Surgical Correction of Great and Second Toe Clawing
Key Takeaway
Clawing of the great and second toes frequently results from neuromuscular imbalance or intrinsic minus foot conditions. Surgical correction requires a systematic approach, addressing both soft tissue contractures and osseous deformities. This guide details the step-by-step operative technique, including extensor tendon lengthening, metatarsophalangeal joint capsulotomy, and interphalangeal joint arthrodesis or arthroplasty, ensuring optimal biomechanical restoration and functional outcomes for the patient.
PATHOMECHANICS AND CLINICAL EVALUATION OF CLAW TOE DEFORMITY
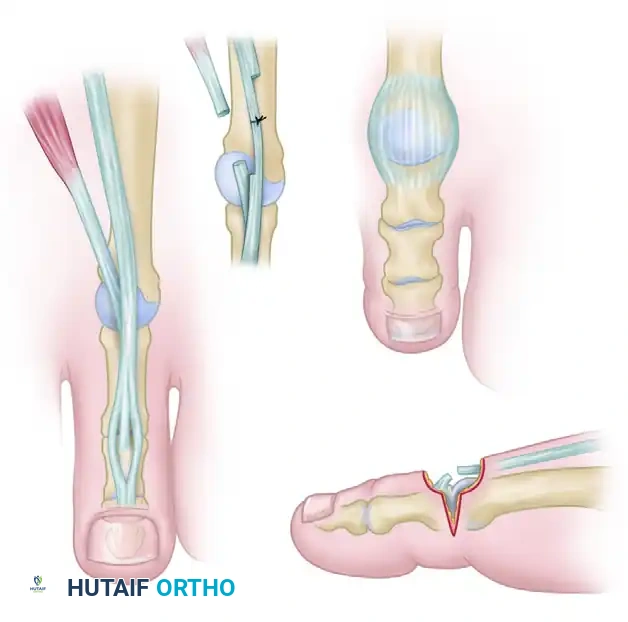
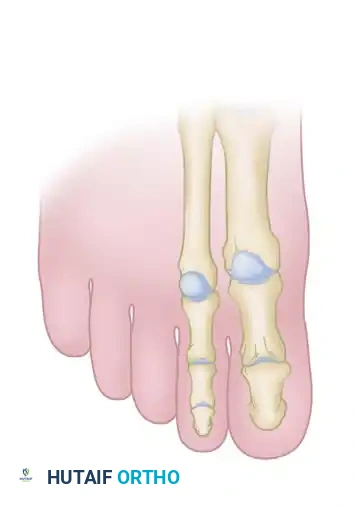
Clawing of the great and lesser toes is a complex multi-planar deformity characterized by hyperextension at the metatarsophalangeal (MTP) joint and flexion at the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints. In the hallux, the deformity manifests as MTP hyperextension and interphalangeal (IP) joint flexion. This condition is frequently encountered in the setting of neuromuscular disorders (such as Charcot-Marie-Tooth disease), intrinsic minus foot conditions, rheumatoid arthritis, or as a sequela of compartment syndrome and isolated plantar fascia release.
The primary pathoanatomy involves an imbalance between the strong extrinsic extensors (Extensor Hallucis Longus [EHL], Extensor Digitorum Longus [EDL]) and the weakened or overpowered intrinsic musculature (lumbricals and interossei). When the intrinsic muscles fail to flex the MTP joints, the extrinsic extensors draw the proximal phalanx into rigid dorsiflexion. Consequently, the extrinsic flexors (Flexor Hallucis Longus [FHL], Flexor Digitorum Longus [FDL]) exert an unopposed flexion force on the interphalangeal joints, exacerbating the clawed posture.
Preoperative Assessment
A meticulous clinical examination is paramount to differentiate between flexible and rigid deformities, as this dictates the surgical algorithm.
Clinical Pearl: Utilize the Kelikian push-up test. Apply pressure to the plantar aspect of the metatarsal heads. If the toes reduce to a neutral alignment, the deformity is flexible, and soft-tissue procedures (tendon lengthening, capsulotomy) may suffice. If the deformity persists, it is rigid, necessitating osseous intervention (phalangeal resection or arthrodesis).
