Surgical Management of Hard and Soft Corns: Condylectomy, Resection Arthroplasty, and Syndactylization
Key Takeaway
Hard corns (heloma durum) and soft corns (heloma molle) frequently require surgical intervention when conservative measures fail. Operative management focuses on eliminating underlying bony prominences through condylectomy or resection arthroplasty. For interdigital soft corns, partial syndactylization combined with targeted exostectomy provides reliable relief. Meticulous surgical technique, thorough palpation to ensure complete bony resection, and structured postoperative splinting are critical to preventing recurrence and managing expected postoperative edema.
Introduction to Digital Hyperkeratotic Lesions
Digital hyperkeratotic lesions, commonly referred to as corns, represent a physiological response of the glabrous skin to pathological, repetitive mechanical stress. In orthopaedic practice, these lesions are broadly classified into two distinct clinical entities: the hard corn (heloma durum) and the soft corn (heloma molle). While conservative management remains the first-line approach, recalcitrant lesions associated with underlying structural osseous deformities frequently necessitate surgical intervention.
The fundamental principle of operative orthopaedics in the treatment of these lesions is the meticulous identification and resection of the offending bony prominence. Failure to address the underlying osseous impingement invariably leads to recurrence, patient dissatisfaction, and potential complications such as deep space infection or chronic ulceration.
Hard Corn (Heloma Durum) Management
A hard corn typically manifests over the dorsal or dorsolateral aspect of the proximal interphalangeal (PIP) joint or distal interphalangeal (DIP) joint of the lesser toes. It is frequently associated with fixed or flexible hammer toe and claw toe deformities, where the prominent phalangeal condyles abut against the rigid toe box of restrictive footwear.
Preoperative Considerations and Patient Counseling
Before proceeding with surgical intervention, a comprehensive clinical and radiographic evaluation is mandatory. Weight-bearing anteroposterior, lateral, and oblique radiographs of the foot are utilized to assess the joint spaces, phalangeal length, and the presence of exostoses.
Clinical Pearl: Patient expectations must be managed aggressively regarding postoperative edema. The soft tissue envelope of the lesser toes is exceptionally thin, lacking a robust subcutaneous layer to accommodate fluid shifts. Consequently, acute or chronic edema "has no place to hide." Enlargement of the toe frequently persists for weeks or even months following condylectomy or resection arthroplasty. Informing the patient preoperatively of this extended period of swelling is critical to preventing postoperative misunderstanding and dissatisfaction.
Surgical Technique: Condylectomy and Resection Arthroplasty
The primary goal of surgery is the decompression of the soft tissue envelope via the removal of the underlying bony prominence.
Anesthesia and Positioning:
* The procedure is typically performed under local anesthesia utilizing a digital block (e.g., 1% lidocaine and 0.5% bupivacaine without epinephrine).
* A sterile digital tourniquet (such as a Penrose drain or a specialized digital ring) is applied to the base of the toe to ensure a bloodless surgical field.
* The patient is positioned supine with the foot elevated and prepped in standard sterile fashion.
Incision and Exposure:
* A dorsolateral incision is utilized. The incision should skirt the medial border of the corn to avoid placing the surgical scar directly over the area of maximal shoe wear pressure.
* The incision begins 5 to 6 mm proximal to the eponychial fold (nail base) and extends proximally for approximately 1.5 cm, centered over the PIP joint.
* Careful blunt dissection is employed to protect the dorsal neurovascular bundles. The extensor tendon is identified and either retracted or longitudinally split to expose the joint capsule.
Osseous Resection:
* The joint capsule is incised, exposing the dorsolateral aspect of the condyle of the proximal phalanx.
* Using sharp dissection with a small-blade scalpel (e.g., #15 blade), the soft tissues are elevated off the bony prominence.
* A small sagittal saw or a sharp multi-action rongeur is utilized to resect the bony prominence from the dorsolateral condyle of the proximal phalanx.
* Attention must also be directed to the adjacent side of the middle phalangeal base. Any corresponding exostosis or prominence here must be resected to prevent "kissing" impingement.
Surgical Warning: Visual inspection of the resected area is notoriously deceptive. Palpation of the surgical bed after removing the prominence is far more revealing than inspection to determine the completeness of the removal. The surgeon must ensure that absolutely no bony prominence remains.
