Orthopedic Anatomy 2026 MCQs: Board Review Questions & Answers (Part 1)
30 مارس 2026
25 min read
28 Views

Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Orthopedic Anatomy 2026 MCQs: Board Review Questions & Answers (Part 1). Top-rated Orthopedic Anatomy 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Question 1
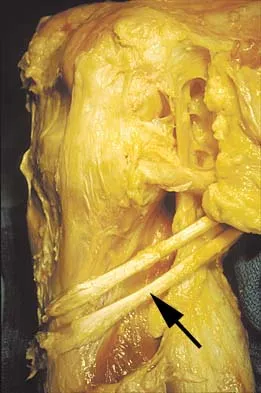
During a retroperitoneal approach to the L4-5 disk, what structure must be ligated to safely mobilize the common iliac vessels toward the midline from laterally and gain exposure?

Explanation
To mobilize the common iliac vessels across the midline, the iliolumbar vein must be ligated. It has a short trunk and can be torn if mobilization is attempted without ligation. It is the only branch off the common iliacs (there are no arterial branches) prior to the terminal branches, the internal (hypogastric) and external iliacs. The middle sacral vessels run distally from the axilla of the bifurcation and are a factor when accessing the L5-S1 disk. Baker JK, Reardon PR, Reardon MJ, et al: Vascular injury in anterior lumbar surgery. Spine 1993;18:2227-2230.
References:
- Lewis WH: Gray's Anatomy of the Human Body: The Veins of the Lower Extremity, Abdomen, and Pelvis, ed 20. Philadelphia, PA, Lea & Febiger, 2000.
Question 2
The injection shown in Figures 1a and 1b would most benefit a patient who reports which of the following symptoms?


Explanation
1b The images demonstrate a L5 selective root block as it exits the L5-S1 foramen. This root block best helps relieve pain or paresthesias in the L5 distribution, which is the dorsal first web space and the great toe. The lateral foot is an S1 distribution and would need to be blocked through the posterior first sacral foramen. The anterior shin and thigh represent the L4 root which exits a level above this at the L4-5 foramen. A stocking distribution is nonanatomic and not indicative of a specific root. Magee D: Principles and concepts, in Orthopaedic Physical Assessment, ed 3. Philadelphia, PA, WB Saunders, 1997, pp 1-18.
References:
- Aeschbach A, Mekhail NA: Common nerve blocks in chronic pain management. Anesthesiol Clin North Am 2000;18:429-459.
Question 3
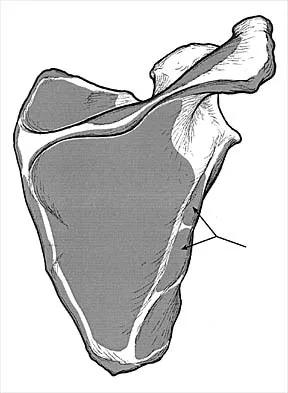
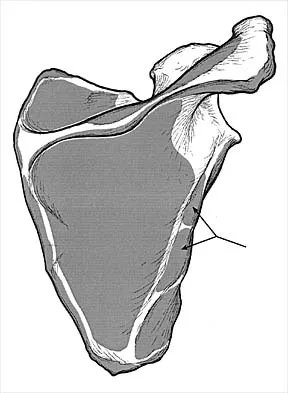
In Figure 2, which of the following structures is the primary stabilizer in preventing valgus instability of the elbow?


