Surgical Management of Hammer Toe and Claw Toe Deformities
Key Takeaway
Hammer toe and claw toe deformities arise from complex biomechanical imbalances between the intrinsic and extrinsic musculature of the foot. This comprehensive guide details the pathoanatomy, clinical evaluation, and step-by-step surgical management of these lesser toe deformities. From closing wedge osteotomies for fixed proximal interphalangeal contractures to soft tissue rebalancing for claw toes, mastering these techniques is essential for restoring foot biomechanics and alleviating patient pain.
INTRODUCTION TO LESSER TOE DEFORMITIES
Lesser toe deformities, specifically hammer toe and claw toe, are among the most common forefoot pathologies encountered by the orthopaedic foot and ankle surgeon. While often grouped together in clinical parlance, they represent distinct pathoanatomical entities with unique biomechanical etiologies. A thorough understanding of the intrinsic and extrinsic muscle balance, joint kinematics, and the flexibility of the deformity is paramount for selecting the appropriate surgical intervention.
The term hammer toe is used most often to describe an abnormal flexion posture of the proximal interphalangeal (PIP) joint. In a classic hammer toe, the metatarsophalangeal (MTP) joint and the distal interphalangeal (DIP) joint remain flexible and may rest in a neutral or slightly extended position. Conversely, a claw toe is characterized by a complex multi-joint deformity involving hyperextension of the MTP joint combined with flexion of both the PIP and DIP joints.
BIOMECHANICS AND PATHOANATOMY
The stability of the lesser toes relies on a delicate equilibrium between the extrinsic musculature (extensor digitorum longus [EDL], flexor digitorum longus [FDL]) and the intrinsic musculature (lumbricals, interossei).
The Intrinsic-Minus Foot and Claw Toe Deformity
Claw toe deformities are classically driven by an intrinsic-minus state. The intrinsic muscles normally act plantar to the axis of rotation of the MTP joint, causing flexion of this joint, while simultaneously extending the interphalangeal (IP) joints via their attachments to the extensor hood.
Loss of intrinsic function of the foot leads to a profound imbalance. This allows the EDL to unopposedly extend the MTP joint, while the FDL flexes the interphalangeal joints. Although the long extensors of the toes may extend the IP joints when the MTP joint is in neutral, the biomechanics shift drastically when an extension posture of the MTP joint develops. In this hyperextended state, the long extensor loses its functional excursion and can no longer extend the IP joints. The powerful flexors of the toe—specifically the long flexor, which attaches to the base of the distal phalanx—accentuate the deformity, driving the IP joints into rigid flexion.

Clinical Pearl: An extension posture of the claw toe significantly increases plantar pressure on the metatarsal heads, often leading to intractable plantar keratoses (IPK) and metatarsalgia. Addressing the MTP hyperextension is critical to relieving plantar forefoot pain.
Etiology of Hammer Toes
Although the causes of claw toe deformity (often neurologic, such as Charcot-Marie-Tooth disease or nerve laceration) can be easily understood through the intrinsic-minus model, most hammer toes have no underlying intrinsic imbalance.
Electromyographic (EMG) studies evaluating the phasic activity of the intrinsic muscles of the foot have found no activity of the intrinsic muscles during the first 35% of the gait cycle. Furthermore, with quiet standing, intrinsic muscle activity is entirely absent. Because the "hammering" of the toes is usually accentuated by standing, the lack of intrinsic activity during quiet standing implies that a loss of intrinsic function is not the primary cause of the hammer toe deformity.
Factors commonly thought to contribute to hammer toe deformity include:
* Improper Footwear: Long-term use of poorly fitting shoes. Crowding of the toes within an excessively tight toe box causes deformation of the MTP and IP joints that, over time, leads to flexible and eventually fixed deformities.
* Anatomical Variants: A "two-bone toe" or a long second ray can result in buckling of the toe during the propulsive phase of gait.
* Hallux Valgus: Severe hallux valgus causes the great toe to under-ride or over-ride the second toe, exerting direct mechanical pressure that forces the second toe into a hammered position.
* Systemic Conditions: Connective tissue disorders, inflammatory arthropathies (e.g., Rheumatoid Arthritis), and direct trauma.
CLINICAL EVALUATION
A meticulous physical examination is required to differentiate between flexible, semi-rigid, and fixed deformities, as this directly dictates the surgical algorithm.
Assessing Deformity Flexibility
The surgeon must evaluate the MTP, PIP, and DIP joints independently.
