Operative Management of Shoulder Fractures: Scapula & Humerus

Key Takeaway
Fractures around the shoulder complex, encompassing the scapula, clavicle, and proximal humerus, present unique biomechanical challenges. While historically managed with benign neglect, modern orthopedic surgery emphasizes precise radiographic evaluation and targeted operative intervention. This guide details evidence-based indications, surgical approaches, and fixation techniques to optimize functional outcomes, mitigate post-traumatic arthrosis, and restore scapulothoracic kinematics in complex shoulder trauma.
FRACTURES AROUND THE SHOULDER: AN ADVANCED ACADEMIC OVERVIEW
The shoulder girdle is a highly complex, dynamically stabilized biomechanical linkage system. Fractures about the shoulder—specifically involving the scapula, clavicle, and proximal humerus—frequently compromise the Superior Shoulder Suspensory Complex (SSSC). The management of these injuries requires a profound understanding of local anatomy, deforming muscular forces, and the evolving evidence base regarding operative versus nonoperative interventions.
Historically, many of these fractures were treated with "benign neglect," relying on the extensive compensatory mobility of the scapulothoracic articulation. However, contemporary orthopedic traumatology recognizes that malunion in this region can lead to profound scapulothoracic dyskinesia, impingement syndromes, and early-onset glenohumeral arthrosis.
FRACTURES OF THE SCAPULA
Epidemiology and Mechanism of Injury
Fractures of the scapula are relatively rare, accounting for 3% to 5% of all fractures about the shoulder girdle, and less than 1% of all skeletal fractures. Because the scapula is heavily protected by a robust muscular envelope (the rotator cuff, trapezius, rhomboids, and serratus anterior), significant kinetic energy is required to fracture it. Consequently, these injuries are most often caused by high-energy trauma, such as motor vehicle collisions, motorcycle accidents, or falls from significant heights.
Clinical Pearl: Approximately 90% of patients with scapular fractures present with associated high-energy injuries. The trauma surgeon must maintain a high index of suspicion for ipsilateral rib fractures, pneumothorax, pulmonary contusions, closed head injuries, and brachial plexus traction injuries.
The Paradigm Shift in Treatment
Treatment of scapular fractures has traditionally been described as “benign neglect.” Like many clavicular fractures, the vast majority of isolated scapular fractures do well with conservative management. However, although outcomes are generally favorable, not all scapular fractures heal uneventfully. Over the past two decades, there has been a significant resurgence of interest in defining precise radiographic criteria to identify which patients will benefit from Open Reduction and Internal Fixation (ORIF).
In a landmark systematic review of the literature concerning scapular fractures, Zlowodzki et al. analyzed 520 reported fractures and found that 82% achieved good-to-excellent functional results overall.
* Scapular Body Fractures: Almost all were treated nonoperatively, yielding 86% good-to-excellent results.
* Scapular Neck and Isolated Glenoid Fractures: These were most often treated operatively (83%), with good-to-excellent results in 76% and 82%, respectively.
Although the absolute numbers of specific fracture patterns in the literature remain relatively small, the overall functional results following operative treatment have consistently proven superior to nonoperative treatment in appropriately selected, highly displaced fracture types. Lantry et al. corroborated these findings in a subsequent systematic review, reporting good-to-excellent functional results in approximately 85% of patients undergoing ORIF.
Radiographic Evaluation and Decision-Making Criteria
Standard trauma radiographs (True AP, Scapular Y, and Axillary lateral views) are mandatory. However, plain radiography is often insufficient for operative planning due to the complex three-dimensional anatomy of the scapula and overlapping thoracic structures.
Surgical Warning: Three-dimensional Computed Tomography (3D-CT) with subtraction of the humeral head and rib cage is the gold standard. Anavian et al. demonstrated that 3D-CT is significantly more reliable than plain radiography in evaluating extra-articular scapular fracture displacement, particularly regarding angular deformity and medialization.
The Glenopolar Angle (GPA)
The Glenopolar Angle is a critical radiographic parameter used to assess rotational malalignment of the glenoid neck. It is measured on a true AP radiograph or 3D-CT.
* Measurement: A line is drawn from the superior pole to the inferior pole of the glenoid fossa. A second line is drawn from the superior pole of the glenoid fossa to the inferiormost angle of the scapular body.
* Normal Range: 30 to 45 degrees.
* Clinical Significance: A GPA of 22 degrees or less indicates severe rotational displacement and is a strong predictor of poor functional outcome if treated nonoperatively.
Cole’s Criteria for Operative Intervention
While the literature is still evolving to formulate concrete, universally accepted treatment guidelines, Cole et al. established highly regarded criteria for the operative treatment of extra-articular scapular fractures:
1. Lateral Border Offset: A 2-cm (20 mm) medial/lateral translation (offset) of the lateral border of the scapula.
2. Angular Deformity: Forty-five degrees or more of scapular body angulation, as measured on a Scapular Y view or axial CT.
3. Glenopolar Angle: A GPA of 22 degrees or less.
4. Double Disruptions of the SSSC: A scapular body/neck fracture associated with a displaced clavicle fracture or acromioclavicular joint disruption.
Operative Techniques for Scapular Fractures
Glenoid Fractures (Intra-articular)
Glenoid fractures must be treated with the same biomechanical respect as any other major weight-bearing intra-articular fracture.
* Indications: ORIF is strictly indicated when there is significant (> 4 mm) step-off or displacement through the articular surface that leads to joint subluxation, dynamic instability, or severe incongruency.
* Surgical Approach: The operative approach of choice is the classic Judet or the modified Judet approach. For anterior glenoid rim fractures (Ideberg Type I), a standard deltopectoral approach is utilized.
Scapular Body and Neck Fractures (Extra-articular)
Fractures of the scapular body or neck that meet Cole's criteria are at high risk for malunion, which alters the resting posture of the scapula and leads to severe impingement and rotator cuff dysfunction.
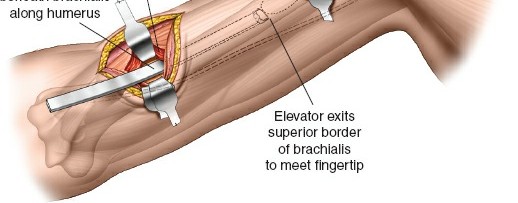
- The Modified Judet Approach:
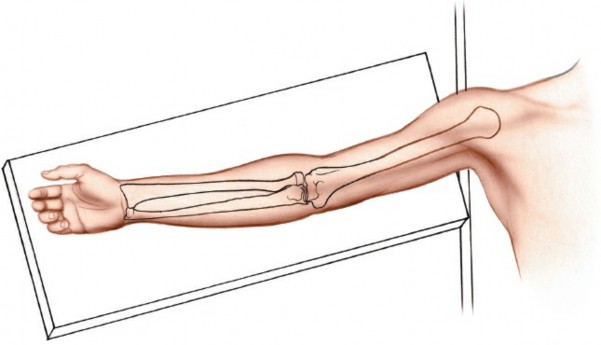
- Positioning: The patient is placed in the lateral decubitus or prone position with the operative arm draped free over a sterile Mayo stand.
- Incision: A "boomerang" or L-shaped incision is made along the spine of the scapula, curving distally along the medial border.
- Internervous Plane: The deltoid is elevated off the scapular spine. The infraspinatus is elevated from medial to lateral.
- Neurological Pitfall: Extreme care must be taken to protect the suprascapular nerve and vessels as they pass through the spinoglenoid notch. Retraction of the infraspinatus must be gentle to avoid traction neuropraxia.
- Fixation: Reduction is achieved using pointed reduction forceps. Fixation relies on the thickest pillars of the scapula: the lateral border and the scapular spine. Low-profile 2.7 mm or 3.5 mm reconstruction plates are contoured to the lateral border.
Nonoperative Management Protocol
For the vast majority of scapular body fractures that do not meet operative criteria, conservative treatment is an active, structured process—not merely "benign neglect."
1. Immobilization: The shoulder is immobilized in a sling for 2 to 3 weeks to allow the initial hematoma to organize and pain to subside.
2. Early Motion: An active-assisted range-of-motion (ROM) protocol is initiated as soon as pain permits (typically around day 10-14) to prevent adhesive capsulitis.
3. Strengthening: Progressive active ROM and isometric strengthening exercises are permitted only when fracture healing is confirmed clinically (absence of point tenderness) and radiographically (callus formation), usually at 6 to 8 weeks.
ASSOCIATED CLAVICULAR TRAUMA & THE SSSC
Because the scapula and clavicle form a continuous biomechanical ring (the SSSC), high-energy trauma often disrupts both structures. A floating shoulder occurs when there is an ipsilateral fracture of the clavicle and the scapular neck. In these instances, stabilizing the clavicle alone may indirectly reduce the scapular neck.
Distal Clavicle Fractures and Hook Plate Fixation
Distal third clavicle fractures (Neer Type II) are notoriously unstable. The proximal fragment is pulled superiorly by the sternocleidomastoid muscle, while the distal fragment and the entire shoulder girdle are pulled inferiorly by gravity and the weight of the arm. Due to the disruption of the coracoclavicular (CC) ligaments, these fractures have a nonunion rate approaching 30% if treated nonoperatively.
When the distal fragment is too small to accommodate standard lag screws or a locking plate, a Clavicle Hook Plate is an excellent biomechanical solution. The hook passes under the acromion, providing a rigid lever that holds the proximal clavicle reduced against the deforming forces, allowing the CC ligaments and the fracture to heal.
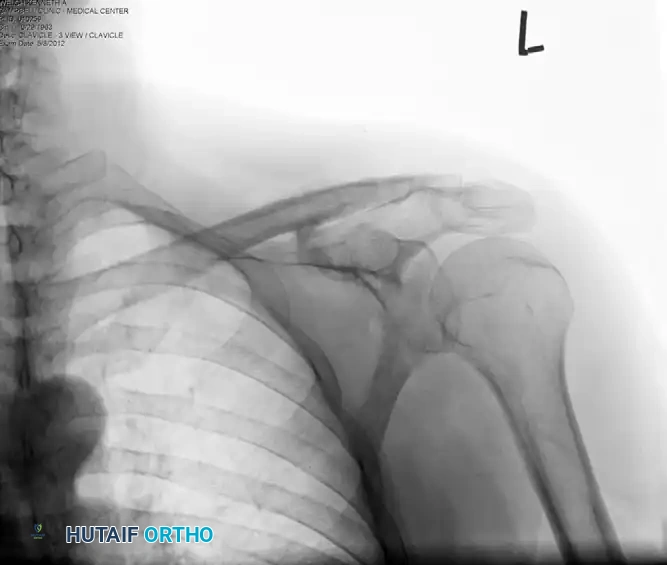
Clinical Case Example:
Below is a radiographic progression of a highly displaced distal clavicle fracture managed with a hook plate.
Preoperative Evaluation: Note the severe superior displacement of the proximal clavicular shaft, indicating complete loss of the coracoclavicular ligamentous restraint.
Postoperative Fixation: The fracture is anatomically reduced and stabilized using a clavicular hook plate. The hook is engaged beneath the acromion, neutralizing superior translation.

Hardware Removal: Because the hook plate alters normal acromioclavicular joint kinematics and can cause acromial osteolysis or subacromial impingement over time, routine removal is mandated after radiographic union is achieved (typically at 4 to 6 months).
PROXIMAL HUMERAL FRACTURES
"The surgeon must accurately assess the fracture pattern, understand the technical pitfalls, and thoughtfully supervise the postoperative patient care."
— R.H. Cofield (1988)
Cofield’s succinct summary regarding the treatment of proximal humeral fractures remains as relevant today as it was decades ago. It highlights the profound difficulty of treating these injuries—from the initial radiographic evaluation to the final functional outcome.
The Clinical Dilemma
Despite advances in locking plate technology and arthroplasty, much controversy and confusion still exist. No single treatment protocol or algorithm has been proven to be universally effective. As indicated by Cofield, areas still heavily debated in orthopedic literature include:
* Inter- and intra-observer reliability of radiographic diagnosis.
* The threshold for operative versus nonoperative treatment.
* The role of physiological patient age and bone density (osteoporosis) in decision-making.
* The choice of surgical approach (Deltopectoral vs. Anterolateral Acromial).
* The decision between joint-preserving fracture fixation (ORIF) versus joint-sacrificing procedures (Hemiarthroplasty or Reverse Total Shoulder Arthroplasty).
Epidemiology and Nonoperative Outcomes
Proximal humeral fractures are the third most common fracture in patients over the age of 65. Numerous authors have historically suggested that nonoperative treatment may be preferable for two-, three-, and even four-part proximal humeral fractures in elderly, low-demand patients. However, modern outcome studies report significant pain, malunion, and profound loss of forward elevation in high percentages of patients following nonoperative treatment of displaced fractures.