Explanation
The anterior bundle of the medial collateral ligament is the prime stabilizer of the medial aspect of the elbow and is indicated by "B" in the figure. When intact, this anterior bundle of the medial collateral ligament is a restraint to valgus instability of the elbow. The posterior bundle is regarded as a secondary stabilizer of the medial elbow (C). The transverse bundle (D), annular ligament (A), and biceps tendon (E) do not play a role in valgus stability of the elbow. Jobe F, Elattrache N: Diagnosis and treatment of ulnar collateral ligament injuries in athletes, in Morrey B (ed): The Elbow and Its Disorders. Philadelphia, PA, WB Saunders, 1993, p 566.
References:
- Wilkins KE, Morrey BF, Jobe FW, et al: The elbow. Instr Course Lect 1991;40:1-87.
Question 4
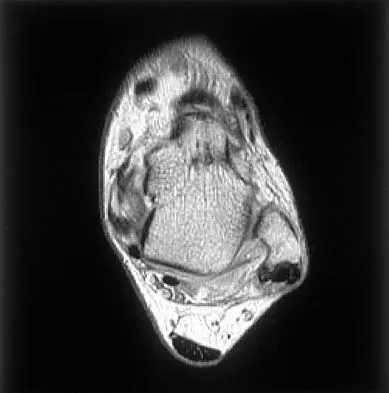
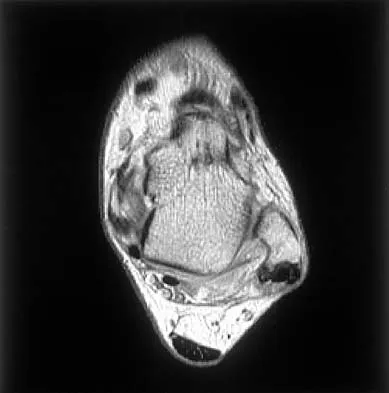
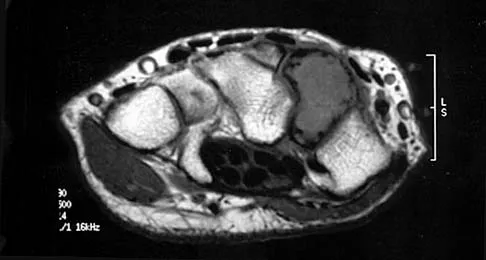
When performing surgical excision of the lesion shown in the MRI scan in Figure 3, what nerve is most likely at risk?

Explanation
The MRI scan shows a large mass (lipoma) in the thenar muscles of the palm. The recurrent motor branch of the median nerve innervates the thenar muscles. The anterior interosseous nerve (AIN) in the proximal forearm innervates the flexor pollicis longus, pronator quadratus, and flexor digitorum pollicis to the index and frequently the middle finger. The terminal branch of the AIN innervates only the wrist capsule. The palmar cutaneous branch of the ulnar nerve is a sensory structure to the hypothenar area. There is no commonly described recurrent branch of the ulnar nerve.
References:
- Kozin SH: The anatomy of the recurrent branch of the median nerve. J Hand Surg Am 1998;23:852-858.
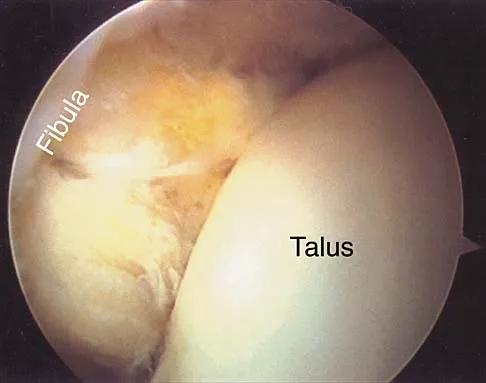
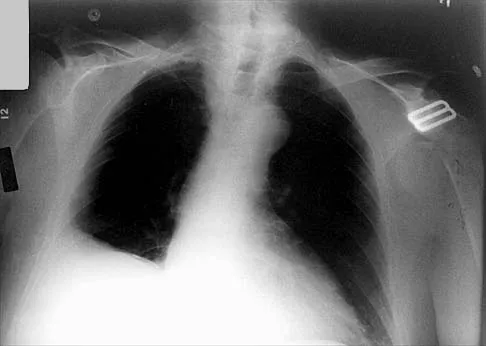
Question 5
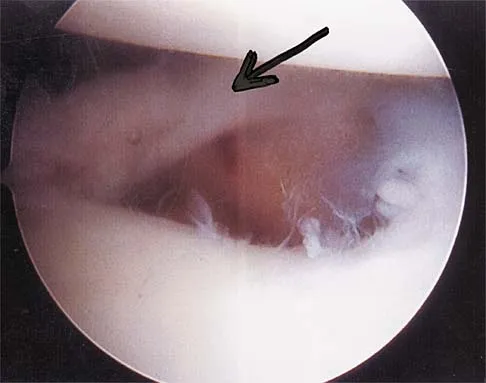
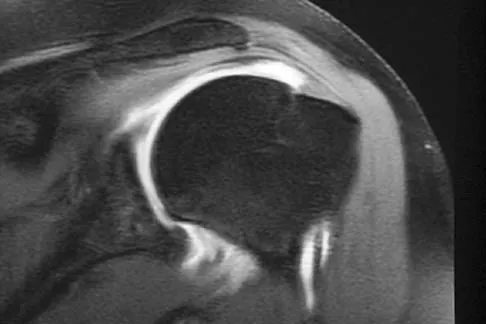
Figure 4a shows the radiograph of a 20-year-old man who has an injury to the right shoulder. Figure 4b shows an arthroscopic view (posterior portal). The arrow points to a