1. Kelikian Push-Up Test: Pressure is applied to the plantar aspect of the metatarsal head. If the toe straightens, the deformity is flexible and may be amenable to soft-tissue procedures (e.g., flexor-to-extensor transfer). If the deformity persists, it is fixed, necessitating bony resection or osteotomy.
2. MTP Joint Stability: The Lachman test (dorsal-plantar drawer test) of the MTP joint assesses the integrity of the plantar plate and collateral ligaments.

Differential Diagnosis: Neuroma vs. Synovitis
Pain in the lesser MTP joints can be multifactorial. It is critical to differentiate between an interdigital (Morton's) neuroma and idiopathic synovitis of the MTP joint, as the surgical treatments are vastly different.
- Interdigital Neuroma: Tenderness is localized to the interdigital web space, typically between the 3rd and 4th metatarsal heads. A Mulder's click may be palpable.
- Idiopathic Synovitis / Plantar Plate Tear: Tenderness is localized directly over the MTP joint capsule, specifically the dorsofibular capsule, fibular collateral ligament, or the plantar plate itself.
SURGICAL ANATOMY
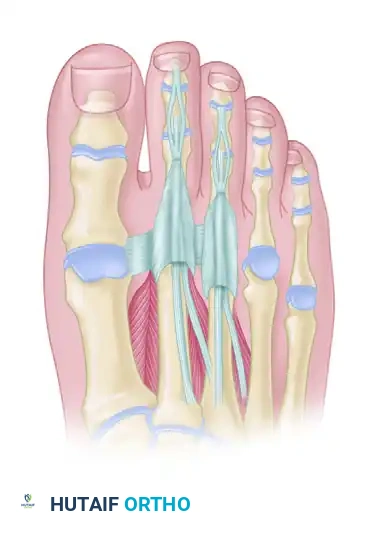
Understanding the osseous and tendinous architecture of the forefoot is essential for precise surgical execution. The following diagrams illustrate the critical relationships between the phalanges, the MTP joints, and the extensor/flexor mechanisms.
Anatomical overview of the lesser toe osseous structures, highlighting the proximal, middle, and distal phalanges where osteotomies and arthroplasties are performed.

Detailed view of the MTP and IP joint articulations. Note the congruency of the joints which is disrupted in chronic claw and hammer toe deformities.

The tendinous anatomy of the lesser toes, demonstrating the central slip of the extensor digitorum longus and the intricate balance of the lumbricals and interossei.
SURGICAL MANAGEMENT
The primary goal of surgery is to restore a plantigrade, pain-free foot with toes that comfortably clear the shoe toe box.
Surgical Warning: Never perform a bony procedure on a toe with compromised vascularity. Always assess capillary refill and palpable pulses preoperatively. If vascularity is questionable, non-invasive arterial studies (ABIs, toe pressures) are mandatory.
Technique 1: Closing Wedge Osteotomy for Fixed Hammer Toe
For a fixed flexion contracture of the PIP joint, a closing wedge osteotomy or a resection arthroplasty (DuVries technique) of the proximal phalanx is the gold standard. The closing wedge osteotomy creates a triangular wedge, generally 3 to 4 mm wide at the base, to correct the axial deformity.
Step-by-Step Procedure:
1. Incision: Make a dorsal longitudinal or transverse elliptical incision over the PIP joint. A transverse elliptical incision allows for the excision of redundant dorsal skin and the associated painful corn (heloma durum).
2. Dissection: Deepen the incision through the subcutaneous tissue. Identify and retract the dorsal neurovascular bundles medially and laterally.
3. Tendon Management: Perform a transverse tenotomy of the extensor tendon over the PIP joint to expose the joint capsule.
4. Capsulotomy: Perform a collateral ligament release and dorsal capsulotomy to fully expose the head of the proximal phalanx.
5. Osteotomy: Using a microsaw or bone rongeur, resect the distal articular surface of the proximal phalanx. To perform the closing wedge osteotomy, create a triangular wedge (3 to 4 mm wide at the dorsal base).
6. Closure of Osteotomy: Feather the lateral cortex, and close the osteotomy with firm finger pressure. Ensure the toe sits in a neutral, rectus alignment.
7. Fixation: While some surgeons rely on soft tissue closure alone for stability, most utilize a 1.1-mm (0.045-inch) or 1.6-mm (0.062-inch) Kirschner wire (K-wire). Drive the K-wire antegrade through the middle and distal phalanges, exiting the tip of the toe, and then retrograde it across the osteotomy site into the proximal phalanx.
