Operative Management of Clavicle and Humeral Nonunions: A Comprehensive Surgical Guide
Key Takeaway
The operative management of clavicle and humeral nonunions requires meticulous surgical technique, rigid internal fixation, and biological optimization. This guide details evidence-based approaches for plate fixation and bone grafting of the clavicle, alongside advanced reconstruction strategies for proximal and diaphyseal humeral nonunions. Key considerations include biomechanical plate positioning, management of osteoporotic bone with locking technology, and the strategic use of structural allografts or arthroplasty in complex salvage scenarios.
INTRODUCTION TO UPPER EXTREMITY NONUNIONS
The management of nonunions in the shoulder girdle and humerus presents a formidable challenge to the orthopedic surgeon. Successful salvage requires a profound understanding of local pathoanatomy, meticulous soft-tissue handling, rigid biomechanical fixation, and the optimization of the biological environment. This masterclass delineates the evidence-based surgical techniques for addressing nonunions of the clavicle, proximal humerus, and humeral shaft, integrating classical principles with contemporary advancements in locking plate technology and arthroplasty.
PLATE FIXATION AND BONE GRAFTING OF THE CLAVICLE
Clavicular nonunions typically occur following conservative management of severely displaced midshaft fractures, particularly those with significant comminution, initial shortening greater than 2 centimeters, or soft tissue interposition. Symptomatic nonunions—characterized by pain, crepitus, and shoulder girdle dysfunction—warrant operative intervention. The gold standard remains open reduction, rigid internal fixation, and autogenous bone grafting.
Biomechanical Considerations and Plate Positioning
The clavicle acts as a strut connecting the axial skeleton to the upper extremity, subjecting it to complex bending, torsional, and axial loads. While superior plating acts as a tension band against the gravitational pull of the arm, anteroinferior plating offers distinct anatomical and biomechanical advantages in the setting of nonunion.
Surgical Pearl: Anteroinferior Plating
Placing the plate on the anteroinferior surface allows the surgeon to direct the drill bits and screws in a superoposterior direction. This trajectory safely directs instrumentation away from the vital subclavicular structures, including the subclavian vein, subclavian artery, and the brachial plexus. Furthermore, anteroinferior plates are less prominent beneath the skin, reducing postoperative hardware irritation.
Surgical Technique: Step-by-Step
- Patient Positioning and Preparation:
Place the patient in the beach-chair position with a small bump between the scapulae to allow the shoulder girdle to fall posteriorly, aiding in the restoration of clavicular length. Ensure the ipsilateral iliac crest is prepped and draped for autogenous bone graft harvesting. - Surgical Approach:
Make an incision parallel with and just distal to the clavicle. This infraclavicular approach avoids placing the scar directly over the hardware, minimizing wound breakdown. - Dissection and Exposure:
Incise the platysma and carefully identify and protect the supraclavicular nerve branches to prevent postoperative chest wall numbness or painful neuromas. Incise the periosteum and meticulously strip it from the anterior and inferior aspects of the bone. Preserve the superior and posterior periosteal attachments to maintain residual vascularity. - Preparation of the Nonunion Site:
Exsect all intervening fibrous tissue. Use a high-speed burr or osteotome to open the sclerotic medullary canals of both the medial and lateral fragments until punctate bleeding (the "paprika sign") is observed, ensuring a viable biological bed. - Plate Fixation:
Reduce the fracture, restoring anatomical length and rotation. Apply a four-hole or six-hole 3.5-mm dynamic compression plate (DCP), a contoured 3.5-mm reconstruction plate, or a modern low-profile, clavicle-specific locking plate to the anteroinferior surface. Ensure at least three bicortical screws (six cortices) are achieved on each side of the nonunion. - Bone Grafting:
Harvest autogenous cancellous bone from the anterior iliac crest. Pack the graft densely around the nonunion site, particularly filling any inferior or posterior cortical defects. - Closure:
Close the clavipectoral fascia and platysma meticulously over the plate to provide a robust soft-tissue envelope. Close the skin with subcuticular sutures.
Postoperative Care
A shoulder immobilizer is worn for 1 to 2 weeks to protect the soft tissue repair. Gentle active and pendulum exercises are initiated immediately to maintain shoulder mobility and prevent adhesive capsulitis. Active-assisted range of motion is progressed at 2 to 4 weeks, with full resistance exercises delayed until radiographic evidence of bridging callus is observed, typically at 8 to 12 weeks.