Resection Arthroplasty (The Radical Approach):
* In cases of severe deformity or recurrent hard corns, simple condylectomy may be insufficient. Resection of the entire head and neck of the proximal phalanx more reliably prevents recurrence and is considered the gold standard for intractable lesions.
* Trade-off: While highly effective at preventing corn recurrence, this radical resection invariably creates instability at the resected PIP joint (a "flail toe").
* This instability is managed postoperatively through meticulous taping and splinting. If the surgeon opts to perform only a localized condylectomy, the patient must be explicitly informed of the higher risk of recurrence and the potential future need for a formal resection arthroplasty.
Closure:
* The wound is irrigated copiously with sterile saline.
* The skin is closed using simple interrupted non-absorbable sutures (e.g., 4-0 or 5-0 nylon).
Postoperative Protocol for Hard Corns
- Immediate Post-op: A bulky, compressive sterile dressing is applied. The toe is splinted in a neutral alignment.
- Weight-Bearing: The patient is allowed to weight-bear as tolerated in a rigid wooden-soled postoperative shoe or a specialized shoe with the lateral toe box removed.
- Immobilization Phase: The initial appropriate dressings are worn continuously for 3 to 4 weeks to allow for soft tissue healing and initial fibrosis of the pseudoarthrosis (if resection arthroplasty was performed).
- Splinting Phase: Following suture removal (typically at 14-21 days), the toe is managed with tape splinting (buddy taping to the adjacent toe) for an additional 3 to 4 weeks to mitigate instability.
- Return to Footwear: At 4 to 6 weeks, the patient may transition to a wide toe-box shoe, progressing to normal footwear as edema subsides.
Soft Corn (Heloma Molle / Interdigital Corn) Management
Soft corns are exquisitely painful, macerated hyperkeratotic lesions that occur almost exclusively within the interdigital web spaces, most commonly in the fourth web space (between the fourth and fifth toes).
Pathoanatomy and Biomechanics
The etiology of the soft corn is rooted in the unique osseous anatomy of the lesser toes combined with the compressive forces of modern footwear.
* Standard Soft Corn: Caused by underlying pressure from the medial flare of the base of the distal phalanx of the fifth toe abutting against the prominent condyle of the PIP joint of the fourth toe.
* Deep "Web Corn": Located deep within the apex of the fourth web space. This is caused when the lateral condyle of the base of the proximal phalanx of the fourth toe and the medial side of the head of the proximal phalanx of the fifth toe pinch the adjacent interdigital skin surfaces together.
Diagnostic Pitfall: Appreciating these bony prominences by palpation and inspection in an unloaded, non-weight-bearing foot is often difficult. Separating the toes manually draws the corn into the center of the web space. However, in a shod, weight-bearing position, the biomechanics shift, and the corn actually sits superficial to the lateral base of the proximal phalanx of the fourth toe.
Due to the naturally moist environment of the interdigital web space, the developing callosity absorbs moisture, becomes macerated (soft), and is highly prone to ulceration. Once ulcerated, it is easily infected by the normal polymicrobial flora occupying the web space.
Conservative Management
Conservative treatment is mandatory before considering surgical intervention, particularly if an ulcer is present.
* Hygiene and Moisture Control: The web spaces must be washed twice daily with household soap and dried completely.
* Topical Agents: Application of antifungal and antibacterial powders.
* Mechanical Spacing: The use of lamb’s wool or a self-adherent rubber web spacer (doughnut pad) to mechanically separate the offending bony prominences.
* Ulcer Management: If an ulcer is present, it must be treated with drying agents, antibacterial solutions, and spacing until the web space is completely dry and epithelialized.
CRITICAL SURGICAL RULE: Surgery should never be performed through a moist, weeping, or actively infected interdigital ulcer. The risk of deep space infection, osteomyelitis, and subsequent digital amputation is unacceptably high.
Surgical Technique: Exostectomy and Syndactylization
If the soft corn remains painful, becomes recurrently infected, ulcerates despite adequate conservative care, or if the patient tires of the exhaustive daily maintenance required, operative treatment is highly justified.
The surgical resolution requires the removal of the underlying bony impingement. Usually, resecting only one side of the opposing prominence is sufficient; however, in severe or recurrent cases, resection of both sides may be necessary. Furthermore, a partial simple syndactylization of the fourth and fifth toes is highly effective for intractable cases.
Step 1: Exposure and Osseous Resection
The location of the hyperkeratotic lesion dictates the primary site of bony resection.
