Achieve Stable Fixation: Tension Band Sutures for Humeral Fractures
Key Takeaway
This article provides essential research regarding Achieve Stable Fixation: Tension Band Sutures for Humeral Fractures. Tension band sutures are a fixation technique for proximal humeral fractures, especially beneficial for patients with osteoporosis or comminution. They offer secure stabilization by being placed through strong tendon insertion sites, which are often more robust than osteoporotic bone. This method allows for optimal stabilization of fragmented fractures, enhancing healing and improving patient outcomes.
Achieve Stable Fixation Tension Band Sutures for Humeral Fractures
Introduction and Epidemiology
Proximal humeral fractures represent a significant burden on orthopedic trauma services, accounting for approximately 5-6% of all fractures and ranking as the third most common fracture in individuals over 65 years of age, following hip and distal radius fractures. While the majority are managed non-operatively, surgical intervention is indicated for displaced or unstable fracture patterns to restore anatomy and facilitate early functional recovery. Among these, isolated greater tuberosity (GT) fractures, especially those displaced, warrant particular attention due to their propensity for impingement and functional compromise if left untreated.
Greater tuberosity fractures most commonly result from high-energy trauma in younger patients, often associated with shoulder dislocations, or from low-energy falls in osteoporotic elderly individuals. Anatomical reduction and stable internal fixation are critical, as the GT serves as the insertion site for the supraspinatus, infraspinatus, and teres minor tendons, essential components of the rotator cuff. Displacement of the GT fragment, typically superomedial due to unopposed rotator cuff pull, can lead to impingement on the coracoacromial arch, causing significant pain, restricted motion, and long-term functional deficits, including rotator cuff dysfunction and osteoarthritis.
Tension band fixation, a biomechanically sound principle, converts tensile forces into compressive forces at the fracture site, thereby promoting union and stability. While traditionally applied with wires, modern surgical techniques often utilize high-strength non-absorbable sutures for tension banding, particularly for metaphyseal fractures and avulsion injuries where bone stock may be limited or where the surrounding soft tissue envelope can be incorporated into the repair construct. For displaced greater tuberosity fractures, tension band sutures offer a robust, load-sharing fixation method that can withstand rotator cuff forces, allowing for early rehabilitation and minimizing hardware-related complications associated with plate and screw constructs in this anatomically complex region. This comprehensive review will delve into the principles, techniques, and outcomes of tension band suture fixation for humeral fractures, with a primary focus on the greater tuberosity.
Surgical Anatomy and Biomechanics
Humeral Surgical Anatomy
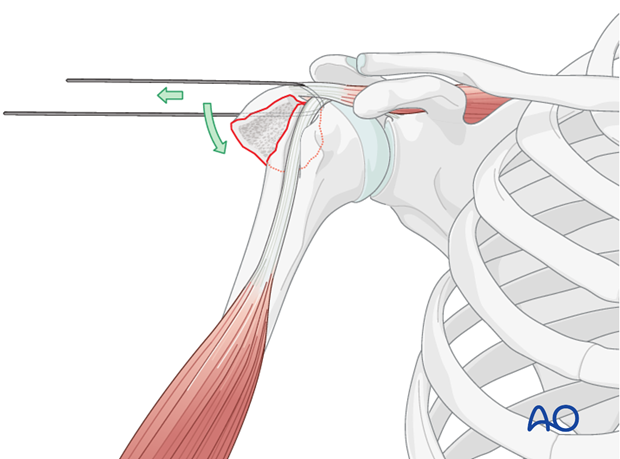
The proximal humerus is a complex anatomical region comprising the humeral head, anatomical neck, surgical neck, greater tuberosity, and lesser tuberosity. The greater tuberosity, located laterally, serves as the insertion point for three of the four rotator cuff tendons: the supraspinatus (superior facet), infraspinatus (middle facet), and teres minor (inferior facet). The lesser tuberosity, anteriorly, is the insertion site for the subscapularis. These muscular attachments exert significant forces, particularly the supraspinatus and infraspinatus, which can cause superior and posterior displacement of greater tuberosity fragments upon fracture.
Critical neurovascular structures around the proximal humerus include the axillary nerve, which courses around the surgical neck, typically 5-7 cm distal to the acromion, and the anterior and posterior circumflex humeral arteries, which provide the primary blood supply to the humeral head. Surgical approaches must meticulously protect these structures. The deltoid muscle, which provides shoulder contour and abduction, is intimately associated with the greater tuberosity and must be carefully managed during exposure.
Biomechanics of Greater Tuberosity Fractures
Fractures of the greater tuberosity typically occur from direct trauma or indirectly through avulsion by the strong traction forces of the rotator cuff, often during a fall onto an outstretched arm with the shoulder abducted and externally rotated, or during an anterior shoulder dislocation. The unresisted pull of the rotator cuff muscles, particularly the supraspinatus, leads to characteristic superior and posterior displacement of the fragment. A displacement of greater than 5 mm, or greater than 3 mm for an associated dislocation, is generally considered significant due to its potential to impinge on the coracoacromial arch and cause mechanical block to motion.
The primary biomechanical goal of fixation for greater tuberosity fractures is to neutralize the tensile forces exerted by the rotator cuff, thereby converting them into compressive forces across the fracture site. This allows for stable healing and minimizes impingement.
Tension Band Principle
The tension band principle is a biomechanical concept that converts tensile stress into compressive stress. In the context of bone fixation, it involves placing a fixation device (e.g., wire, suture) on the tension side of a bone or fragment, which is then resisted by a compression side (often the bone itself or a plate). When a functional load is applied, the tension band resists distraction and pulls the fracture fragments together, generating interfragmentary compression.
For greater tuberosity fractures, the rotator cuff muscles apply tensile forces to the tuberosity fragment. A tension band suture, passed through the greater tuberosity and anchored securely in the humeral shaft (or via suture anchors), creates a construct that resists this tensile pull. As the rotator cuff attempts to displace the fragment, the tension band tightens, compressing the fragment against the humeral head. This dynamic compression promotes biological healing and provides enough stability for early controlled mobilization, preventing fragment migration and impingement. The sutures act as dynamic internal splints, sharing the load with the healing bone.
Indications and Contraindications
Surgical intervention for proximal humeral fractures, particularly greater tuberosity fractures, is guided by a meticulous assessment of fracture morphology, patient factors, and the potential for long-term functional impairment.
Indications for Operative Fixation
The primary indications for operative fixation of greater tuberosity fractures are based on the degree of displacement and angulation, which dictate the risk of impingement, nonunion, and rotator cuff dysfunction.
- Displacement: A displacement of the greater tuberosity fragment exceeding 5 mm in any plane (superior, posterior, or medial) is generally considered a primary indication for surgical reduction and fixation. For fractures associated with shoulder dislocation, a displacement of 3 mm or more is often considered significant due to the already compromised soft tissue envelope and potential for recurrent instability.
- Angulation: Significant angulation of the fragment can also lead to impingement.
- Rotational Malalignment: Rotational displacement can disrupt the biomechanics of the rotator cuff insertion and lead to functional deficits.