MANAGEMENT OF PROXIMAL HUMERUS NONUNIONS
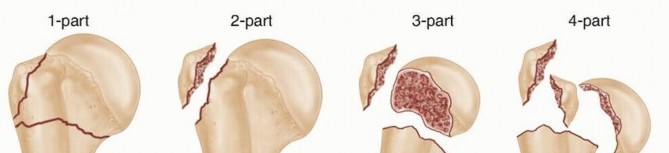
Nonunions of the proximal humerus most frequently manifest as two-part fractures at the surgical neck. According to Crosby et al., a nonunion of the proximal humerus is defined clinically and radiographically when there is an absolute cessation of healing at 3 months from the time of injury. The management algorithm is dictated by the patient's age, bone quality, rotator cuff integrity, and the specific pathoanatomy of the nonunion (atrophic, hypertrophic, or oligotrophic).
Open Reduction and Internal Fixation (ORIF)
In physiologically younger patients with adequate bone stock, joint preservation is the primary goal. Healy et al. demonstrated that the best outcomes are achieved with rigid internal fixation combined with cancellous bone grafting.
The Tension Band and Screw Construct
Historically, Healy recommended a tension band construction. This technique involves passing heavy non-absorbable sutures or wire through the rotator cuff insertions and securing them to the distal shaft fragment. This neutralizes the deforming forces of the rotator cuff, while two or three cancellous screws are placed into the proximal fragment to achieve interfragmentary compression.
Advanced Locking Plate Technology
In contemporary practice, locking plates have revolutionized the treatment of proximal humeral nonunions, particularly in osteoporotic bone.
Biomechanical Advantage of Locking Plates
The locking plate is superior to traditional non-locking plates because it functions as a fixed-angle construct. It features a lower profile, demonstrates significantly higher torsional strength and stiffness, and allows for multiple divergent proximal screw placements. This divergent trajectory maximizes purchase in the subchondral bone of the humeral head, which is often the only region of dense bone remaining in osteoporotic patients.
For hypertrophic and oligotrophic nonunions, locking plates augmented with intramedullary fibular allografts provide exceptional structural stability. The allograft acts as an internal strut, preventing varus collapse and enhancing screw purchase. For atrophic nonunions, the addition of autogenous iliac crest bone graft is mandatory to provide the necessary osteoinductive and osteogenic factors.
Arthroplasty for Proximal Humerus Nonunions
When joint preservation is impossible—due to severe osteopenia, avascular necrosis of the humeral head, or massive articular destruction—shoulder arthroplasty becomes the treatment of choice. While arthroplasty provides significant reduction in pain and improves motion, patients must be counseled that functional outcomes are generally less satisfying than when the procedure is performed for primary glenohumeral osteoarthritis.
Hemiarthroplasty
Nonunited fractures or fracture-dislocations at the anatomical neck of the humerus, where the articular segment is devascularized, can be treated by open reduction and the insertion of a prosthesis through the head fragment.
Figure A: Preoperative appearance on admission demonstrating a complex four-part fracture-dislocation with an ununited fracture at the anatomical neck of the humerus.
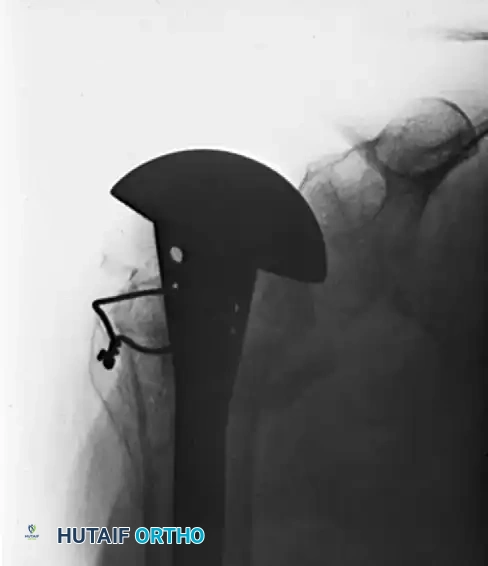
The Neer I prosthesis (hemiarthroplasty) relies heavily on the anatomical healing of the greater and lesser tuberosities around the implant to restore rotator cuff function. Meticulous tuberosity mobilization, heavy suture fixation through the prosthesis fin, and securement to the humeral shaft are critical steps.

Figure B: Solid union and stable fixation 6 months postoperatively following reconstruction with a Neer I prosthesis, yielding satisfactory clinical function.