Explanation
4b The radiograph shows an anterior dislocation of the shoulder. A frequently encountered sequela of this is a compression fracture of the posterolateral humeral head, commonly referred to as a Hill-Sachs defect. The arthroscopic view of the glenohumeral joint visualizes the posterior aspect of the humeral head. In the image, the area devoid of cartilage to the right is the bare area. The indentation seen to the left is a Hill-Sachs defect. Matsen FA, Thomas SC, Rockwood CA, et al: Glenohumeral instability, in Rockwood CA, Matsen FA (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 611-754.
References:
- Mazzocca AD, Noerdlinger M, Cole B, et al: Arthroscopy of the shoulder: Indications and general principals of techniques, in McGinty JB (ed): Operative Arthroscopy, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 412-427.
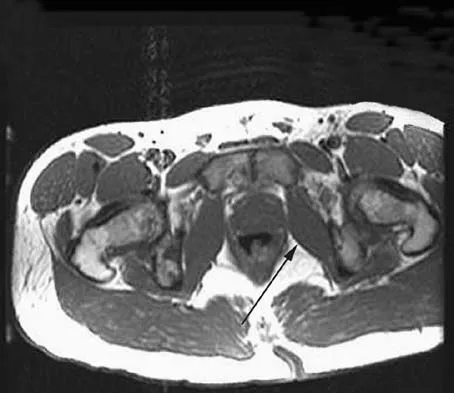
Question 6
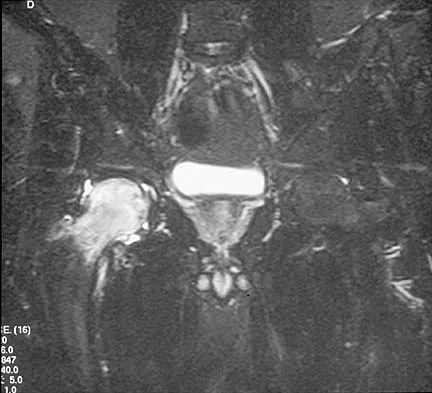
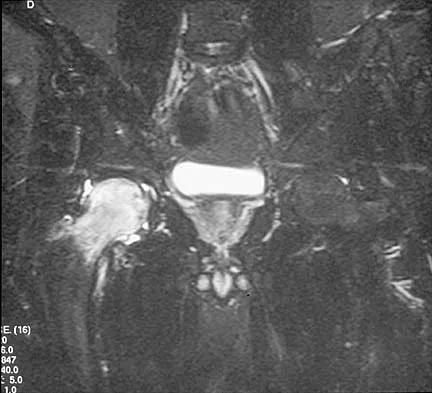
A 15-year-old girl who swims the breaststroke has had hip pain after training excessively for a national level competition. Based on the MRI scans shown in Figures 5a through 5c, what is the most likely diagnosis?