- Associated Injuries: Greater tuberosity fractures frequently accompany anterior shoulder dislocations. If the tuberosity fragment fails to reduce spontaneously with the humeral head, or if it remains significantly displaced after reduction of the dislocation, operative intervention is warranted to prevent recurrent instability and chronic impingement. Concomitant rotator cuff tears requiring repair may also influence the decision towards operative management of the fracture.
- Functional Impingement: Even with lesser displacement, if clinical examination or diagnostic imaging demonstrates clear impingement on the coracoacromial arch or glenoid, leading to pain and limited range of motion, operative intervention may be considered.
- Acute Rotator Cuff Avulsion: In younger, active patients, a significantly displaced GT fracture can be treated akin to an acute rotator cuff avulsion, requiring robust repair to restore function.
Contraindications for Operative Fixation
While operative fixation is beneficial for specific indications, certain factors may contraindicate surgical intervention, favoring non-operative management or alternative treatment strategies.
- Minimal or Non-Displaced Fractures: Fractures with less than 5 mm displacement, no significant angulation, and no evidence of impingement are typically managed non-operatively with immobilization and early rehabilitation.
- Severely Comminuted Fragments: In cases of severe comminution of the greater tuberosity where a stable fixation construct cannot be achieved with sutures or screws, attempting internal fixation may be futile. However, if the main fragment is large enough, tension banding can still be effective.
- Poor Bone Quality (Severe Osteoporosis): While tension band sutures can sometimes be more forgiving than screws in osteoporotic bone by dispersing forces over a larger area (especially with suture anchors), extremely poor bone stock may preclude stable fixation, increasing the risk of suture pull-through or construct failure.
- Significant Comorbidities and High Surgical Risk: Patients with multiple severe comorbidities (e.g., uncontrolled cardiac disease, severe pulmonary disease, active malignancy) that significantly increase the risk of anesthesia and surgery may be better managed non-operatively.
- Active Infection: Absolute contraindication to elective internal fixation.
- Soft Tissue Compromise: Extensive soft tissue injury, open wounds, or compromised skin integrity over the surgical site may preclude immediate open reduction and internal fixation.
- Patient Compliance: Patients who are unwilling or unable to comply with the necessary post-operative rehabilitation protocol may have suboptimal outcomes following operative fixation.
Operative Versus Non-Operative Indications
| Feature / Indication | Operative Management | Non-Operative Management |
|---|---|---|
| Displacement (Isolated GT) | > 5 mm in any plane (superior, posterior, medial) | < 5 mm displacement |
| Displacement (with Dislocation) | > 3 mm displacement after reduction of dislocation | < 3 mm displacement after reduction of dislocation, spontaneously reduced |
| Angulation / Rotation | Significant angulation or rotational malalignment causing impingement | Minimal angulation or rotation, no impingement |
| Associated Injuries | Irreducible fracture-dislocation; significant concomitant rotator cuff pathology requiring repair | No associated shoulder dislocation; isolated, stable GT fracture |
| Functional Impingement | Clinical or radiographic evidence of mechanical impingement and pain | Absence of impingement symptoms |
| Patient Demographics | Younger, active patients; physiologically fit elderly patients with good bone quality | Elderly patients with low functional demands; patients with significant surgical contraindications |
| Bone Quality | Adequate bone stock for stable fixation | Severe osteoporosis precluding stable fixation |
| Comminution | Manageable comminution with a primary load-bearing fragment | Severe comminution where no reconstructable fragment exists |
| Soft Tissue Envelope | Intact and healthy | Significant compromise (e.g., severe open injury) |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is paramount for successful outcomes in the operative management of greater tuberosity fractures. This involves comprehensive imaging review, meticulous patient assessment, and precise intraoperative setup.
Imaging Assessment
- Standard Radiographs: An initial series including true anteroposterior (AP) (Grashey view), scapular Y-view, and axillary lateral views of the shoulder is essential. These views help characterize the fracture pattern, degree of displacement, and angulation. Specific attention should be paid to the superior and posterior displacement of the greater tuberosity fragment.
- Computed Tomography (CT) Scan: A CT scan with 3D reconstructions is highly recommended, especially for complex or comminuted fractures, or when there is suspicion of articular involvement. CT provides detailed information regarding fragment size, comminution, and precise displacement, which is invaluable for surgical planning. It can also help identify potential incarceration of the biceps tendon within the fracture site.
- Magnetic Resonance Imaging (MRI): While not routinely required, MRI may be considered if there is suspicion of concomitant rotator cuff tears or other soft tissue injuries that could influence the surgical approach or repair strategy. It can also differentiate between bony avulsion and primary tendon tear.
Patient Preparation
A comprehensive medical workup is performed to assess the patient's overall health status and optimize them for surgery. This includes a thorough history and physical examination, laboratory tests, and an electrocardiogram. Co-morbidities are managed appropriately, and a pre-anesthetic consultation is conducted.
Informed consent is obtained, detailing the surgical procedure, potential risks (e.g., infection, neurovascular injury, nonunion, hardware failure, stiffness), and expected post-operative course.
Patient Positioning
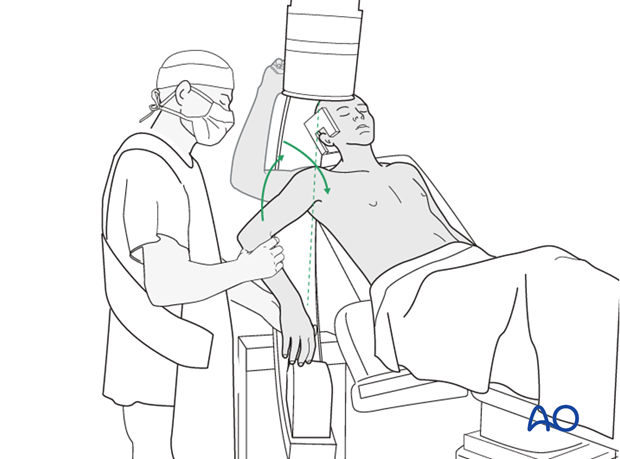
The choice of patient position significantly impacts surgical exposure and surgeon comfort. For greater tuberosity fractures, the beach chair position is generally preferred.
-
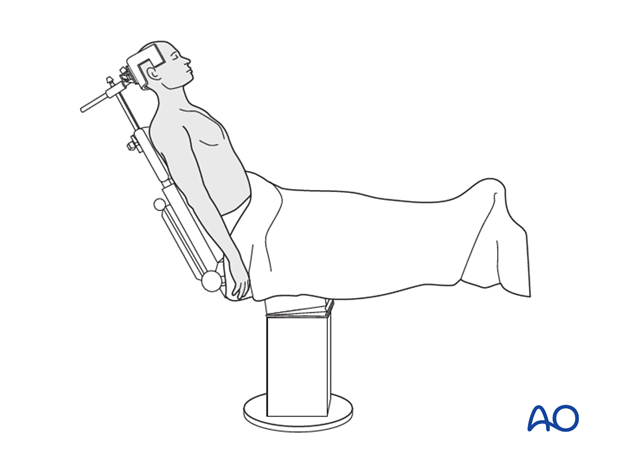
Beach Chair Position:
- The patient is positioned supine on the operating table, and the table is then flexed to raise the torso to approximately 30-45 degrees, similar to a beach chair.
- The head is secured in a well-padded headrest, ensuring the cervical spine is in a neutral position.