Reverse Total Shoulder Arthroplasty (RTSA)
In the low-demand elderly patient with a functional deltoid, poor tuberosity bone stock, or concurrent rotator cuff arthropathy, Reverse Total Shoulder Arthroplasty (RTSA) has emerged as a highly successful salvage procedure. By medializing the center of rotation and increasing the deltoid moment arm, RTSA bypasses the need for a functioning rotator cuff or healed tuberosities, offering superior and more predictable forward elevation compared to hemiarthroplasty in the salvage setting.
MANAGEMENT OF HUMERAL SHAFT NONUNIONS
Nonunions occur in approximately 10% of patients with humeral shaft fractures, regardless of the initial modality of treatment. The humerus is uniquely susceptible to nonunion because the arm acts as a long lever arm, making fracture site motion notoriously difficult to control with external splintage alone.
Etiology and Risk Factors
Nonunion is most prevalent in the mid and proximal diaphysis, particularly with spiral or oblique fracture patterns. The etiology is multifactorial:
* Mechanical Factors: Distraction, overriding of fragments, or inadequate immobilization.
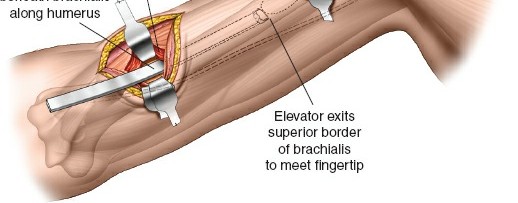
* Biological Factors: Soft tissue interposition (frequently the brachialis or biceps muscle), severe bone loss, or disrupted blood supply secondary to high-energy comminution.
Patient Selection and Conservative Management
The type of nonunion, alongside the age and comorbidities of the patient, must heavily influence treatment decisions. In most patients, operative treatment is strictly indicated to correct angular deformity, eliminate pain, and regain upper extremity function.
Clinical Pitfall: The Elderly Patient
In elderly, low-demand patients with severe osteoporotic bone and multiple medical comorbidities, the diminished function caused by a painless pseudarthrosis may be preferable to the significant risks of open reduction and internal fixation. In such cases, the use of a custom-molded, lightweight functional orthosis (Sarmiento brace) may allow sufficient activities of daily living to avoid further surgical intervention.
Surgical Technique: Compression Plating and Bone Grafting
For the vast majority of humeral diaphyseal nonunions, the gold standard treatment is open reduction, autogenous bone grafting, and dynamic compression plating. This approach yields an up to 98% union rate in the literature.
- Surgical Approach:
Depending on the level of the nonunion, an anterolateral or posterior approach is utilized. The posterior approach is highly favored for mid-to-distal third nonunions as it provides an expansive, flat surface for plate application. - Radial Nerve Management:
The radial nerve must be meticulously identified, neurolysed, and protected throughout the procedure. In the posterior approach, the nerve is mobilized from the spiral groove and gently retracted with vessel loops. - Biological Preparation:
Radical excision of all fibrous pseudarthrosis tissue is mandatory. The sclerotic bone ends must be freshened with a rongeur or burr until healthy, bleeding bone is encountered. The medullary canal must be recanalized bilaterally. - Fixation Strategy:
A 4.5-mm broad dynamic compression plate (LC-DCP) or a 4.5-mm locking compression plate is applied. The plate must be long enough to achieve a minimum of eight cortices of fixation proximal and distal to the nonunion. Interfragmentary compression is achieved using an articulated tension device or eccentrically placed screws. - Structural Augmentation:
In cases of atrophic nonunion with significant cortical defects or severe osteoporosis, the use of an intramedullary fibular allograft is highly recommended. The fibula is impacted into the canal, and screws are passed through the plate, the near cortex, the fibular strut, and the far cortex. This dramatically improves construct stability and enhances the rate of union.
The Role of Intramedullary Nailing
While primary intramedullary (IM) nailing of acute humeral shaft fractures is a well-established technique, its role in the treatment of nonunions is nuanced. IM nailing of a humeral nonunion that was initially treated non-operatively can be successful, provided the canal is over-reamed and the nonunion site is biologically stimulated.
However, exchange nailing—the process of removing an existing IM nail, reaming the canal larger, and inserting a larger diameter nail—has not proven to be as successful in the humerus as it is in the weight-bearing femur or tibia. The humerus lacks the axial compressive forces of gait that stimulate healing in lower extremity exchange nailing. Furthermore, IM nailing does not reliably control rotational forces at the nonunion site as effectively as broad compression plating. Therefore, for nonunions following failed IM nailing, the preferred salvage strategy is nail removal, open debridement, compression plating, and copious autogenous bone grafting.
You Might Also Like