
Guided Growth to Correct Limb Deformity
- ###
- ## DEFINITION
- The anatomic axis is the mid-diaphyseal line of a bone. The anatomic angle of the lower extremity consists of the angle between the anatomic axis of the femur and tibia (normal = 5 to 9 degrees valgus).
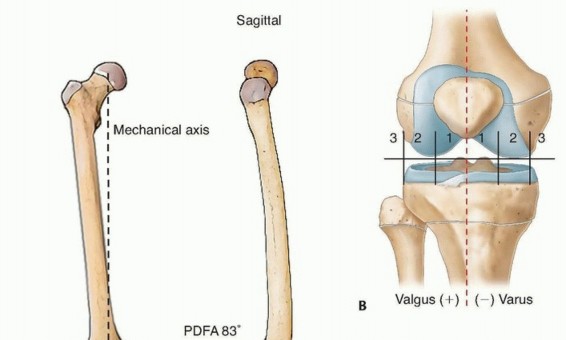
- The mechanical axis represents the weight-bearing alignment of a bone or an extremity in either the coronal or sagittal plane. It is a straight line connecting the proximal and distal extent of the bone regardless of its anatomic alignment. For example, the normal mechanical axis of the lower extremity in the coronal plane is a straight line from the center of the femoral head to center of the distal tibia and
- passes through the middle of the knee (FIG 1).14
-
###