Explanation
5b 5c The MRI scans reveal open physes but no evidence of a slipped capital femoral epiphysis, labral tear, or acetabular dysplasia. The femoral neck does not show evidence of a fracture. The muscle tear seen on the right side lies near the musculotendinous junction of the external rotators of the hip at the level of the lesser trochanter, representing the obturator externus. This is consistent with the forced motion required for the breaststroke kick. Grote K, Lincoln TL, Gamble JG: Hip adductor injury in competitive swimmers. Am J Sports Med 2004;32:104-108.
References:
- Clemente C: Anatomy: A Regional Atlas of the Human Body, ed 3. Baltimore-Munich, Urban and Schwarzenberg, 1987, Figures 429, 430.
Question 7
During placement of an external fixator for a distal radius fracture, the most commonly injured nerve is a branch of which of the following nerves?
Explanation
Pin track infections and sensory injuries are among the most common complications of external fixation for distal radius fractures. The proximal pins of most distal radius external fixators are placed in the "bare area" of the distal radius, about four finger-breadths above the radial styloid. This corresponds to the area where the dorsal sensory branch of the radial nerve penetrates the fascia dorsal to the brachioradialis tendon to become a subcutaneous structure. Injury to the superficial radial nerve may produce painful dysesthesias and neuromas.
References:
- Beldner S, Zlotolow DA, Melone CP, et al: Anatomy of the lateral antebrachial cutaneous and superficial radial nerves in the forearm: A cadaveric and clinical study. J Hand Surg Am 2005;30:1226-1230.
Question 8
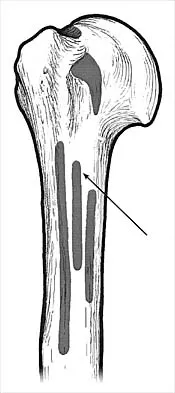
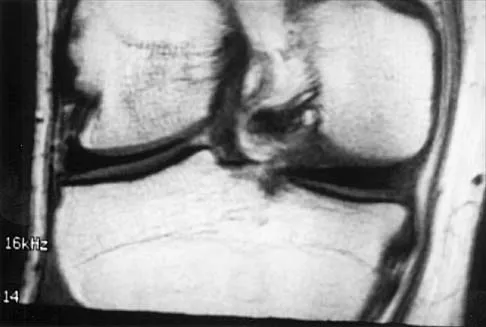
Figure 6 shows a sagittal oblique MRI scan. The arrow is pointing to what structure?
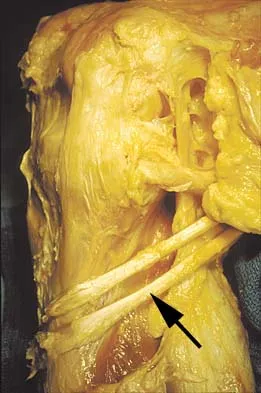

Explanation
The meniscofemoral ligaments connect the posterior horn of the lateral meniscus to the intercondylar wall of the medial femoral condyle. The ligament of Humphrey (arrow) passes anterior to the posterior cruciate ligament, whereas the ligament of Wrisberg passes posterior to the posterior cruciate ligament. One or the other has been identified in 71% to 100% of cadaver knees, with the ligament of Wrisberg being more common. Clarke HD, Scott WN, Insall JN, et al: Anatomy, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 3-66.
References:
- Miller TT: Magnetic resonance imaging of the knee, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 201-224.
Question 9
An 18-year-old woman sustains a twisting injury of the knee while skiing. Figures 7a and 7b show the radiograph and coronal MRI scan of the knee. In addition to the injury shown, what is the most likely associated injury?


Explanation
7b The MRI scan shows a Segond fracture, which is a small avulsion of the lateral joint capsule from the anterolateral aspect of the proximal tibia. It is almost always associated with anterior cruciate ligament rupture and often with a tear of either the medial or lateral meniscus. Goldman AB, Pavlov H, Rubenstein D: The Segond fracture of the proximal tibia: A small avulsion that reflects major ligamentous damage. Am J Roentgenol 1988;151:1163-1167. Sanders TG, Miller MD: A systematic approach to magnetic resonance imaging interpretation of sports medicine injuries of the knee. Am J Sports Med 2005;33:131-148.
References:
- Miller TT: Magnetic resonance imaging of the knee, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 201-224.
Question 10
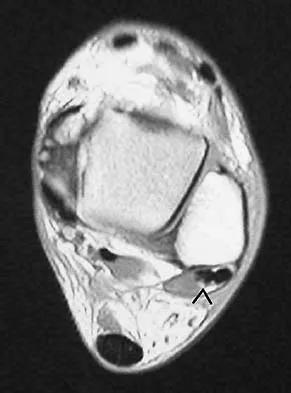
A 42-year-old athletic trainer has a persistent popping sensation about the lateral ankle associated with weakness and pain following a remote injury. Deficiency in what structure directly leads to this pathology?