SURGICAL INDICATIONS AND PREOPERATIVE PLANNING
Surgical intervention is indicated for patients with painful, rigid claw toe deformities that have failed conservative management (e.g., deep toe-box footwear, crest pads, custom orthoses), particularly when complicated by dorsal ulcerations over the PIP joints or plantar keratoses beneath the metatarsal heads.
Goals of Surgery:
* Restore a plantigrade, functional foot.
* Relieve pressure over bony prominences.
* Re-establish the windlass mechanism and normal forefoot kinematics.
* Prevent recurrence through meticulous tendon balancing.
Anesthesia and Positioning:
The procedure is typically performed under general anesthesia or regional anesthesia (popliteal block with a saphenous nerve block). The patient is positioned supine on the operating table. A bump may be placed under the ipsilateral hip to internally rotate the leg to a neutral position. A thigh or calf tourniquet is applied to ensure a bloodless surgical field.
OPERATIVE TECHNIQUE: STEP-BY-STEP GUIDE
1. Incision and Deep Exposure
The approach begins with a carefully planned longitudinal incision to access the extensor mechanisms of both the great and second toes simultaneously.
- Make a longitudinal incision in the first intermetatarsal space. The incision should extend from just proximal to the first web space, coursing proximally to the midshaft level of the respective first and second metatarsals.
- Carefully dissect through the subcutaneous tissues.
Surgical Warning: The terminal branch of the deep peroneal nerve and the accompanying first dorsal intermetatarsal artery occupy a plane slightly deeper than the extensor tendons. Meticulous blunt dissection and minimal undermining of the skin edges are critical to prevent iatrogenic neurovascular injury, which could lead to painful neuromas or compromised flap viability.
- By minimally undermining each side of the incision, expose the Extensor Hallucis Longus (EHL), Extensor Hallucis Brevis (EHB), Extensor Digitorum Longus (EDL), and Extensor Digitorum Brevis (EDB) tendons.
2. Tendon Lengthening and Resection
Correction of the hyperextension deformity at the MTP joint begins with addressing the contracted extrinsic and intrinsic extensor tendons.
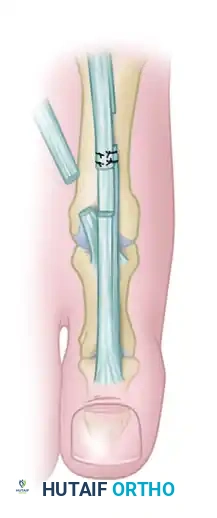
- EHL Lengthening: Perform a Z-plasty lengthening of the EHL tendon. A 3-cm coronal Z-plasty is preferred over a sagittal cut, as the coronal plane allows for a smoother gliding surface post-repair and minimizes subcutaneous bulk.
- EHB and EDB Resection: Identify the EHB and EDB tendons, which lie immediately lateral and deep to the EHL and EDL as they approach the MTP joints. Excise a 5- to 8-mm section of both the EHB and EDB. Simple tenotomy is insufficient; a tenectomy prevents spontaneous reconstitution and recurrent contracture.
Clinical Pearl: Do not repair the EHL tendon at this stage. Keep in mind that overlapping the tendons during the final repair is much easier than discovering you have insufficient length when the MTP joint is later pinned or held in a neutral position.
3. Metatarsophalangeal Joint Capsulotomy
Assess the resting posture of the toes. The correction of the extension posture by tendon lengthening alone can sometimes be remarkable. However, if the deformity is not fully corrected to a neutral position at the MTP joint, a dorsal capsulotomy is required.
- With the EHL and EDL tendons retracted beneath the skin edges, sharply incise the dorsal capsule of the MTP joint.
- Release both the medial and lateral collateral ligaments at the MTP joint to allow the proximal phalanx to glide plantarly over the metatarsal head.
- Forcefully flex the MTP joint past neutral and dorsiflex the ankle to neutral. Observe the resting posture of the toes. If the MTP joint can now be flexed past neutral, turn your attention to the fixed contractures of the interphalangeal joints.