- Padding is applied to all pressure points, particularly the sacrum, heels, and elbows, to prevent nerve compression or skin breakdown.
- The affected arm is draped free to allow for full range of motion intraoperatively, crucial for reduction maneuvers and assessing implant stability.
- The advantages of the beach chair position include improved visualization of the anterior and lateral aspects of the shoulder, easier access to the axilla for neurovascular protection, and the ability to convert to an arthroscopic procedure if necessary.
- It also allows the surgeon to operate in a more ergonomic position.
- Potential disadvantages include the risk of cerebral hypoperfusion (though rare with appropriate blood pressure monitoring) and venous air embolism.
-
Supine Position: While less common for routine greater tuberosity fixation, a supine position with a bolster under the ipsilateral scapula can also be used. This provides a stable base but may limit some aspects of exposure compared to the beach chair position.
- Lateral Decubitus Position: This position is more frequently used for arthroscopic shoulder procedures but can be adapted for open cases. The patient lies on their contralateral side, secured with beanbags and bolsters. The arm is often suspended in traction. While providing excellent posterior access, anterior exposure can be more challenging.
Regardless of the chosen position, ensuring adequate padding, securing the patient appropriately, and maintaining physiological parameters are paramount for patient safety and surgical efficacy.
Detailed Surgical Approach and Technique
The surgical approach to the greater tuberosity must provide adequate visualization for reduction and fixation while minimizing iatrogenic damage to surrounding soft tissues and neurovascular structures.
Surgical Approaches
Two main approaches are commonly utilized:
-
Anterolateral Approach (Deltopectoral): This is a versatile approach for many proximal humeral fractures.
- Incision: A curvilinear incision is made from the coracoid process inferiorly along the deltopectoral groove for approximately 8-10 cm.
- Internervous Plane: The deltopectoral groove lies between the deltoid muscle (innervated by the axillary nerve) laterally and the pectoralis major muscle (innervated by the medial and lateral pectoral nerves) medially. This provides a true internervous plane.
- Dissection: The cephalic vein, which lies within the groove, is identified and protected, typically retracted medially with the pectoralis major. The clavipectoral fascia is incised, exposing the underlying conjoined tendon and subscapularis. The anterior deltoid is elevated from its insertion on the humerus if necessary, or a partial deltoid split may be performed distally, with caution to protect the axillary nerve, which is generally 5-7 cm from the acromion. For greater tuberosity fractures, the approach may need to extend more laterally over the deltoid to gain direct access.
-
Transdeltoid Lateral Approach: This approach offers more direct access to the greater tuberosity.
- Incision: A straight longitudinal incision is made over the lateral aspect of the deltoid, centered over the greater tuberosity.
- Dissection: The deltoid muscle fibers are split bluntly in line with their fibers. Care must be taken to avoid exceeding 5 cm distal to the acromion to protect the axillary nerve. A small deltoid split is usually sufficient for GT fractures.
- Advantages: Direct visualization of the GT, minimal dissection of other structures.
- Disadvantages: Risk of iatrogenic injury to the axillary nerve if the split extends too distally or if traction is excessive.
The choice between approaches depends on the specific fracture pattern and surgeon preference. For isolated greater tuberosity fractures, a transdeltoid approach is often preferred due to its directness.
Fracture Reduction and Preliminary Fixation
Once the fracture site is exposed, the following steps are crucial:
-
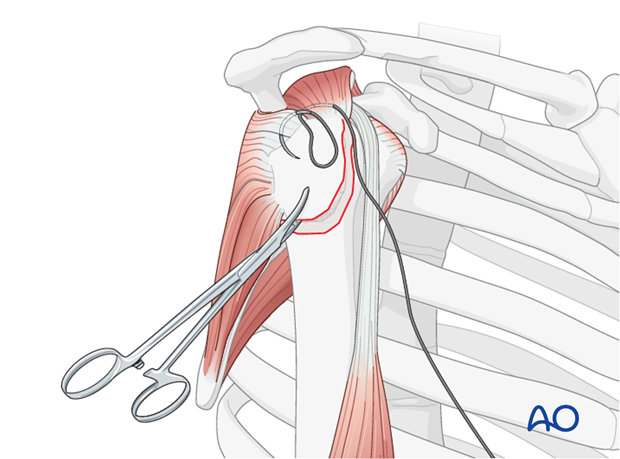
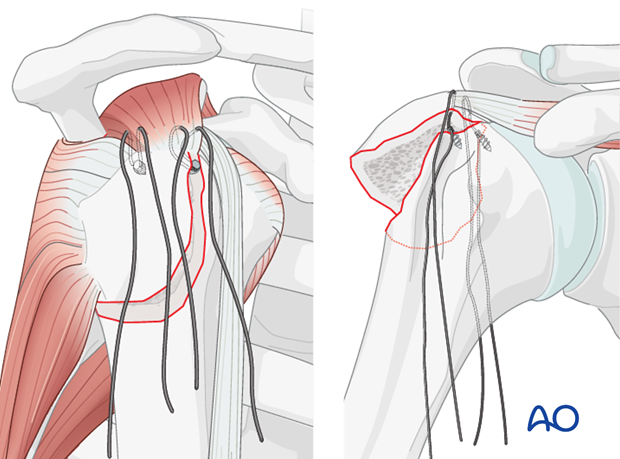
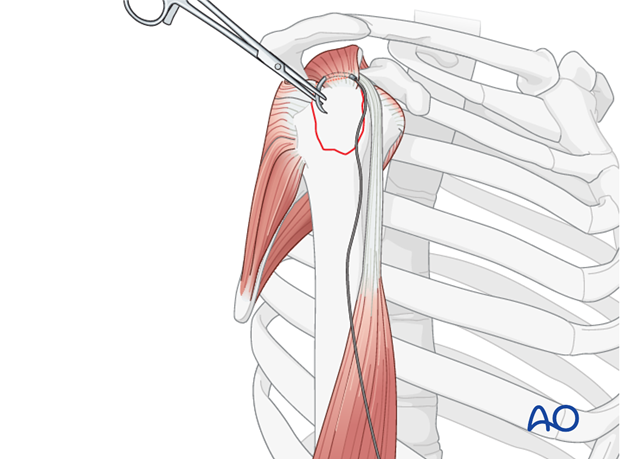
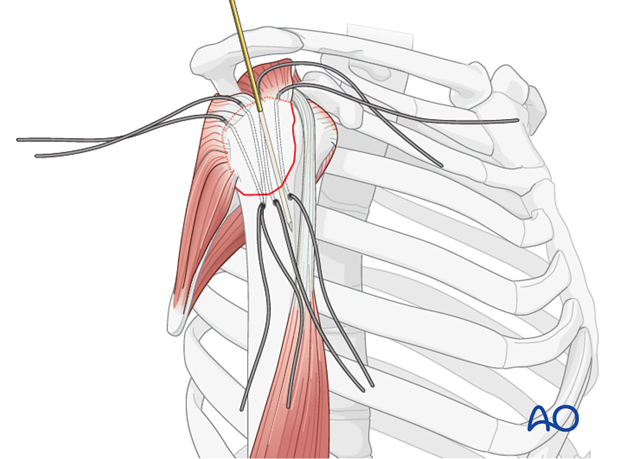
Stay Sutures: Insert strong, non-absorbable stay sutures (e.g., #2 FiberWire or Ethibond) through the rotator cuff tendons attached to the greater tuberosity fragment. Typically, sutures are placed through the supraspinatus and, if necessary, the infraspinatus tendons. These sutures act as "joy-sticks" to manipulate the fragment.