Explanation
The patient has instability of the peroneal tendon. The superior peroneal retinaculum is the primary retaining structure preventing peroneal subluxation. It is a thickening of fascia that arises off the posterior margin of the distal 1 to 2 cm of the fibula and runs posteriorly to blend with the Achilles tendon sheath. The inferior peroneal retinaculum attaches to the peroneal tubercle of the calcaneus and is not involved in this pathology. A deficient groove in the posterior distal fibula may also be a contributing factor in the development of the condition.
References:
- Maffuli N, Ferran NA, Oliva F, et al: Recurrent subluxation of the peroneal tendons. Am J Sports Med 2006;34:986-992.
Question 11
A 21-year-old man sustains multiple gunshot wounds to his right upper extremity. He can not extend his digits or his thumb but can extend and radially deviate his wrist. An injury to the radial nerve or one of its branches has most likely occurred at which of the following locations?

Explanation
In this patient, the radial nerve is most likely injured at the level of the radial neck. The radial nerve emerges from the posterior cord of the brachial plexus and travels along the spiral groove of the humerus. At the level of the lateral humeral condyle, the radial nerve branches into the posterior interosseous nerve after giving off two cutaneous branches, the superficial radial and the posterior cutaneous. The posterior interosseous nerve travels through the supinator muscle and winds around the radial neck. At this level, the posterior interosseous nerve is vulnerable to injury, particularly following fracture or penetrating trauma. Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System, Part 1: Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy Corporation, 1987, vol 8, p 53.
References:
- Hollinshead W: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, vol 3, pp 428-429.
Question 12
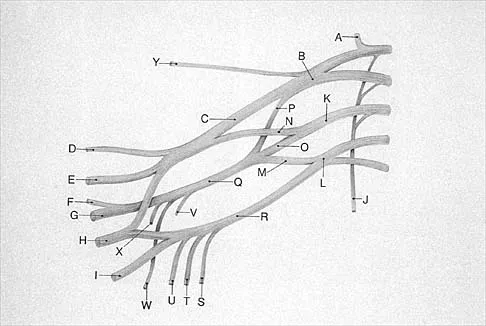
A woman with a neck and chest tumor has weakness in the biceps and paresthesias in the thumb. Brachioradialis and infraspinatus function are normal. The lesion is affecting which of the following structures?




Explanation
The lateral cord terminates as the musculocutaneous nerve and also contributes sensory fibers to the median nerve. Involvement of the C6 root or upper trunk could potentially cause weakness of the infraspinatus and the brachioradialis. The middle trunk and the posterior cord do not contribute motor fibers to the thumb or sensory fibers to the thumb.
References:
- Kline DG, Hudson AR: Nerve Injuries: Operative Results for Major Nerve Injuries, Entrapments and Tumors. Philadelphia, PA, WB Saunders, 1995, p 334.
Question 13
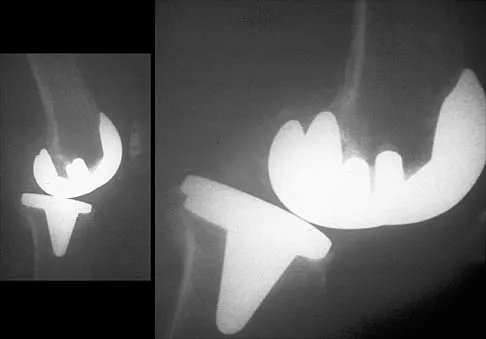
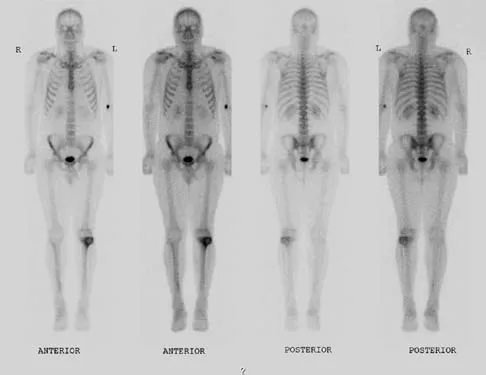
Figure 8 shows the radiograph of a 76-year-old man who has knee pain and swelling. History reveals that he underwent total knee arthroplasty 18 years ago. What is the most likely diagnosis?