- Fifth Toe Resection: If the lesion is located more on the fifth toe side of the web, the head and neck of the proximal phalanx of the fifth toe should be resected. This is approached through either a dorsal, transverse, elliptical incision over the PIP joint or a dorsolateral, gently curved incision.
- Fourth Toe Resection: If the center of the ulceration or hyperkeratosis is more on the fourth phalangeal side, the lateral flare of the base of the fourth proximal phalanx should be resected flush with the diaphysis.
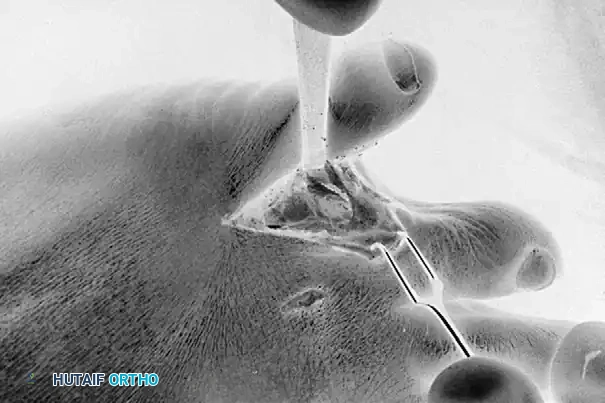
Exposure of the web space and meticulous resection of the lateral base of the fourth proximal phalanx using a sharp osteotome or sagittal saw.

Exposure and resection of the medial aspect of the proximal fifth toe. Note the careful protection of the surrounding soft tissue envelope.
Following the initial resection, the surgeon must manually compress the fourth and fifth toes together to simulate a weight-bearing, shod foot. The web space is deeply palpated to determine if any residual bony impingement exists. If the resection seems inadequate or if impingement persists, the opposite bony offender must also be resected.
Step 2: Partial Simple Syndactylization
For recurrent or highly intractable interdigital corns, combining the bony resection with a partial syndactylization eliminates the friction between the toes and permanently alters the web space anatomy.
- The opposing skin surfaces of the fourth and fifth toes within the web space are carefully excised to create raw, bleeding dermal beds.
- Cosmetic Consideration: Placing the digital limbs of the syndactyly incision slightly toward the plantar aspect of the adjacent toes is a crucial technique. This preserves the normal dorsal skin bridge, retaining the cosmetic cleft that the patient sees when looking down at their foot from the dorsal aspect.

Dorsal appearance of the closure following partial syndactylization. The dorsal aesthetic cleft is meticulously preserved to ensure high patient satisfaction.

Plantar appearance of the closure. The incisions are biased plantarly to allow for robust healing and to hide the surgical scar from dorsal view.
Wound Management and Closure:
* The surgical incisions used for bone resection and the syndactylization borders are closed with non-absorbable monofilament sutures.
* Ulcer Protocol: If a chronic (but dry and non-infected) ulcer was present, the ulcer itself should not be primarily closed. Ulcers in this region heal rapidly by secondary intention once the underlying bony pressure is removed. Attempting to pull macerated, compromised tissue together with sutures will result in dehiscence.
Postoperative Protocol for Soft Corns
- Initial Dressing: The toes are dressed with non-adherent gauze and a mild compressive wrap, holding them in the proper syndactylized position.
- Immobilization: The initial dressing is maintained for 3 weeks. The patient is placed in a rigid postoperative shoe to limit forefoot splaying during ambulation.
- Transition Phase: After suture removal at 3 weeks, the toes are taped together loosely (buddy taping) with a small amount of lamb’s wool placed between the distal, un-syndactylized portions of the toes to prevent moisture accumulation. This taping continues for an additional 3 weeks.
- Long-term Care: Patients are advised to utilize wide toe-box footwear to prevent lateral compression of the forefoot, which could stress the syndactyly site or provoke new lesions on adjacent digits.
Conclusion
The surgical management of hard and soft corns requires a deep understanding of forefoot biomechanics and a meticulous approach to osseous resection. Whether performing a condylectomy for a heloma durum or a complex resection with syndactylization for a heloma molle, the orthopaedic surgeon must prioritize complete removal of the bony impingement. By adhering to strict preoperative indications—especially regarding the resolution of active web space infections—and employing rigorous postoperative splinting protocols, surgeons can achieve excellent, long-lasting relief for these debilitating forefoot pathologies.
You Might Also Like
