsal joint capsule longitudinally to expose the metatarsal head and neck.
* Perform a thorough release of the contracted dorsal structures. Dissect the collateral ligaments of the MTP joint off their insertions at the base of the proximal phalanx.
* Partly reduce the MTP joint dislocation and maximally plantarflex the toe. This maneuver delivers the metatarsal head dorsally, providing optimal exposure for the saw blade.
3. Executing the Osteotomy
* Utilize a small sagittal saw with a fine-toothed blade.
* Initiate the cut at the dorsal-most portion of the articular cartilage of the metatarsal head.
* Direct the saw blade proximally, ensuring the plane of the osteotomy is strictly parallel to the ground (the plantar aspect of the foot).
* The Double-Cut Technique: For deformities requiring significant shortening (>3-4 mm), a single cut with proximal translation can cause the plantar fragment to shift excessively plantarward due to the thickness of the metatarsal neck. To prevent this, before completing the first cut, create a second cut parallel to the first. Remove a parallel-sided slice of bone 2 to 3 mm thick. This allows for substantial shortening without altering the plantar elevation of the metatarsal head.
4. Translation and Fixation
* Shift the plantar capital fragment proximally to achieve the preoperatively templated shortening (3 to 8 mm).
* Temporarily secure the osteotomy with a smooth 0.045-inch Kirschner wire.
* Evaluate the metatarsal parabola and joint reduction clinically and with intraoperative fluoroscopy.
* Secure the osteotomy definitively using a single screw from a mini-fragment AO/ASIF set (typically a 1.5 mm or 2.0 mm cortical screw, or a specialized twist-off Weil screw).
* Direct the screw from dorsal-proximal to plantar-distal. Crucial: Measure the screw length precisely to avoid plantar prominence, which can irritate the flexor tendons or sesamoids. Countersink the screw head to prevent dorsal soft tissue irritation.
5. Resection of the Dorsal Prominence
* Following proximal translation, a sharp dorsal protuberance of the proximal metatarsal shaft will overhang the capital fragment.
* Use a rongeur or the sagittal saw to resect this dorsal overhang flush with the metatarsal head. Failure to remove this bone will result in dorsal impingement and restricted MTP joint dorsiflexion.
6. Adjunctive Pinning (Optional)
* If the MTP joint remains unstable or if concurrent proximal interphalangeal (PIP) joint arthrodesis was performed, consider advancing a Kirschner wire across the MTP joint into the metatarsal shaft.
* Surgical Warning: The transfixing wire must be 0.062-inch or greater. Using a smaller wire (e.g., 0.045-inch) to transfix the MTP joint carries a high risk of pin breakage due to the sheer forces across the joint. Perform this step under fluoroscopic guidance.
Postoperative Care for Weil Osteotomy
If fixation is secure and bone quality is adequate, a lightly compressive forefoot dressing is applied. The patient is generally allowed to bear weight as tolerated on the heel and lateral border of the foot in a rigid, postoperative stiff-soled shoe.
Bandages are typically replaced at 2 weeks postoperatively and are maintained for a total of 4 weeks to hold the toe in a slightly plantarflexed position (mitigating the risk of a "floating toe"). If radiographs at 4 to 6 weeks demonstrate satisfactory primary bone healing, the patient may transition to a supportive, stiff-soled athletic shoe.
Complication Management: The "Floating Toe"
The most common complication of the Weil osteotomy is the "floating toe" (elevation of the toe off the ground during weight-bearing). This occurs because shortening the metatarsal alters the axis of the lumbrical muscles, shifting them dorsal to the center of rotation of the MTP joint, converting them from plantarflexors to dorsiflexors. Meticulous plantarflexion taping postoperatively and concurrent flexor tendon transfers (e.g., Girdlestone-Taylor procedure) can help mitigate this risk.
PART II: MALLET TOE DEFORMITY
While MTP joint pathology often dictates metatarsal interventions, isolated deformities of the distal interphalangeal (DIP) joint require a different anatomical approach. A mallet toe is characterized by an isolated flexion deformity at the DIP joint, with normal alignment at the PIP and MTP joints.
Pathoanatomy and Clinical Evaluation
The exact etiology of a mallet toe is multifactorial, but it occurs most frequently in the second toe. The second toe is often the longest digit in the human foot (Morton's toe). When confined within a shoe featuring a narrow or short toe box, the projection of the second toe distal to the others causes repetitive axial pressure at the tip of the toe, leading to buckling at the DIP joint.
Over time, this chronic flexion posture attenuates the terminal extensor tendon until it loses its mechanical advantage and can no longer extend the distal phalanx. In the absence of a strong extensor antagonist, the flexor digitorum longus (FDL) holds the DIP joint in continuous flexion until the soft tissues contract and the deformity becomes rigidly fixed.

Clinical Presentation:
In feet with normal sensibility, the hallmark complication of a mallet toe is a painful, hyperkeratotic "end corn" located just beneath the nail bed or at the distal tip of the toe. This results from chronic, unyielding pressure as the tip of the toe is habitually driven into the sole of the shoe during the toe-off phase of gait.
Diabetic Considerations:
Mallet toes are highly prevalent in diabetic patients with peripheral neuropathy. The exact biomechanical trigger in this population is debated, but intrinsic muscle wasting (intrinsic minus foot) plays a significant role. Because these patients lack protective sensation, the terminal end corn can rapidly ulcerate, progressing to deep soft tissue infection and distal phalangeal osteomyelitis before the patient is even aware of the lesion.