Explanation
The radiograph reveals complete loss of joint space with particulate metal debris consistent with total polyethylene failure and metal-on-metal articulation. The components appear to be well fixed and minimal osteolysis is evident. Kilgus DJ, Moreland JR, Finerman GA, et al: Catastrophic wear of tibial polyethylene inserts. Clin Orthop Relat Res 1991;273:223-231.
References:
- Vince KG: Why knees fail. J Arthroplasty 2003;18:39-44.
Question 14
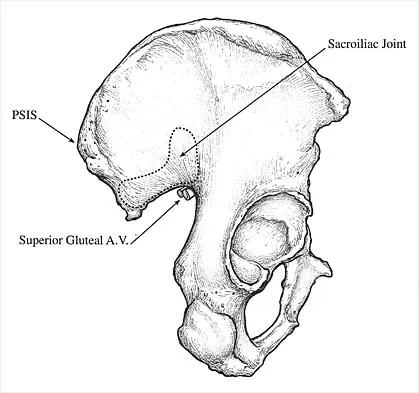
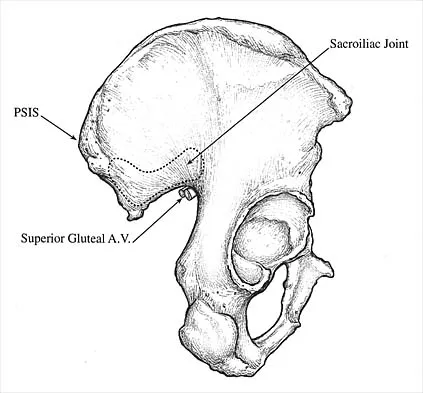
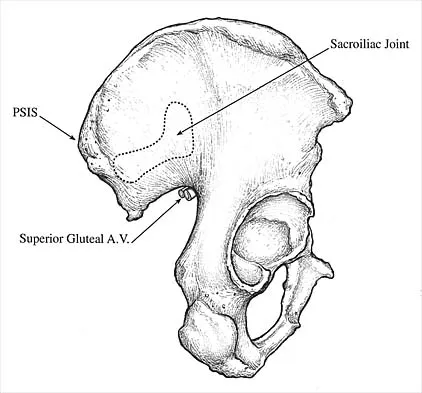
Which of the following radiographic images is best for detecting anterior acetabular deficiency in the dysplastic hip?

Explanation
The false profile view of Lequesne and de Seze is obtained with the patient standing with the affected hip on the cassette, the ipsilateral foot parallel to the cassette, and the pelvis rotated 65 degrees from the plane of the cassette. This view best assesses anterior coverage of the femoral head. Garbuz DS, Masri BA, Haddad F, et al: Clinical and radiographic assessment the young adult with symptomatic dysplasia. Clin Orthop Relat Res 2004;418:18-22.
References:
- Delauney S, Dussault RG, Kaplan PA, et al: Radiographic measurements of dysplastic adult hips. Skelelal Radiol 1997;26:75-81.
Question 15
Figure 9 shows the AP radiograph of a 65-year-old man who has knee pain and swelling. What is the most likely diagnosis?
Explanation
Although all the choices are known causes of joint degeneration (secondary osteoarthritis), only chondrocalcinosis shows distinct linear calcification of the cartilage due to deposition of calcium pyrophosphate crystals. Gout is a recurrent acute arthritis resulting from the deposition of monosodium urate from supersaturated hyperuricemic body fluids. Hemochromotosis is characterized by focal or generalized deposition of iron within body tissues. Arthritis may be present but is less common than other manifestations such as liver cirrhosis, skin pigmentation, diabetes mellitus, and cardiac disease. Rheumatoid arthritis is a nonspecific, usually symmetric inflammation of peripheral joints resulting in destruction of articular and periarticular structures. Ochronosis is a hereditary enzyme deficiency (homogentisic acid oxidase) resulting in deposition of homogentisic acid polymers in articular cartilage. Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 188.
References:
- Berkow R (ed): The Merck Manual, ed 14. Rathway, NJ, Merck, 1984, pp 910, 1176, 1200.
Question 16
If a surgeon inadvertently burrs through the midlateral wall of C5 during a anterior corpectomy, what structure is at greatest risk for injury?
Explanation
The vertebral artery is contained within the vertebral foramen and thus tethered alongside the vertebral body, making it vulnerable to injury if a drill penetrates the lateral wall. The C5 root passes over the C5 pedicle and is not in the vicinity. The C6 root passes under the C5 pedicle but is posterior to the vertebral artery and is only vulnerable at the very posterior-inferior corner. The carotid artery and the vagus nerve are both within the carotid sheath and well anterior. Pfeifer BA, Freidberg SR, Jewell ER: Repair of injured vertebral artery in anterior cervical procedures. Spine 1994;19:1471-1474.
References:
- Gerszten PC, Welch WC, King JT: Quality of life assessment in patients undergoing nucleoplasty-based percutaneous discectomy. J Neurosurg Spine 2006;4:36-42.
Question 17
In patients with displaced radial neck fractures treated with open reduction and internal fixation with a plate and screws, the plate must be limited to what surface of the radius to avoid impingement on the proximal ulna?
Explanation
The radial head is covered by cartilage on 360 degrees of its circumference. However, with the normal range of forearm rotation of 160 to 180 degrees, there is a consistent area that is nonarticulating. This area is found by palpation of the radial styloid and Lister's tubercle. The hardware should be kept within a 90-degree arc on the radial head subtended by these two structures. Smith GR, Hotchkiss RN: Radial head and neck fractures: Anatomic guidelines for proper placement of internal fixation. J Shoulder Elbow Surg 1996;5:113-117.
References:
- Caputo AE, Mazzocca AD, Santoro VM: The nonarticulating portion of the radial head: Anatomic and clinical correlations for internal fixation. J Hand Surg Am 1998;23:1082-1090.
Question 18
A 57-year-old man reports right hip pain that has been progressive for the past several months. The pain is exacerbated by weight-bearing activities and improves somewhat with rest. A radiograph is shown in Figure 10a and a coronal T1-weighted MRI scan is shown in Figure 10b. What is the most likely diagnosis?