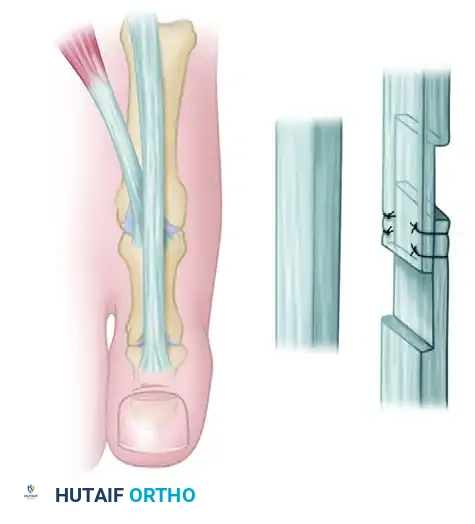
4. Management of the Hallux Interphalangeal Joint
If the IP joint of the great toe remains rigidly flexed, it must be addressed to prevent a "cock-up" deformity postoperatively.
- Approach the IP joint of the hallux through a separate L-shaped incision. The transverse limb of the "L" should be placed directly over the joint line.
Pitfall: The most common error during this approach is placing the transverse incision too far proximally, limiting joint access. Conversely, placing it too far distally risks irreversible damage to the germinal matrix of the nail.
- Incise the dorsal capsule, including the terminal tendon of the EHL, and release both collateral ligaments. Acutely flex the distal phalanx to open the joint.
- Using a Freer elevator, meticulously release the plantar plate from its proximal attachment on the proximal phalanx, and attempt to dorsiflex the IP joint to neutral.
- Decision Matrix for the IP Joint:
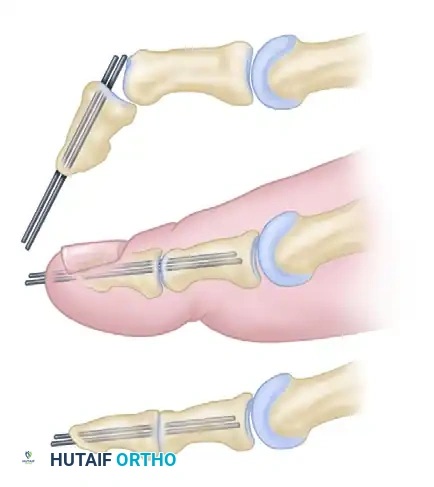
- If neutral position is attained: Maintain the IP joint in a straight position using two longitudinal transarticular Kirschner wires (K-wires) or a single obliquely placed wire.
- If neutral position cannot be attained: Proceed to an IP joint arthrodesis. Resect the articular cartilage and enough subchondral bone from both the proximal and distal phalanges to allow the joint to sit flush in a neutral position.
- Pinning Technique: Drive the K-wires retrograde through the distal phalanx so they emerge 2 to 3 mm plantar to the nail bed. Then, drive them proximally across the IP joint into the subchondral bone of the proximal phalanx.
Note: Occasionally, the K-wires must cross the first MTP joint for added stability, though a properly applied bulky forefoot dressing usually holds the MTP joint in the correct position without transarticular MTP pinning.
5. Correction of the Second Toe
Return to the first intermetatarsal space incision to manage the second toe MTP joint. Lengthen the EDL, tenotomize the EDB, and perform a dorsal capsulotomy and collateral ligament release at the second MTP joint, mirroring the steps performed on the hallux.
Next, address the rigid PIP joint contracture of the second toe:
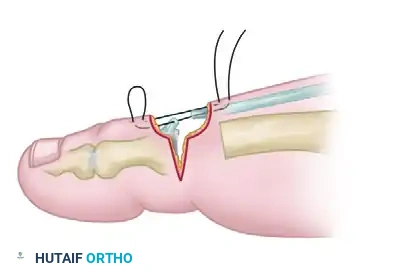
* Approach the second toe PIP joint through a dorsal elliptical incision. This incision design allows for the excision of redundant dorsal skin, creating a "dermodesis" effect that assists in maintaining extension.

- Incise the dorsal capsule and collateral ligaments of the PIP joint.
- Elevate the extensor tendon proximally. Perform a resection arthroplasty by removing the distal one-third of the proximal phalanx using a microsaw or bone rongeur.
- Ensure enough bone is resected so that the toe can be held in a neutral position at the PIP joint without any bony impingement.
- Closure and Dermodesis: Hold the joint in the proper position (0 to 15 degrees of flexion). Pass a suture through the skin and tendon, back through the tendon and skin, and tie it in a reverse skin-to-skin mattress configuration. This secures the dermodesis and stabilizes the resection arthroplasty.