 -
Cleaning the Fracture Bed: Carefully clean the fracture bed, removing any hematoma, loose bone fragments, or soft tissue interposition (e.g., incarcerated biceps tendon). Prepare the margins of the fracture by gently reflecting the periosteum 2-3 mm back from the fracture line to ensure bone-to-bone contact. Avoid aggressive stripping to preserve vascularity.
 -
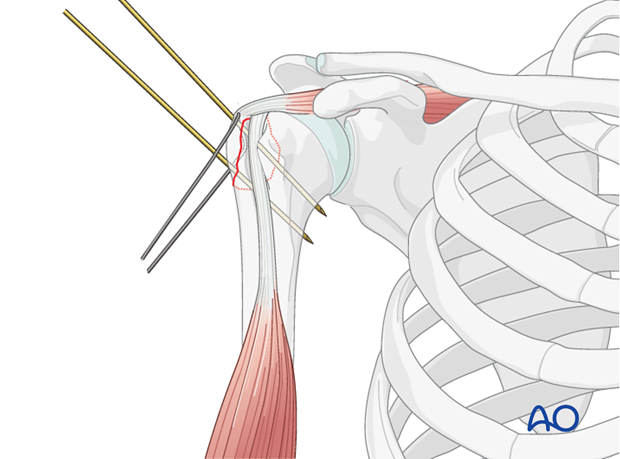
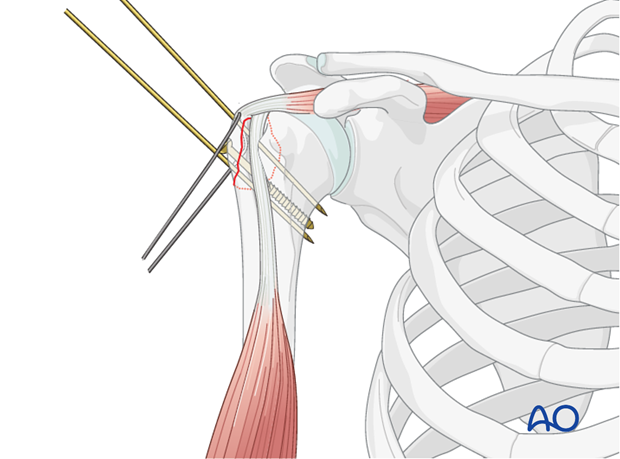
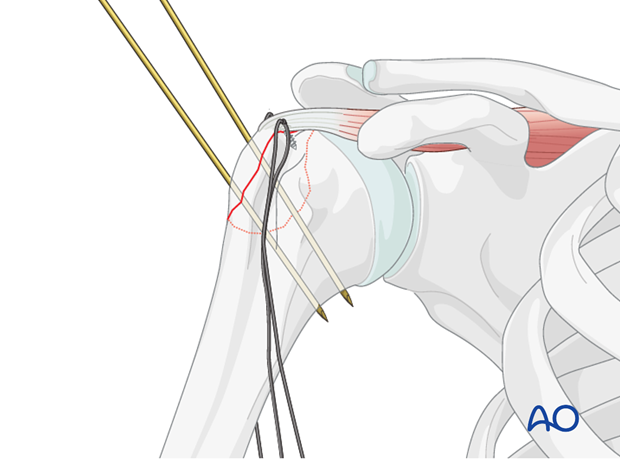
Reduction: Reduce the greater tuberosity fragment anatomically to its bed on the humeral head. This is achieved by pulling on the stay sutures, often combined with gentle manipulation of the humeral head (traction, rotation, adduction) to align the fracture surfaces. Ensure complete anatomical reduction, checking for any remaining displacement or malrotation. Provisional fixation with K-wires may be used to maintain reduction during definitive fixation.
Tension Band Suture Fixation Technique
The goal of tension band suture fixation is to convert tensile forces from the rotator cuff into compressive forces across the fracture site. Several configurations exist, but the core principle remains consistent.
-
Preparation of Humeral Tunnels/Anchor Sites:
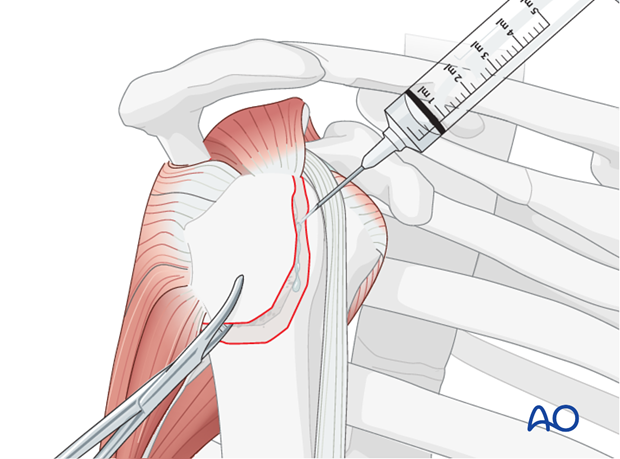
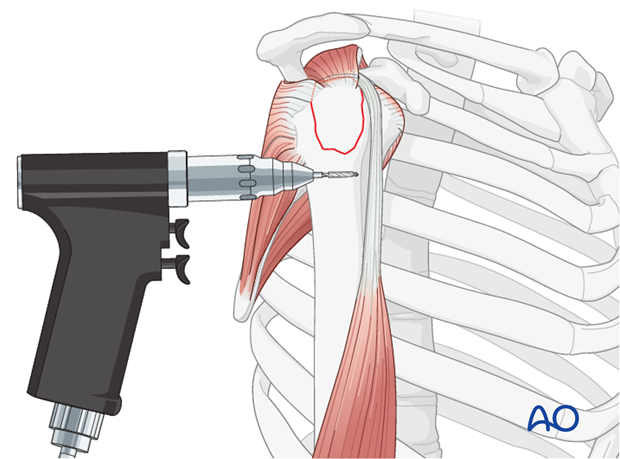
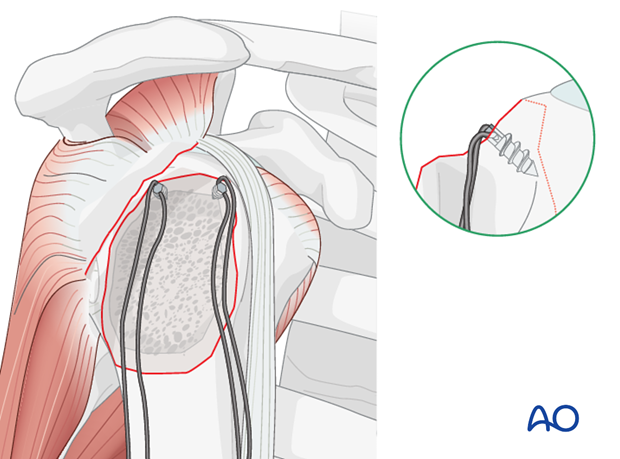
- For transosseous tension banding, two small drill holes (typically 2.0-2.5 mm) are created in the lateral cortex of the humeral shaft, distal to the fracture site and approximately 2-3 cm apart. These holes should be positioned to allow the sutures to exit proximally near the fracture site in an appropriate tensioning direction. A suture passer can then be used to retrieve sutures from the humeral head side, out through the distal cortex.
- Alternatively, and often preferred for better bone purchase in the metaphysis, suture anchors can be placed in the posterolateral aspect of the humeral head. Typically, two to three anchors (e.g., 5.0 mm push-in or screw-in type) are placed distally and medially to the fracture, ensuring sufficient bone stock and avoiding the articular surface. The choice depends on bone quality and surgeon preference.
-
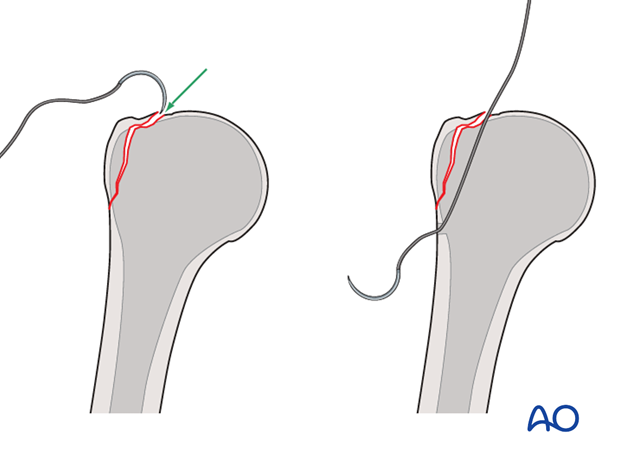
Suture Placement through Greater Tuberosity Fragment:
- Using a small curved awl or drill, two to three transosseous tunnels are created through the greater tuberosity fragment itself. These tunnels should be placed robustly to avoid fragmenting the bone, especially in osteoporotic patients.
- Alternatively, the stay sutures initially placed for reduction can be used as the definitive fixation sutures, passed appropriately through the fragment and then to the humeral shaft.
-
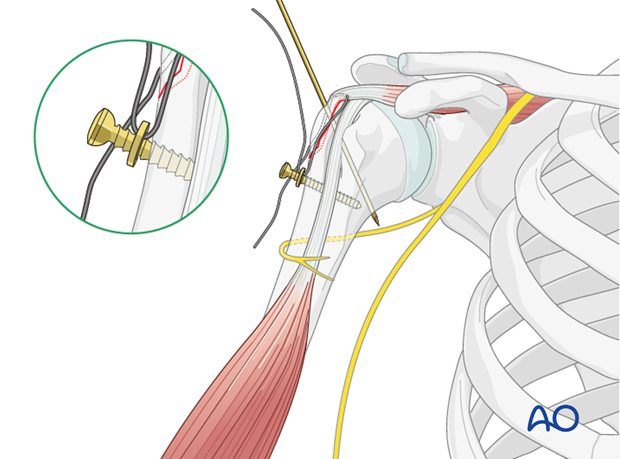
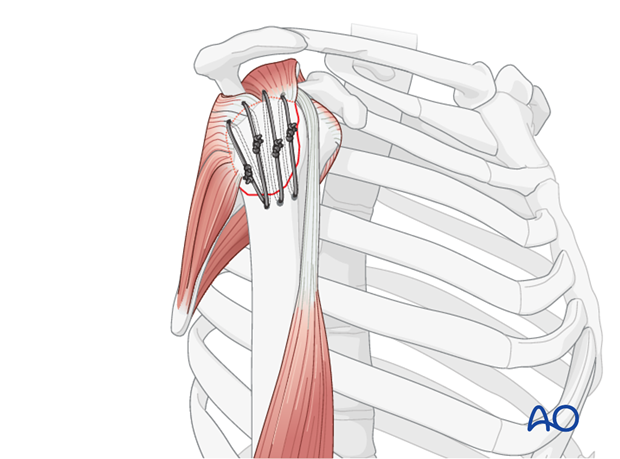
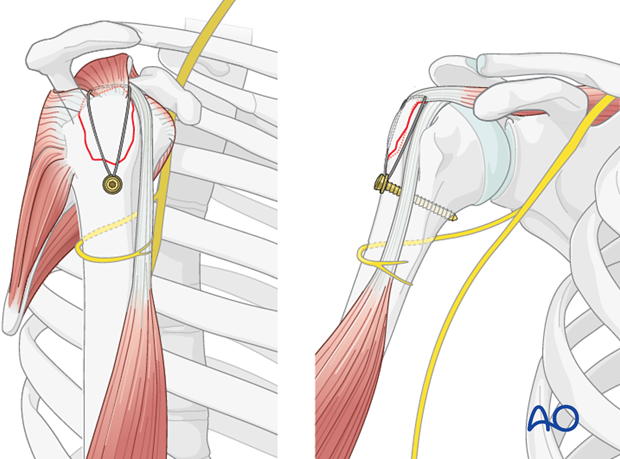
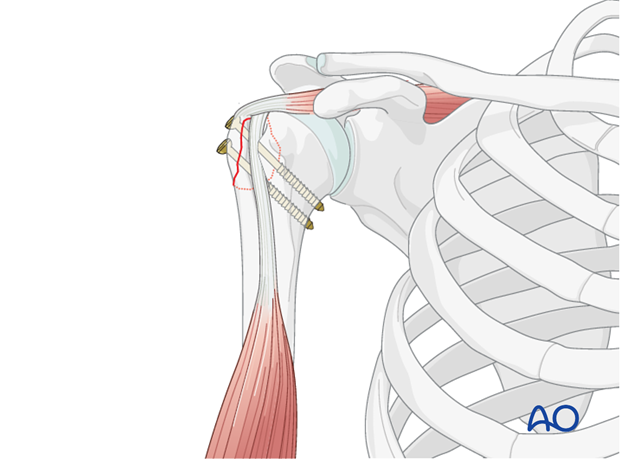
Suture Configuration and Tensioning:
- Figure-of-Eight Tension Band: This is a common and robust method. The non-absorbable suture (e.g., #5 Ethibond, #2 FiberWire, or similar high-strength braided suture) is passed through the greater tuberosity fragment, then distally through the humeral shaft tunnels (or through the eyelets of suture anchors), and finally tied over the lateral cortex of the humeral shaft or around the anchors. This creates a figure-of-eight loop that compresses the fragment onto the humeral head.
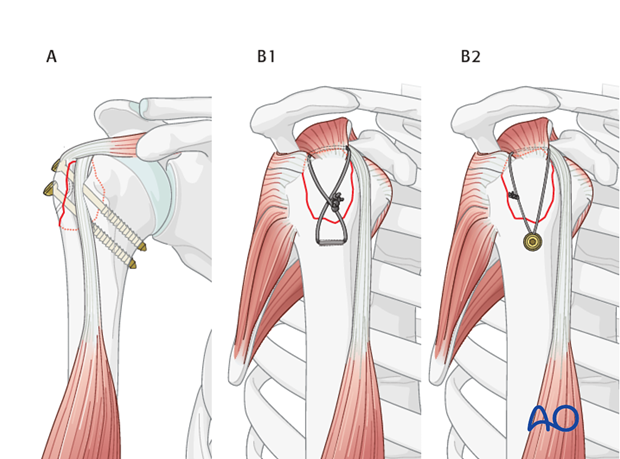

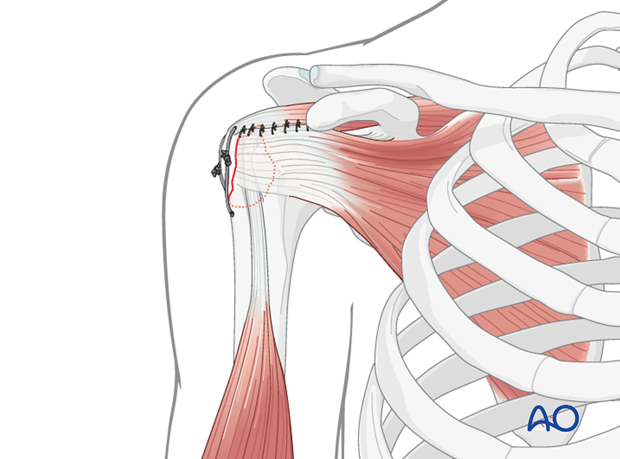 - Single Loop or Multiple Suture Fixation: Depending on the fracture pattern and number of fragments, multiple individual sutures can be passed, each providing localized compression. These can also be passed through the rotator cuff tendons themselves and then anchored to the humeral shaft, effectively repairing the cuff while fixing the fracture. This technique may be particularly useful when the fracture is more of an avulsion of the tendon insertion with a small bone fragment.
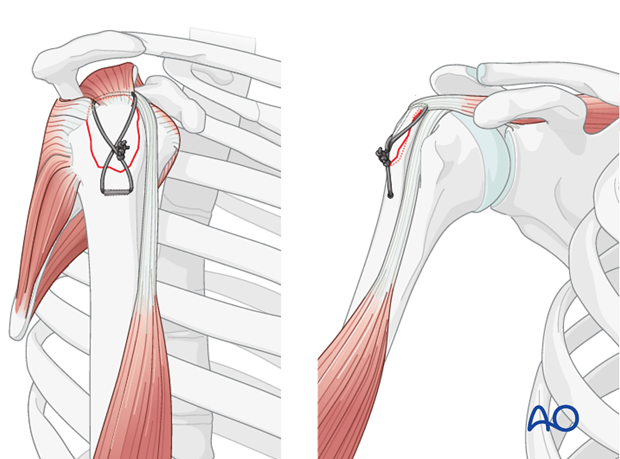
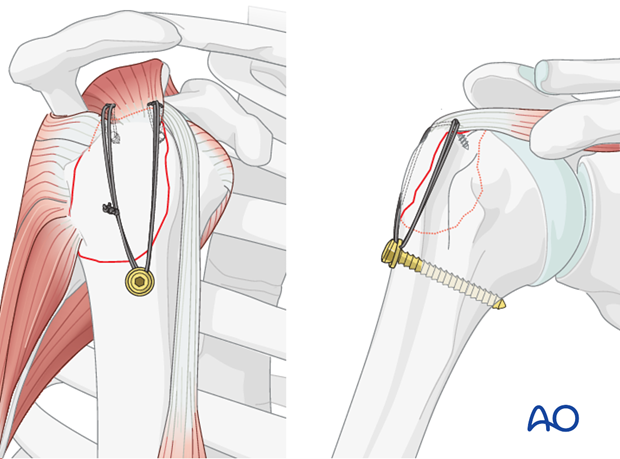 - Tensioning: The sutures are then progressively tightened to achieve firm compression across the fracture site. This step is critical; inadequate tensioning will lead to insufficient compression and potential failure, while excessive tensioning can cut through soft bone. The reduction should be held with K-wires during this process. Knot tying should be secure with multiple throws to prevent slippage.
- Figure-of-Eight Tension Band: This is a common and robust method. The non-absorbable suture (e.g., #5 Ethibond, #2 FiberWire, or similar high-strength braided suture) is passed through the greater tuberosity fragment, then distally through the humeral shaft tunnels (or through the eyelets of suture anchors), and finally tied over the lateral cortex of the humeral shaft or around the anchors. This creates a figure-of-eight loop that compresses the fragment onto the humeral head.
-
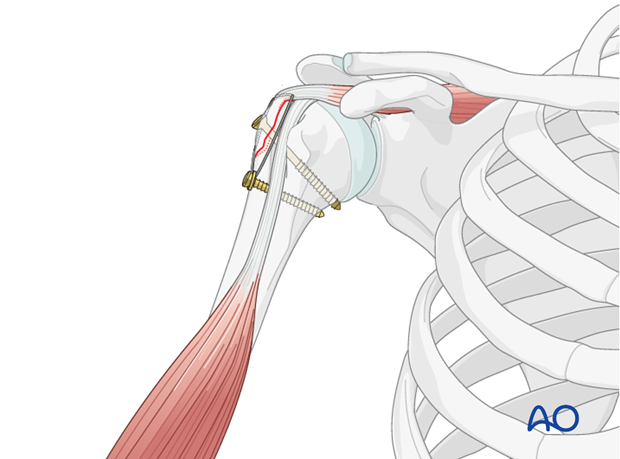
Adjunct Fixation: For larger or more comminuted greater tuberosity fractures, tension band sutures can be augmented with small screws (e.g., 2.7 mm or 3.5 mm cortical or cancellous screws) placed perpendicular to the fracture plane, or even with a small locking plate for multi-fragmentary patterns. The tension band sutures can then augment the plate/screw construct, especially to resist rotator cuff pull. This is particularly relevant when the GT fracture is part of a more complex proximal humeral fracture pattern.
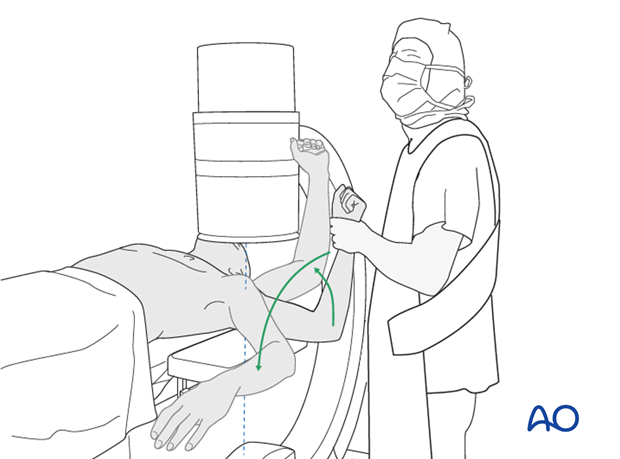
Intraoperative Assessment of Stability
After fixation, the shoulder's range of motion should be carefully assessed under fluoroscopy or direct visualization to confirm stable reduction, evaluate the security of the fixation, and ensure no impingement occurs throughout the functional arc of motion. Any instability or gapping at the fracture site requires re-evaluation and potentially revision of the fixation.
Wound Closure
After confirming stability, the surgical field is irrigated thoroughly. If a drain is indicated (e.g., significant bleeding or hematoma risk), it is placed away from the nerve and arterial structures. The deltoid muscle is repaired (if split), followed by meticulous, layered closure of the subcutaneous tissues and skin.
Complications and Management
Despite meticulous surgical technique, complications can arise following tension band suture fixation of humeral fractures, particularly those involving the greater tuberosity. Recognizing and managing these complications is crucial for optimizing patient outcomes.
Common Complications
-
Loss of Reduction/Nonunion/Malunion:
- Incidence: Varies, but can range from 5-20%. Higher in cases with poor bone quality, inadequate initial reduction, insufficient tensioning of sutures, or premature aggressive rehabilitation.
- Description: Loss of initial reduction often manifests as superior or posterior displacement of the GT fragment, leading to painful impingement and reduced range of motion. Nonunion (failure of bone healing by 6-9 months) or malunion (healing in an unacceptable position) can result in chronic pain, weakness, and functional limitations.
- Management:
- Minor loss of reduction without clinical symptoms may be observed.
- Symptomatic malunion or nonunion often necessitates revision surgery. This may involve osteotomy for correction of malunion, debridement of the nonunion site, bone grafting, and more robust fixation (e.g., plate and screw fixation, or revision tension band with improved technique), potentially augmented with allograft or autograft.
- For elderly patients with severe malunion and debilitating pain, shoulder arthroplasty (hemiarthroplasty or reverse total shoulder arthroplasty) may be considered as a salvage procedure.
-
Hardware Failure (Suture Breakage/Pull-Through):
- Incidence: Can occur in up to 10% of cases, particularly with early, unprotected motion or severe osteoporosis.
- Description: Suture breakage results in loss of fixation. Suture pull-through occurs when the sutures cut through soft bone, leading to loss of compression.
- Management: Symptomatic hardware failure requires re-evaluation. If displacement is significant and symptomatic, revision surgery with stronger fixation (e.g., locking plate, screws, or revised tension band with suture anchors) is indicated. In cases of failed tension band due to poor bone, augmenting with allograft or bone cement may be considered.
-
Impingement from Prominent Hardware/Scar Tissue:
- Incidence: Not uncommon, especially if knots are bulky or placed in a way that impinges on the acromion or rotator cuff during motion.
- Description: Pain and restricted motion due to mechanical irritation.
- Management: If conservative management (NSAIDs, physical therapy) fails, arthroscopic or open hardware removal, bursectomy, or even acromioplasty may be considered.
-
Infection:
- Incidence: Low, typically <1-2% for elective orthopedic surgeries.
- Description: Supervised infection (cellulitis) or deep surgical site infection (osteomyelitis).
- Management: Superficial infections may respond to oral antibiotics. Deep infections require surgical debridement, intravenous antibiotics, and potentially hardware removal if the infection persists or bone involvement is significant.
-
Neurovascular Injury:
- Incidence: Rare, but can be devastating. Axillary nerve injury is the most common, especially with lateral deltoid-splitting approaches or distal screw placement.
- Description: Axillary nerve injury can lead to deltoid weakness and sensory deficits over the lateral shoulder. Brachial plexus or vascular injury is extremely rare.
- Management: Meticulous surgical technique is the best prevention. Post-operatively, neurological deficits warrant prompt evaluation (EMG/NCS) and potential exploration and repair if indicated. Most iatrogenic nerve palsies are neuropraxias and resolve spontaneously.
-
Stiffness/Arthrofibrosis:
- Incidence: Common after shoulder trauma and surgery, ranging from 15-50%.
- Description: Restricted active and passive range of motion due to capsular contracture, scar tissue formation, or pain.
- Management: Aggressive but controlled physical therapy is paramount in the post-operative period. If stiffness persists despite optimal therapy, manipulation under anesthesia (MUA) or arthroscopic capsular release (arthrolysis) may be indicated.
-
Rotator Cuff Pathology:
- Incidence: Can be pre-existing, iatrogenic, or due to failed healing of the GT fragment.
- Description: Persistent pain, weakness, and limited motion if the rotator cuff is injured during surgery or fails to heal to the repositioned GT.
- Management: MRI can assess cuff integrity. Symptomatic rotator cuff tears may require revision repair, either open or arthroscopic.
Complications and Management Summary
| Complication | Typical Incidence | Description | Salvage Strategy / Management |
|---|---|---|---|
| Loss of Reduction / Nonunion / Malunion | 5-20% | Fragment displacement, failure of bone healing, or healing in an unacceptable position | Revision ORIF with bone grafting, osteotomy for malunion correction, shoulder arthroplasty for severe symptomatic cases |
| Hardware Failure (Suture Breakage/Pull-Through) | Up to 10% | Loss of fixation due to suture fatigue or cutting through bone | Revision ORIF with alternative/stronger fixation (e.g., locking plate, suture anchors), bone augmentation |
| Impingement from Prominent Hardware | Variable | Pain/restricted motion from mechanical irritation by sutures/knots | Hardware removal (if symptomatic and union achieved), bursectomy, acromioplasty (rare) |
| Infection | <1-2% | Superficial or deep surgical site infection | Oral/IV antibiotics, surgical debridement, hardware removal (for deep/persistent cases) |
| Neurovascular Injury (Axillary Nerve) | <1-2% | Deltoid weakness, sensory deficits over lateral shoulder | Observation for neuropraxia, EMG/NCS, surgical exploration and repair (if indicated) |
| Stiffness / Arthrofibrosis | 15-50% | Restricted active/passive range of motion | Aggressive physical therapy, manipulation under anesthesia, arthroscopic capsular release |
| Rotator Cuff Pathology | Variable | Pre-existing, iatrogenic, or failed healing leading to tears | MRI assessment, revision rotator cuff repair (open or arthroscopic) |
Post Operative Rehabilitation Protocols
Post-operative rehabilitation following tension band suture fixation of greater tuberosity fractures is a critical determinant of functional outcome. The protocol must balance protecting the repair with promoting early motion to prevent stiffness and optimize rotator cuff function. A phased approach, tailored to individual patient factors, fracture stability, and bone quality, is generally employed.
Phase I: Immobilization and Passive Range of Motion (Weeks 0-6)
The primary goals of this phase are to protect the repair, control pain and swelling, and initiate gentle passive motion to prevent stiffness.
- Immobilization: The arm is typically immobilized in a sling for 4-6 weeks, with strict instructions to avoid active shoulder motion. The sling may be removed for hygiene and specific exercises.
- Pain Management: Opioids, NSAIDs, and ice application are used to manage post-operative pain and swelling.
- Pendulum Exercises: Starting within the first week, gentle pendulum exercises are initiated, ensuring the patient understands to relax the shoulder muscles and let gravity assist. These help maintain joint nutrition and reduce pain.
- Passive Range of Motion (PROM):
- Forward Flexion: Initiated cautiously, typically in the supine position with the elbow flexed, using the contralateral hand to support the arm. Progression up to 90-120 degrees by 4-6 weeks, as tolerated.
- External Rotation: Initiated with the arm adducted and elbow flexed to 90 degrees. External rotation is performed gently, typically to 0-30 degrees initially, progressing up to 45 degrees by 6 weeks. Avoid any position that places stress on the repair (e.g., abduction with external rotation).
- Internal Rotation: Hand-to-back exercises are performed passively, gradually increasing internal rotation.
- Scapular Mobilization: Gentle scapular glides and shrugs can be performed to maintain scapular rhythm.
- Elbow, Wrist, Hand Exercises: Active range of motion for the elbow, wrist, and hand is encouraged throughout the day to prevent stiffness and promote circulation.
Precautions: No active shoulder elevation, abduction, or external rotation. Avoid lifting, pushing, or pulling with the affected arm. Do not weight-bear through the arm.
Phase II: Active-Assistive and Active Range of Motion (Weeks 6-12)
This phase focuses on gradually restoring active range of motion, initiating gentle strengthening, and improving proprioception.
- Discontinuation of Sling: The sling is typically discontinued around 6 weeks post-operatively, provided clinical and radiographic healing are progressing.
- Active-Assistive Range of Motion (AAROM):
- Using a wand, pulley system, or assistance from the contralateral hand, patients gradually increase active-assistive forward flexion and abduction.
- Continue passive external and internal rotation exercises.
- Active Range of Motion (AROM):
- Once AAROM is comfortable and pain-free, patients begin active range of motion exercises, focusing on regaining full flexion, abduction, and rotation.
- Progressive increase in the arcs of motion, aiming for near-full pain-free AROM by 10-12 weeks.
- Initiation of Strengthening:
- Isometrics: Gentle isometric exercises for the rotator cuff (internal rotation, external rotation, abduction) and deltoid are introduced, ensuring no pain at the fracture site.
- Theraband/Light Resistance: Very light resistance exercises using Theraband or light weights for internal and external rotation, scapular stabilization, and deltoid strengthening. Focus on proper form and controlled movements.
- Proprioceptive Exercises: Wall walks, ball rolling exercises, and gentle weight-bearing through the hand/forearm on a table (avoiding direct shoulder load).
Precautions: Avoid heavy lifting, sudden movements, or activities that cause pain. Continue to protect the repair from excessive strain.
Phase III: Strengthening and Return to Activity (Weeks 12+)
This phase focuses on progressive strengthening, functional training, and gradual return to full activity, including sports or work.
- Progressive Strengthening:
- Increase resistance and repetitions for rotator cuff and deltoid muscles using dumbbells, resistance bands, and machines.
- Focus on eccentric strengthening and sport-specific movements if applicable.
- Incorporate exercises for the entire upper kinetic chain, including core stability.
- Functional Training:
- Mimic daily activities and work-related tasks, gradually increasing load and complexity.
- Overhead activities are progressively introduced.
- Return to Sport/High-Demand Activities:
- Gradual return to recreational sports or demanding occupations, typically starting at 4-6 months, with full return often taking 6-12 months, depending on the sport and individual recovery. This is contingent on achieving symmetrical strength, full range of motion, and absence of pain.
- Throwing programs or sport-specific drills are initiated under supervision.
Key Considerations:
- Individualization: Rehabilitation protocols must be tailored to the patient's age, bone quality, fracture stability, co-morbidities, and functional goals.
- Pain as a Guide: Pain should be used as a guide; exercises should be performed without exacerbating pain.
- Patient Compliance: Adherence to the rehabilitation program is paramount for successful outcomes.
- Communication: Close communication between the surgeon, physical therapist, and patient is essential throughout the recovery process.
- Radiographic Assessment: Regular radiographic follow-up is necessary to monitor fracture healing.
Summary of Key Literature and Guidelines
The management of greater tuberosity fractures of the humerus, particularly with tension band suture fixation, is supported by a growing body of literature emphasizing the importance of anatomical reduction and stable fixation to prevent impingement and restore rotator cuff function.
Current guidelines from professional societies such as the American Academy of Orthopaedic Surgeons (AAOS) and the Orthopaedic Trauma Association (OTA) generally advocate for operative intervention in significantly displaced greater tuberosity fractures (>5 mm displacement, or >3 mm in the context of dislocation). The consensus highlights that non-operative treatment for these displaced fractures can lead to malunion, subacromial impingement, and chronic rotator cuff dysfunction, particularly in active individuals.
Tension Band Suture Outcomes and Efficacy
Studies evaluating tension band suture fixation for greater tuberosity fractures demonstrate good to excellent functional outcomes, high union rates, and relatively low complication rates, especially when compared to non-operative treatment of displaced fractures.
- Functional Outcomes: Several series report favorable results using various outcome scores such as Constant-Murley score, ASES score, and UCLA score, indicating good pain relief and functional restoration. Patients typically regain a significant range of motion, although some degree of residual stiffness can occur.
- Union Rates: Union rates for greater tuberosity fractures treated with tension band sutures are generally high, often exceeding 90%. The dynamic compression provided by the tension band principle is thought to contribute positively to fracture healing.
- Advantages of Suture Fixation:
- Minimally Invasive: Sutures can be applied through smaller incisions or even arthroscopically, potentially reducing soft tissue dissection.
- Reduced Hardware Prominence: Suture knots are less prominent than metal plates or screws, potentially reducing the need for hardware removal due to impingement.
- Biocompatibility: High-strength non-absorbable sutures are generally well-tolerated.
- Flexibility: Suture constructs can adapt to comminuted fragments and poor bone quality better than rigid screw fixation alone, particularly when combined with suture anchors.
- Rotator Cuff Integration: The technique often involves passing sutures through the rotator cuff, effectively repairing both the bone fracture and any associated soft tissue avulsion of the tendon insertion.
Comparison to Other Fixation Methods
While tension band sutures are effective, other fixation methods exist, each with its own indications and advantages:
- Screw Fixation: Direct screw fixation (lag screws) can provide strong interfragmentary compression. However, it requires a fragment of sufficient size and bone quality to hold the screw threads and can be challenging in osteoporotic bone or very small fragments. Screw heads can also be prominent and cause impingement.
- Plate Fixation: Small locking plates are sometimes used for greater tuberosity fractures, especially when they are part of a more complex proximal humeral fracture pattern or when comminution requires broader support. Plates provide rigid stability but are more invasive, carry a higher risk of hardware prominence, and may require a second surgery for removal.
- Suture Anchors: Suture anchors are frequently used in conjunction with tension band sutures, particularly to enhance fixation in the humeral head, especially in osteoporotic bone where transosseous tunnels might be compromised. They provide a strong purchase point for the tensioning sutures.
Current literature suggests that for isolated, reducible greater tuberosity fractures, tension band suture fixation provides comparable or superior biomechanical stability to screw fixation in resisting rotator cuff pull, particularly in cadaveric studies. The choice often comes down to surgeon preference, fracture morphology, and bone quality.
Areas of Ongoing Research
Ongoing research continues to refine surgical techniques, implant materials, and rehabilitation protocols for greater tuberosity fractures. Areas of interest include:
* Optimization of suture materials and knot configurations for maximum strength and minimal profile.
* The role of arthroscopic-assisted fixation techniques to minimize invasiveness.
* Development of patient-specific rehabilitation protocols based on real-time biomechanical feedback.
* Long-term outcomes of different fixation methods, especially in osteoporotic patients.
In conclusion, tension band suture fixation represents a robust and effective surgical option for displaced greater tuberosity fractures of the humerus. By understanding the underlying biomechanical principles, adhering to meticulous surgical technique, and implementing structured post-operative rehabilitation, orthopedic surgeons can achieve excellent functional outcomes and restore critical shoulder function in their patients.
Clinical & Radiographic Imaging
You Might Also Like