Conversely, Court-Brown et al. reported good or excellent results in 81% of impacted valgus fractures in elderly patients treated nonoperatively. In a direct comparison of operative and nonoperative treatment of displaced two-part fractures, these authors found statistically similar functional results between the two cohorts, emphasizing that fracture pattern—not just displacement—dictates the success of conservative care.
Geographical Variations in Treatment
The lack of consensus is glaringly apparent in epidemiological data. In a study of the geographical incidence and treatment variation of common fractures in elderly Medicare patients, Sporer et al. found massive variations in the percentage of proximal humeral fractures treated operatively across the United States.
* Operative rates ranged wildly from 6.4% to 60%.
* In eight regions, at least 40% were treated operatively.
* In 35 regions, fewer than 20% were treated operatively.
The fact that over 10 different fixation techniques (percutaneous pinning, intramedullary nailing, locking plates, tension band wiring, hemiarthroplasty, RTSA, etc.) are routinely evaluated for a single fracture type (surgical neck fractures) is a definitive indication of the complexity and lack of consensus in treating proximal humeral trauma.
Classification: The Neer System
The most universally utilized classification system for proximal humeral fractures is the Neer Classification. Developed by Charles S. Neer II in 1970, it is based on the anatomical relationship of the four major segments of the proximal humerus:
1. The Articular Segment (Humeral Head)
2. The Greater Tuberosity
3. The Lesser Tuberosity
4. The Humeral Shaft
Biomechanical Principle: Neer defined a "part" not merely by the presence of a fracture line, but by displacement. A segment is only considered a separate "part" if it is displaced by more than 1 centimeter or angulated by more than 45 degrees relative to the other fragments.
While the Neer classification is foundational for communication among surgeons, it has been criticized for limited inter-observer reliability and reproducibility. 3D-CT is increasingly utilized to improve the accuracy of preoperative classification, particularly in assessing the degree of medial calcar comminution and the exact position of the tuberosities, which dictate the viability of the humeral head's blood supply (primarily via the ascending branch of the anterior circumflex humeral artery).
Operative Strategies for the Proximal Humerus
Open Reduction and Internal Fixation (ORIF)
For displaced 2-part and 3-part fractures in patients with reasonable bone stock, ORIF with a Proximal Humeral Interlocking System (PHILOS) or similar locking plate is the standard of care.
* Approach: The Deltopectoral approach utilizes the internervous plane between the deltoid (axillary nerve) and the pectoralis major (medial and lateral pectoral nerves).
* Technique: The tuberosities are controlled with heavy non-absorbable sutures (e.g., #2 FiberWire). The fracture is reduced, and the locking plate is applied lateral to the bicipital groove, avoiding superior placement to prevent subacromial impingement.
* Calcar Support: The placement of inferomedial locking screws into the calcar region is biomechanically critical to prevent secondary varus collapse of the humeral head.
Arthroplasty (Hemiarthroplasty vs. RTSA)
In elderly patients with severe osteoporosis, 4-part fractures, or head-splitting components where the risk of avascular necrosis (AVN) approaches 100%, arthroplasty is indicated.
* Hemiarthroplasty: Historically the procedure of choice, but outcomes are heavily dependent on the anatomic healing of the tuberosities to the prosthesis. If the tuberosities resorb or migrate, the patient will suffer from profound pseudoparalysis.
* Reverse Total Shoulder Arthroplasty (RTSA): RTSA has rapidly become the treatment of choice for complex 3- and 4-part fractures in the elderly. By medializing the center of rotation and increasing the lever arm of the deltoid, RTSA provides reliable forward elevation and pain relief, even in the setting of tuberosity nonunion or rotator cuff failure.
Postoperative Rehabilitation
Whether managing a scapular fracture, a clavicular hook plate, or a proximal humeral locking plate, the rehabilitation philosophy remains consistent: protect the fixation while preventing capsular contracture.
* Phase I (0-4 weeks): Sling immobilization. Passive ROM only (pendulum exercises, passive forward elevation). No active internal/external rotation to protect tuberosity fixation.
* Phase II (4-8 weeks): Transition to active-assisted ROM. Discontinue sling.
* Phase III (8-12 weeks): Initiate active ROM and light resistance bands once radiographic union is confirmed.
* Phase IV (3-6 months): Advanced strengthening and return to functional baseline. Maximum medical improvement is typically not reached until 12 to 18 months post-injury.
You Might Also Like