6. Correction of the Lateral Toes (Third, Fourth, and Fifth)
- Third and Fourth Toes: Perform the procedure in a similar manner to the second toe. Approach the MTP joints through a single longitudinal incision in the third intermetatarsal space. Address the PIP joints via dorsal elliptical incisions.
- Fifth Toe: Approach the fifth toe through a straight lateral incision. Note that the fifth toe lacks an EDB tendon.
- If a painful callosity is present beneath the fifth metatarsal head, perform a partial plantar condylectomy, removing the plantar projection of the head flush with the metatarsal shaft.
- Suture the tendon of the abductor digiti minimi at the MTP joint to prevent postoperative medial subluxation of the fifth toe.
- Address the PIP joint through a dorsal elliptical incision (or a straight incision, though the dermodesis effect of the elliptical excision is highly beneficial for maintaining alignment).
7. Final Tendon Repair and Closure
- Return to the primary intermetatarsal incisions.
- With an assistant holding the MTP joints in 0 to 10 degrees of extension, repair the lengthened EHL and EDL tendons. Use 4-0 nonabsorbable sutures on a small, curved needle. Ensure appropriate tensioning; the tendons should be taut enough to prevent recurrent plantarflexion but not so tight as to recreate the hyperextension deformity.
- If a concurrent plantar fascia release was performed, suture the skin only using 3-0 nonabsorbable sutures to prevent deep tissue strangulation.
- Close all dorsal forefoot incisions with 4-0 or 5-0 nonabsorbable sutures.
ALTERNATIVE HISTORICAL PROCEDURES
While the soft tissue balancing and arthroplasty techniques described above are the modern standard, several historical procedures remain valuable in specific neuromuscular presentations:
- The Jones Procedure: Highly effective for severe, rigid clawing of the hallux, particularly in Charcot-Marie-Tooth disease. It involves a tendon transfer of the EHL to the neck of the first metatarsal, combined with an arthrodesis of the hallux IP joint. Instead of a Z-lengthening, the EHL is transected distally, routed through a drill hole in the first metatarsal neck, and sutured back onto itself. This provides a strong dorsiflexion force to the first ray, elevating a plantarflexed first metatarsal.
- The Hibbs Procedure: Utilized for the lesser toes, this involves transferring the EDL tendons to the lateral cuneiform or the lesser metatarsal necks, combined with EDB transfer to the distal EDL stumps.
The added biomechanical benefits of these tendon suspensions must be carefully weighed against their increased technical demands and the risk of overcorrection.
POSTOPERATIVE CARE AND REHABILITATION
Meticulous postoperative dressing application is as critical as the surgery itself. The dressing acts as an external splint, holding the soft tissues in their newly balanced alignment while healing occurs.
- Immediate Postoperative Phase: Apply a compressive, but strictly non-constricting, bulky forefoot dressing. The dressing must extend to the tips of the toes, holding them in the desired neutral alignment at both the MTP and IP joints. If K-wires were not used, this dressing is the sole restraint against recurrent deformity.
- Weight-Bearing: Weight-bearing to tolerance (e.g., ambulating to the bathroom) is permitted immediately after surgery using a rigid, wooden-soled postoperative shoe. The use of a walker or crutches is dictated by patient balance and whether bilateral surgery was performed. Shuffling is encouraged to minimize forefoot stress.
- Weeks 0 to 3: The initial bulky dressing is left completely undisturbed for 3 weeks, provided there are no signs of infection or excessive drainage. If a dressing change is mandatory before 3 weeks, the surgeon must apply the new dressing with the exact same meticulous attention to toe positioning.
- Weeks 3 to 4: At the 3-week mark, the bulky dressing is removed. Sutures and K-wires (if utilized and clinically ready) are extracted. A lighter, less bulky forefoot dressing is applied, continuing to hold the toes in proper alignment for an additional 7 to 10 days.
- 1 Month and Beyond: At 4 to 5 weeks postoperatively, the patient is transitioned into a wide, deep toe-box shoe. Active and passive toe range-of-motion exercises are initiated to prevent debilitating stiffness, particularly at the MTP joints. Full functional recovery and resolution of postoperative edema may take up to 6 months.
You Might Also Like