Note: Congenital mallet toes, much like congenital hammer toes, are generally asymptomatic and rarely require surgical intervention.
Conservative Management
Conservative treatment for mallet toe is notoriously difficult and generally unrewarding once the deformity becomes fixed.
* Footwear Modifications: Extra-depth shoes with wide, high toe boxes are the first line of defense.
* Orthotics: The use of a silicone toe crest pad can help relieve pressure at the tip of the toes by elevating the distal phalanx and transferring weight-bearing forces to the plantar aspect of the middle phalanx.
* Splinting: Taping and splinting are generally ineffective for rigid deformities.
Surgical Treatment Strategies
When conservative measures fail and symptoms warrant surgical intervention, the approach is dictated by the rigidity of the deformity and the patient's functional demands. Transfer of the deforming FDL to the extensor mechanism (to correct a flexion deformity this far distal) is technically demanding and yields unpredictable results; therefore, it is generally not recommended over simpler, more dependable procedures.
1. Percutaneous Flexor Tenotomy
In elderly patients, diabetic patients, or those with a flexible deformity, a simple flexor tenotomy at the DIP flexion crease is often sufficient to relieve symptoms.
* Technique: This can be performed percutaneously in the office setting under local anesthesia. A #11 blade is inserted in the midline of the plantar DIP flexion crease to transect the FDL tendon.
* The tenotomy is combined with manual, forceful dorsiflexion to rupture any residual fixed flexion contractures of the volar plate.
* Postoperative Care: A compression forefoot dressing is applied. The foot is elevated for 5 minutes (patient supine, foot resting on the flexed opposite knee) to achieve hemostasis. One or two simple sutures may be used if the incision was widened. A wooden-soled postoperative shoe is worn until sutures are removed at 2 weeks.
2. Middle Phalanx Resection and Dorsal Dermodesis
If the mallet deformity is of long duration and rigidly fixed in severe flexion, soft tissue release alone will fail. Bony resection is required to decompress the joint.
* Technique: An elliptical dorsal incision is made over the DIP joint, excising the redundant skin (dermodesis).
* The terminal extensor tendon is transected, and the collateral ligaments are released.
* A subtotal or total resection of the head and neck of the middle phalanx is performed using a rongeur or bone-cutting forceps.
* If the toe does not sit in a corrected, neutral position after bony resection, an FDL tenotomy is added.
* The wound is closed by suturing the proximal and distal skin edges together, which acts as a dorsal dermodesis to hold the toe in extension while fibrous ankylosis occurs.
3. Terminal Syme Amputation
For severe, recalcitrant fixed flexion contractures at the DIP joint—particularly in diabetic patients with chronic, non-healing distal ulcerations or osteomyelitis of the distal phalanx—a terminal Syme amputation is highly effective.
* Technique: This involves the amputation of the distal half of the distal phalanx, including the complete excision of the nail plate and the germinal matrix. The plantar flap is then advanced dorsally to cover the defect, providing a durable, weight-bearing soft tissue envelope at the tip of the toe.
PART III: AMPUTATION FOR SEVERE DEFORMITY
In specific clinical scenarios, joint-preserving osteotomies and arthroplasties may be contraindicated. For severe, rigid hammer toe or crossover toe deformities in low-demand, elderly patients, complete removal of the second toe at the MTP joint is a viable and highly successful salvage procedure.
Historically, surgeons hesitated to amputate the second toe due to the theoretical risk of accelerating hallux valgus deformity (as the second toe acts as a lateral buttress for the hallux). However, contemporary literature challenges the severity of this risk in the elderly population.
Evidence-Based Outcomes:
Gallentine and DeOrio evaluated the amputation of the second toe at the MTP joint in a cohort of 17 toes across 12 low-demand elderly patients. The results demonstrated high patient satisfaction (10 patients fully satisfied, 2 satisfied with reservations). Notably, even when associated hallux valgus was present and left surgically uncorrected, progression of the bunion deformity did not appear to be a clinically significant problem at an average follow-up of 33 months.
Amputation provides immediate pain relief, eliminates the risk of recurrent contracture, and allows for rapid mobilization in patients whose primary goal is comfortable ambulation in standard or extra-depth footwear.
📚 Medical References
- Weil osteotomy of the lesser metatarsals: a clinical and pedobarographic follow-up study, Foot Ankle Int 21:370, 2000.
- Weil LS: Weil head-neck oblique osteotomy: technique and fi xation. Presented at Techniques of Osteotomies on the Forefoot, Bordeaux, France, Oct 20-22, 1994.
- Zingas C, Katcherian DA, Wu KK: Kirschner wire breakage after surgery of the lesser toes, Foot Ankle Int 16:504, 1995.
- Mallet Toe Coughlin MJ: Operative repair of mallet toe deformity, Foot Ankle Int 16:109, 1995.
- Murphy GA: Mallet toe deformity, Foot Ankle Clin 3:279, 1998.
- Corns and Calluses Claeys R: The analysis of ground reaction forces in pathological gait secondary to disorders of the foot, Int Orthop 7:113, 1983.
- Coughlin MJ, Kennedy MP: Operative repair of fourth and fi fth toe corns, Foot Ankle Int 24:147, 2003.
- Giannestras N: Shortening of the metatarsal shaft in the treatment of plantar keratosis: an end-result study, J Bone Joint Surg 40A:61, 1958.
- Helal B, Greiss M: Telescoping osteotomy for pressure metatarsalgia, J Bone Joint Surg 66B:213, 1984.
- Idusuyi OB, Kitaoka HB, Patzer GL: Oblique
You Might Also Like