Explanation
10b These are classic findings of osteonecrosis of the hip. The radiograph reveals the subchondral sclerotic pattern commonly seen in osteonecrosis and is quite extensive in this patient. The MRI scan reveals the typical serpentine-like region of low signal intensity with a central zone where the signal is similar to fat. Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA, WB Saunders, 2002, pp 3160-3162.
References:
- Sugano N: Osteonecrosis, in Fitzgerald R Jr, Kaufer H, Malkani A (eds): Orthopaedics. Philadelphia, PA, Mosby International, 2002, pp 877-887.
Question 19
The arrow in Figure 11 points toward a finding consistent with which of the following?

Explanation
The finding of a unilateral absent pedicle is often referred to as a winking owl sign and is a manifestation of pedicle destruction from metastatic disease. As the vertebral body is destroyed from the neoplastic process, it extends into the pedicle and destroys the cortical rim that normally creates the oval ring of the pedicle on an AP image. McLain R, Weinstein J (eds): Rothman-Simeone: The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, p 1173.
References:
- Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 674.
Question 20
The attachments of the transverse carpal ligament include which of the following structures?

Explanation
The transverse carpal ligament is the volar boundary of the carpal tunnel. It attaches to the scaphoid and trapezium radially and the pisiform and the hook of the hamate ulnarly. The ulna and trapezoid do not receive attachments of the transverse carpal ligament. Hollinshead W: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, vol 3, pp 471-472.
References:
- Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 168-170.
Question 21
A 23-year-old woman falls from a bicycle and sustains a right knee injury. Figures 12a through 12d show radiographs and MRI scans of the knee. What is the most likely diagnosis?




Explanation
12b 12c 12d The radiographs and MRI scans both show an avulsion of the anterior cruciate ligament, which has been described by Meyers and McKeever in three different fracture patterns. Type I fractures are nondisplaced or have minimal displacement of the anterior margin. Type II fractures have superior displacement of their anterior aspect with an intact posterior hinge. Type III fractures are completely displaced. Although the injury is visible on the radiographs, it is more subtle in adults than children. Thus, MRI is helpful in clarifying this injury in adults. Open or arthroscopic reduction and internal fixation is recommended for type II and type III fractures that do not respond to closed reduction. Meyers MH, McKeever FM: Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684. Wiss DA, Watson JT: Fractures of the tibial plateau, in Rockwood CA, Green DP, Bucholz RW, et al (eds): Rockwood and Green's Fractures in Adults. Philadelphia, PA, Lippincott-Raven, 1996, pp 1920-1953.
References:
- Lubowitz JH, Elson WS, Guttmann D: Arthroscopic treatment of tibial plateau fractures: Intercondylar eminence avulsion fractures. Arthroscopy 2005;21:86-92.
Question 22
A 25-year-old man has a mass on the medial aspect of the left knee. He reports that the mass has been present for several years, but a recent increase in physical activity has resulted in periodic tenderness. Radiographs are shown in Figures 13a and 13b. What is the most likely diagnosis?