-

- ###
- FIG 1 • A. The mechanical axis is a straight line drawn on a full-length, standing AP, or lateral radiograph of the lower extremity connecting the center of the femoral head to the center of the distal tibia. The normal angles for LDFA, MPTA, and LDTA will assist in identifying the location of deformity in the coronal plane, and PDFA, PPTA, and ADTA likewise will locate deformity in the sagittal plane. B. Dividing the knee into zones, the mechanical axis should pass through the central one-third of the joint. Deviation into zone 2 or 3 indicates deformity which may require surgical intervention.
- ###
- The mechanical axis is used to assess coronal and sagittal plane deformity and guide surgical correction to restore a normal weight-bearing alignment. Sagittal plane deformity can also be manipulated to improve the amount of extension at the knee or dorsiflexion at the ankle.
- ### Symmetric physiologic varus is expected between birth and 18 to 24 months, which transitions to a physiologic valgus deformity that is maximal at 3 to 4 years and should correct by 6 to 8 years of age.18
- ### P.551
- ### The physis is located at the junction of the epiphysis and metaphysis of long bones and is responsible for longitudinal growth. Consisting of chondrocytes in an extracellular matrix, the cells are oriented
- ### longitudinally in four distinct zones: the resting zone, the proliferative zone, the zone of hypertrophy, and the zone of provisional calcification.
- The zone of Ranvier is located at the periphery of the physis and contributes to circumferential growth of the physis.
- The perichondrial ring of LaCroix is an extension of the diaphyseal bone and periosteum and stabilizes the physis to the periosteum of the bone enhancing the shear strength of the growth plate.1
- The Heuter-Volkmann principle states that compression of the growth plate results in slowing the rate of bone growth. Delpech law is related in that tension across the growth plate increases the rate of bone growth.
- Guided growth or growth modulation techniques use the Heuter-Volkmann principle to affect the rate of growth at one part of the physis relative to another to gain correction of deformity in the coronal or sagittal plane. Common lower limb deformities that are treated with guided growth include pathologic:
- Genu varum and genu valgum19 Knee flexion contracture8, 16 Ankle valgus20
- Ankle plantarflexion contracture
- Hip varus and valgus23
- ### ANATOMY
- ### Mechanical and anatomic axis of lower extremity (see FIG 1A)15
- ###
- Hip
- ###
- ### Neck-shaft angle (NSA) = 130 degrees Knee
- ###
- ###
- Lateral distal femoral angle (LDFA) = 87 degrees Medial proximal tibia angle (MPTA) = 87 degrees Posterior distal femoral angle (PDFA) = 83 degrees Posterior proximal tibia angle (PPTA) = 81 degrees
- ### Ankle
- ###
- ### Lateral distal tibia angle (LDTA) = 89 degrees Anterior distal tibia angle (ADTA) = 80 degrees
- ### Center of rotation of angulation (CORA) is the location of deformity in a long bone. If a single point of deformity exists, the point of intersection between the proximal mechanical axis and the distal mechanical axis is the CORA and it should correspond to anatomic deformity. If a constructed CORA does not correspond with obvious anatomic deformity, another deformity must exist. Therefore, deformity correction should occur at the
- CORA to restore the mechanical axis.14
- ### Assessment of the physis should occur to ensure adequate growth is available for guided growth. This would
- include checking for physeal bars and to identify whether the physis is normal or pathologic secondary to an underlying etiology.
- ### Secondary problems
- ###
- ###
- Limb length discrepancy Rotational problems Osteochondritis dissecans
- ### Angular problems resulting in subluxation
- ###
- ### Hip—coxa valga Patella—genu valgum
- PATHOGEN ESIS
- ### Physiologic
- ###
- Idiopathic genu valgum Heuter-Volkmann principle
- ### Infantile and adolescent tibia vara
- ### Acquired (insult to the physis)—trauma, infection, radiation, iatrogenic, juvenile inflammatory arthritis, osteochondroma
- ### Congenital (condition affecting the health/growth of the physis)—skeletal dysplasia, focal fibrocartilaginous dysplasia, osteogenesis imperfecta, multiple hereditary exostosis, Ollier disease, Maffucci syndrome
- ### Metabolic bone disease (the physis is susceptible to the Heuter-Volkmann principle at the age of physiologic angulation, for example, onset before 2 years of age will lead to progressive varus, after 4 or 5 years of age will lead to progressive valgus)—rickets, renal osteodystrophy
- ### Adaptive response to a long bone deformity
- ### NATURAL HISTORY
- ### Physiologic = spontaneous resolution
- ### Progressive angular deformity can cause gait disturbance, limitations in function, and pain.
- ### There is no consistent evidence demonstrating what degree of malalignment could lead to osteoarthritis and at what age. Various biomechanical and gait studies describe increased force through the medial and lateral compartments with genu varum and valgum, respectively, but this has not been shown to cause
- osteoarthritis.4, 9, 12, 24
- ### PATIENT HISTORY AND PHYSICAL FINDINGS
- ###
- History is important to identify underlying pathology and determine growth potential. Current symptoms
- ###
- Pain, functional limitations, cosmetic concerns Observe gait
- ### Thrust, instability, crouch, equinus
- ###
- Assess for limb length discrepancy and rotational profile. Joint examination
- ###
- Range of motion of affected and adjacent joints Joint instability and pain
- ### Foot deformities
- ### IMAGING AND OTHER DIAGNOSTIC STUDIES
- ###
- Plain radiographs (as indicated) Bone age
- ### Lower extremity
- ###
- ###
- Standing, full-length anteroposterior (AP) alignment radiograph Lateral views of the lower extremities and joints involved Consider comparison views
- ### Consider scanogram
- ### Standing lateral foot film to assess foot height
- ### Computed tomography (CT)—most accurate assessment of rotational profile and best method to assess individual bone lengths in children with sagittal plane joint contractures
- ### CT or magnetic resonance imaging (MRI)—identifies a physeal bar
- DIFFERENTIAL DIAGNOSIS
- Physiologic
- Idiopathic genu valgum
- P.552
- Infantile and adolescent tibia vara
- Acquired: trauma, infection, radiation, iatrogenic, juvenile inflammatory arthritis, osteochondroma, adaptive response to a long bone deformity
- Congenital: skeletal dysplasia, focal fibrocartilaginous dysplasia, osteogenesis imperfecta, multiple hereditary exostosis, Ollier disease, Maffucci syndrome
- Metabolic bone disease: rickets, renal osteodystrophy
- ###
- NONOPERATIVE MANAGEMENT
- ### Pathologic conditions by definition are progressive and therefore not commonly amenable to observation or bracing.
- ### Metabolic disorder—treat and optimize underlying condition first, then if progressive deformity remains, guided growth is indicated.
- ### SURGICAL MANAGEMENT
- ### Progressive angular deformity resulting in pain or functional limitation
- ###
- Must have a physis with sufficient growth remaining (variable based on location of physis, patient, and pathology). It is important to remember that in some syndromes, the radiographic presence of an open growth plate does not ensure that the physis is growing sufficiently to correct deformity via guided growth.
- ### Surgical options
- ###
- Temporary hemiepiphysiodesis
- ###
- Rigid stapling
- ###
- Percutaneous screw (Metaizeau) Tension band plate and screws
- ###
- ### Stainless steel or titanium Cannulated or solid screws One or two plates
- ### Permanent hemiepiphysiodesis
- ###
- Modified Phemister technique
- ###
- Percutaneous drilling
- ### Preoperative Planning
- ### Ensure physis has adequate growth remaining to allow guided growth.
- ###
-

-

- ###
- FIG 2 • A. A 13-year-old girl with knee pain and difficulty with ambulation secondary to genu valgum. B. Standing AP radiograph of her lower extremities demonstrating bilateral genu valgum with abnormal LDFA bilaterally and an abnormal MPTA on the right tibia. She was indicated for bilateral medial distal femoral
- guided growth and right medial proximal tibia guided growth. C. Standing AP radiograph at 7 month postoperatively demonstrates normalization of her mechanical axis. (Courtesy of UW Pediatric Orthopaedics.)
- ###
- Consider placing an implant in an adjacent bone that is normal to accelerate correction of limb deformity. For example, in adolescent Blount disease, it may be necessary to guide growth of both the lateral tibia and lateral femur in an obese patient with less than 2 years of growth remaining.
- ### Identify the CORA and the corresponding growth plate(s) to affect correction of the deformity.
- ### Select the proper technique and implant. Specifically for tension band plates, options exist for metal (titanium or stainless steel) and screw type (cannulated or solid).
- ### Positioning
- ###
- Radiolucent operating table Tourniquet
- ### Fluoroscopy
- ### Approach
- ### Hemiepiphysiodesis (temporary or permanent) should be performed on the convex side of the deformity.
- ###
- The implant should be placed midsagittal on the bone when attempting to correct pure coronal plane deformity to avoid causing unintended sagittal plane deformity.
- ### Deformity may be in a plane that is not fully characterized by AP and lateral radiographs. Thus, the implant may need to be placed slightly anterior (to correct posterior slope) or posterior (to correct anterior slope).
- ### Open approach
- ###
- ###
- Medial distal femur or proximal tibia for genu valgum (FIG 2) Lateral distal femur or proximal tibia for genu varum (FIG 3) Anterior distal femur (FIG 4)
- ###
- Anterior distal tibia (FIG 5) Medial distal tibia (FIG 6)
- ### Percutaneous approach (Metaizeau)
- ###
- ### Medial distal tibia (FIG 7) Lateral hip
- ### Anterior knee (FIG 8)
- ###
- Lateral distal femur and proximal tibia Medial distal femur and proximal tibia
- ### P.553
-
###

-

- ###
- FIG 3 • A. A 7-year-old boy with traumatic amputation from a lawn mower injury with varus deformity causing difficulty with prosthetic wear. B,C. Although the CORA was a result of fracture malunion proximal to the distal femoral physis, guided growth was chosen as an alternative to osteotomy to straighten the limb and to improve prosthetic wear.
- ###
-
###

-

- ###
- FIG 4 • A,B. A 13-year-old boy with spastic diplegia who ambulates with a crouch knee gait, hamstring contracture, and knee flexion contracture. C,D. The patient was able to achieve full extension after hamstring release and anterior distal femoral guided growth with two modular implants placed next to the patella. To place these implants, two peripatellar incisions are needed to allow intra-articular placement of the devices across the physis and to ensure that no patellar contact ensues. (Courtesy of UW Pediatric Orthopaedics.)
-
###

-

- ###
- FIG 5 • A. An 8-year-old boy with 20 degrees residual equinus and talus dysmorphology after revision posterior medial release. B,C. Anterior distal tibia guided growth was performed after a CT scan ensured appropriate sizing of the epiphysis. In this procedure, a modular implant is placed by putting a guide pin into the distal tibia epiphysis and then a cannulated screw is placed. D,E. Two years postoperatively, the patient now has 10 degrees of ankle dorsiflexion. (Courtesy of UW Pediatric Orthopaedics.)
- ###
- P.554
- ###
-

- ###
- FIG 6 • Open medial distal tibia guided growth for ankle valgus is performed with a modular implant.
-
###

- ###
- FIG 7 • A. A 12-year-old boy with multiple hereditary exostosis who developed symptomatic ankle valgus underwent medial malleolus guided growth with a single percutaneously placed screw. B. AP radiograph at 3.5 years postoperatively demonstrates improvement in distal tibial articular alignment. (Courtesy of UW Pediatric Orthopaedics.)
- ###
-
###

-

- ###
- FIG 8 • A,B. A 12-year-old boy with spastic diplegia who ambulates with a crouch gait, hamstring contracture, and knee flexion contracture. C,D. Intraoperative fluoroscopy demonstrating preoperative PDFA. The child underwent hamstring transfer and distal femoral guided growth with placement of 6.5-mm cannulated screw positioned anterior in the center of the distal femur. E,F. Postoperative lateral radiographs show improved PDFA and full extension on clinical examination. (Courtesy of UW Pediatric Orthopaedics.)
- TECHNIQUES
-
Tension Band Plating for Pure Coronal Plane Deformity at the Knee
- ### The patient is positioned supine on a radiolucent table with a thigh tourniquet.
- ### Fluoroscopy is used to identify the distal femoral or proximal tibial physis (or both) and a 2- to 3-cm incision is made centered over the physis in the midsagittal plane.
- ### Medial distal femur—the fascia of medial quadriceps mechanism and medial patella femoral ligament is incised and the vastus medialis muscle is retracted anteriorly.
- ###
- Lateral distal femur: The iliotibial band is split longitudinally. Medial proximal tibia: The pes anserine is split longitudinally.
- ### Lateral proximal tibia: The anterior compartment may be left intact if the plate does not overlap or may need to be incised longitudinally and the muscle retracted.
- ### The dissection continues until periosteum is visualized but not violated.
- ### A guide pin is inserted into the physis, which serves to center the plate at the physis. Fluoroscopy is used to confirm proper position.
- ### A properly sized plate is chosen and placed over the guide pin through the center hole (TECH FIG 1A).
- ###
- P.555
- ###
-

-

- ### TECH FIG 1 • A. A guide pin has been placed into the physis and the plate slid over the guide pin to properly center it. B. An epiphyseal pin is placed parallel or slightly divergent to the physis. C. A metaphyseal pin is placed second aiming parallel or slightly divergent to the physis. D,E. The near cortex was drilled and then fully threaded cannulated screws were placed over the guide pins. F. Lateral fluoroscopic image of the proximal tibia demonstrating the midsagittal positioning of the plate.
- ### Guide pins are then inserted through the plate in a parallel to slightly divergent fashion from the physis, placing the epiphyseal pin first, followed by the metaphyseal pin. Confirm proper position with fluoroscopy and avoid inadvertent physeal or joint disruption (TECH FIG 1B,C).
- ### The near cortex is drilled and then a fully threaded screw is inserted (cannulated or solid screws depending on surgeon preference) (TECH FIG 1D,E).
- ### Confirm final screw positions with fluoroscopy (TECH FIG 1E,F).
- ### Finish with irrigation, routine wound closure, local anesthesia, dressing, and immobilization.
-
Hemiepiphyseal Stapling
- ###
- The surgical approach is the same as tension band plating, with care taken not to disrupt the periosteum. The physis is marked with a guide pin and the proper position is confirmed with fluoroscopy.
- ### Usually, only one rigid staple is inserted, straddling the physis with one side of the staple in the epiphysis and the other in the metaphysis. Some surgeons use more than one staple.
- ### Confirm final position with fluoroscopy. Then irrigation, routine wound closure, local anesthesia, dressing, and immobilization.2
-
Metaizeau Technique
- ### A percutaneous approach is used to place a transphyseal screw under fluoroscopic guidance.
- ### In the distal femur, the screw can be placed across the desired location in the physis from either the medial or lateral side of the bone.
- ### In the proximal tibia, a single screw is placed from the medial side to tether the lateral growth plate (genu varum) or placed from the lateral side to tether the medial growth plate (genu valgum). The screw passes from the metaphysis to the epiphysis and crosses the physis near its periphery.
- ### The goal is to place the tip of the screw into the epiphysis just across the physis at the peripheral aspect of the bone in order to maximally affect angular growth.
- ###
- Upon obtaining desired correction, the screw is able to be removed.10
- 4. ### Modified Phemister Technique
- P.556
- ### The surgical approach to the physis is the same as tension band plating. A headlamp or lighted sucker tip may help with visualization. The periosteum, however, is incised longitudinally with this technique.
- ### Periosteal flaps are made to allow visualization of the physis.
- ### A hemiepiphysiodesis is performed by removing a square block of bone that includes the physis (1 to 2 cm from anterior to posterior, 1 to 2 cm from superior to inferior, and 1 cm deep).
- ### Through the void left by the removed block of bone, the physis can be visualized and the exposed growth plate is then curetted anterior and posterior to allow a bony tether to occur. Care is taken to avoid to curette too much bone in order to effectuate a partial growth arrest as opposed to compete physeal arrest by extensive curettage across the physis.
- ### The bone block should be reinserted in an orientation 180 degrees from its original position to create a bone bridge.
- ### This technique is permanent and requires precise timing and calculation to ensure proper correction before growth plate closure.6, 17
-
Percutaneous Drilling
- ### Fluoroscopy is used to identify the physis and a 1-cm incision is made in the desired sagittal plane.
- A guide pin is inserted into the physis and proper position is confirmed with fluoroscopy.
- Anterior cruciate ligament (ACL) reamers are used to sequentially ream up to 1 cm to drill out the physis and curettes are able to be used to finalize the peripheral physeal removal. Similar to the open method, care is needed to avoid removing too much physis and thus limiting angular correction and resulting in complete arrest.
- Hemiepiphysiodesis is complete when a bone bridge is established. This technique is permanent and requires precise timing and calculation to ensure proper correction before growth plate closure.
- ###
- ### PEARLS AND PITFALLS
- ### Ensure good indications, patient and family education
-
Identify patients with a physis with adequate growth remaining to allow deformity correction.
-
Consider advanced imaging (CT and MRI) to assess for bony bars that will diminish effectiveness.
-
Educate families on expected rate of correction and the importance of close follow-up to ensure removal at the appropriate time to avoid undesired overcorrection.
- ### Prevent periosteal damage
-
When performing instrumented hemiepiphysiodesis, avoid damaging the periosteum with implant insertion or removal to prevent damage to the physis.
- ### Avoid soft tissue tethering
-
It is important to split and repair tendinous structures such as the pes anserinus and the medial patella femoral ligament during medial guided growth of the knee. Failing to place the implants under these structures can lead to painful tethering.
- ### Screw choice ▪ In obese patients, it may be desired to use stainless steel or solid screws to avoid fracture of the screw. This tends to happen at the metaphyseal location (FIG 9)
- ### Tension band plates
-
Tension band plates may need to be prebent to maintain a low profile to the bone, especially at the lateral proximal tibia.
-
###

-

- ###
- FIG 9 • A 9-year-old boy with juvenile Blount disease and distal femoral and proximal tibia deformity was indicated for guided growth. In this method, lateral epiphysiodesis was performed by placing guide pins for cannulated screws into the epiphysis and solid screws were placed in the metaphysis. The metaphyseal screws are prone to failure, which is why solid screws were chosen. (Courtesy of UW Pediatric Orthopaedics.)
- ###
- ### P.557
- POSTOPERATIVE CARE
- ###
- Local anesthetic or nerve block (use knee immobilizer for 24 hours in patients with femoral nerve block) Temporary immobilization for wound healing
- ###
- Activity as tolerated, physical therapy (PT) if necessary Follow-up
- ### Standing AP lower extremity radiograph taken at 3- to 6-month intervals
- ###
- Allow for slight overcorrection if there is growth remaining prior to implant removal (5 degrees).5, 7, 10, 11, 13, 19, 21, 22, 25
- ###
- Implant does not need to be removed if growth is finished and it is asymptomatic.
- OUTCOMES
- The rate of correction is variable between patients. A published calculation estimates angular correction of 7 degrees per year at the distal femur and 5 degrees per year at the proximal tibia.3
- Potential for 5 degrees of rebound once the plate is removed and if growth remains.
- ###
- COMPLICATIONS
- Implant failure—broken plate or screw with tension band plates; broken staples
- Implant loosening—staples may loosen; screws may lose purchase with tension band plates Wound complications in obese
- Infection Nerve damage
- Overcorrection or undercorrection
- ###
-
Scientific References
🔗 Read the comprehensive guide:
Ponseti Clubfoot Correction: The Role of Percutaneous Achilles Tenotomy
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding guided-growth-to-correct-limb-deformity
01
Chapter 1
14 min
Unlock Straighter Limbs: Guided Growth to Correct Deformity
02
Chapter 2
40 min