8. Soft Tissue Closure: Close the deep structures, including the extensor tendon and capsule, with 3-0 Vicryl interrupted sutures. Close the skin with 4-0 Monocryl subcuticular sutures or simple interrupted non-absorbable sutures.
Technique 2: Soft Tissue Rebalancing for Claw Toe
Claw toes require addressing the MTP joint hyperextension in addition to the IP joint flexion.
Step-by-Step Procedure:
1. MTP Joint Release: Make a dorsal longitudinal incision over the MTP joint. Perform a Z-lengthening of the EDL tendon.
2. Capsulotomy: Perform a dorsal capsulotomy of the MTP joint. If the joint remains extended, release the collateral ligaments.
3. Plantar Plate Release: In severe, rigid cases, a McGlamry elevator may be passed dorsally over the metatarsal head to release the plantar plate and plantar capsule.
4. Flexor-to-Extensor Transfer (Girdlestone-Taylor): For flexible deformities, the FDL tendon is harvested at the level of the distal interphalangeal joint, split longitudinally, brought dorsally around the proximal phalanx, and sutured into the extensor hood. This converts the deforming flexor force into a stabilizing plantarflexion force at the MTP joint.
5. Pinning: The MTP joint is often pinned in neutral alignment with a K-wire driven from the toe tip, across the IP joints, and into the metatarsal to maintain alignment during soft tissue healing.
POSTOPERATIVE CARE AND REHABILITATION
Meticulous postoperative care is essential to prevent recurrence, malunion, or the dreaded "floating toe" complication.
Immediate Postoperative Protocol:
* Dressing and Taping: The surgical site is dressed with sterile non-adherent gauze. Crucially, the operated toe must be splinted to maintain alignment. The second toe is "buddy taped" to the first toe with up to six 12-mm wide strips of adhesive surgical tape. These strips are placed dorsally and plantarly on the hallux and second toe, acting as a dynamic splint.
* Duration of Taping: The tape is kept in place for 2 weeks, though many surgeons advocate for continued buddy taping for up to 6 weeks to prevent dorsal contracture.
* Weight-Bearing Status: Patients are placed in a stiff-soled postoperative shoe. Heel-weight-bearing or flat-foot weight-bearing is permitted immediately, provided the stiff sole prevents toe-off forces. The stiff-soled shoe is worn strictly for 2 to 4 weeks.
* Pin Management: If K-wires were used, they are typically left protruding from the tip of the toe and capped. They are removed in the clinic at 4 to 6 weeks postoperatively.
Long-Term Rehabilitation:
* After the initial 2 to 4 weeks, and following pin removal (if applicable), patients are allowed to transition to wide toe-box running shoes.
* Patients may slowly return to normal activities as tolerated.
* Active and passive plantarflexion exercises of the MTP joint are initiated at 4 weeks to prevent stiffness and the development of a floating toe.
COMPLICATIONS AND PITFALLS
Despite high success rates, lesser toe surgery carries specific risks that the orthopaedic surgeon must anticipate:
- Floating Toe Deformity: Often caused by over-resection of the proximal phalanx, excessive dorsal MTP release, or failure to address a plantar plate deficiency. The toe fails to purchase the ground during stance phase.
- Recurrence: Inadequate bony resection or failure to recognize and treat an underlying equinus contracture or intrinsic-minus state can lead to recurrence of the claw or hammer toe.
- Vascular Compromise: Aggressive correction of a severe, chronic deformity can stretch the neurovascular bundles, leading to arterial spasm or thrombosis. If the toe appears blanched postoperatively, the K-wire should be removed, the toe slightly flexed, and warm compresses applied. If perfusion does not return, all sutures must be removed.
- Infection and Pin Tract Issues: Exposed K-wires carry a risk of superficial pin tract infections. Patients must be educated on keeping the pin sites clean and dry. Oral antibiotics are usually sufficient for superficial erythema.
CONCLUSION
The successful management of hammer toe and claw toe deformities requires a profound understanding of forefoot biomechanics and a meticulous, step-wise approach to clinical evaluation. By accurately differentiating between flexible and fixed deformities, and by addressing both the osseous and soft-tissue components of the pathology, the orthopaedic surgeon can reliably restore function, alleviate pain, and improve the quality of life for patients suffering from these complex lesser toe pathologies.
You Might Also Like