Explanation
13b The radiographs reveal a sessile lesion projecting from the medial aspect of the distal femur. The lesion shares the cortex with the bone and the base communicates with the medullary space of the femur. This is the classic appearance of an osteochondroma, the most common benign tumor of bone. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
References:
- Parsons TW: Benign bone tumors, in Fitzgerald R Jr, Kaufer H, Malkani A (eds): Orthopaedics. Philadelphia, PA, Mosby International, 2002, pp 1027-1035.
Question 23
A previously asymptomatic 40-year-old man injures his shoulder in a fall. Examination shows that he is unable to lift the hand away from his back while maximally internally rotated. An axial MRI scan of the shoulder is shown in Figure 14. What is the most likely diagnosis?


Explanation
The MRI scan shows detachment of the subscapularis from its insertion on the lesser tuberosity. The examination finding is consistent with a positive lift-off test, also indicating a tear of the subscapularis. Lyons RP, Green A: Subscapularis tendon tears. J Am Acad Orthop Surg 2005;13:353-363.
References:
- Warner JJ, Higgins L, Parsons IM, et al: Diagnosis and treatment of anterosuperior rotator cuff tears. J Shoulder Elbow Surg 2001;10:37-46.
Question 24
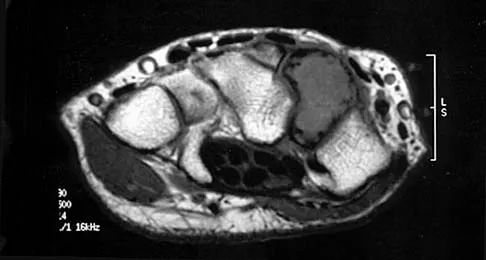
A patient is treated with volar plating for a distal radius fracture. The CT scan shown in Figure 15 is obtained after union of the fracture because the patient reports ongoing symptoms. The prominent hardware is most likely injuring what tendon?


Explanation
Extensor tendon injuries have been reported after volar plating of distal radius fractures. The CT scan shows prominent dorsal hardware a few millimeters ulnar to Lister's tubercle. The second compartment, the ECRL and ECRB, is radial to Lister's tubercle. The ECU runs along the distal ulna. The contents of the fourth dorsal compartment run just ulnar to Lister's tubercle. The EDC tendon is likely irritated in this patient. The EPB runs along the radial border of the radius and is well away from prominent hardware. Benson EC, Decarvalho A, Mikola EA, et al: Two potential causes of EPL rupture after distal radius volar plate fixation. Clin Orthop Relat Res 2006;451:218-222.
References:
- Cooney WP, Linscheid RL, Dobyns JH (eds): The Wrist: Diagnosis and Operative Treatment. Philadelphia, PA, Mosby-Year Book, 1998.
Question 25
A 9-year-old child sustains a proximal tibial physeal fracture with a hyperextension mechanism. What structure is at most risk for serious injury?

Explanation
The most serious injury associated with proximal tibial physeal fracture is vascular trauma. The popliteal artery is tethered by its major branches near the posterior surface of the proximal tibial epiphysis. During tibial physeal displacement, the popliteal artery is susceptible to injury. Injuries to the other structures are less common.
References:
- Beaty JH, Kasser JR: Rockwood and Wilkins Fractures in Children. Philadelphia, PA, JB Lippincott, 2006, p 961.
Finish Exam?
You cannot change answers after submitting.
You Might Also Like


Previous ChapterOrthopedic Sports Medicine 2026 MCQs: Board Review Question…
Next Chapter Orthopedic Anatomy 2026 MCQs: Board Review Questions & Answ…

Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon