Unlock the Anterior Compartment of the Forearm: Surgical Keys
Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Unlock the Anterior Compartment of the Forearm: Surgical Keys. The anterior compartment of the forearm contains two primary muscle groups: the mobile wad of three (brachioradialis, extensor carpi radialis longus, and brevis), innervated by the radial nerve; and the flexor-pronator muscles, supplied by the median and ulnar nerves. The flexor-pronator group is further organized into superficial, middle, and deep layers.
Introduction and Epidemiology
The anterior compartment of the forearm represents a complex anatomic and functional domain that demands precise surgical navigation. Encompassing the flexor-pronator musculature, critical neurovascular bundles, and the volar aspects of the radius and ulna, this region is frequently accessed in orthopedic trauma and reconstructive surgery. Operative interventions in this area range from open reduction and internal fixation of diaphyseal forearm fractures to flexor tendon repairs, nerve decompressions, and emergent fasciotomies for acute compartment syndrome.
Epidemiologically, diaphyseal fractures of the radius and ulna account for approximately ten to fourteen percent of all upper extremity fractures in the adult population. These injuries often result from high-energy trauma, such as motor vehicle collisions, or low-energy falls in osteoporotic individuals. The anterior compartment is also uniquely susceptible to volar compartment syndrome due to the dense fascial envelopes enclosing the deep flexor musculature. Understanding the intricate applied surgical anatomy of the anterior forearm is paramount for minimizing iatrogenic neurovascular injury, achieving anatomic restoration of the radial bow, and restoring the complex biomechanics of forearm pronation and supination. Mastery of the internervous planes allows the orthopedic surgeon to unlock the anterior compartment safely, facilitating optimal functional outcomes.
Surgical Anatomy and Biomechanics
The musculature of the anterior aspect of the forearm is divided into two primary functional and anatomic groups. The lateral border of the supinated forearm is formed by the mobile wad of three, while the remainder of the volar forearm comprises the flexor-pronator mass.
The Mobile Wad of Three
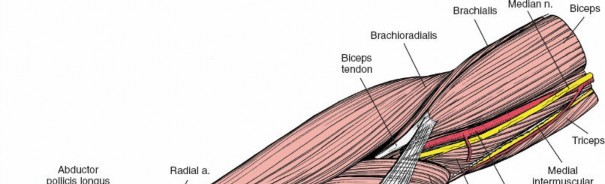
The mobile wad consists of the brachioradialis, the extensor carpi radialis longus, and the extensor carpi radialis brevis. Innervated exclusively by the radial nerve, this muscle group forms the lateral boundary of the primary anterior internervous plane. Retracting the mobile wad laterally is the foundational step in the volar approach to the proximal radius.

Superficial Flexor Pronator Layer
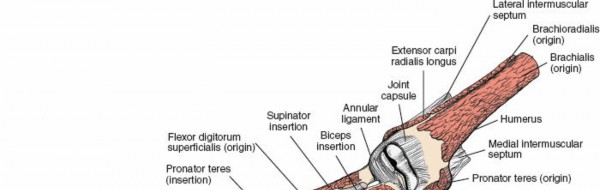
The flexor-pronator group is supplied by the median and ulnar nerves and is arranged in three distinct layers. The superficial layer arises from the common flexor origin on the medial humeral epicondyle and fans out distally across the forearm. This layer can be easily conceptualized using a classic anatomic maneuver. By placing the butt of the opposite hand over the medial epicondyle with the palm resting on the anterior surface of the forearm, the digits represent the trajectory of the superficial muscles. The thumb points in the direction of the pronator teres, the index finger represents the flexor carpi radialis, the middle finger represents the palmaris longus, and the ring finger represents the flexor carpi ulnaris.

Middle Flexor Pronator Layer
The middle layer of the anterior compartment consists entirely of a single, complex muscle belly, the flexor digitorum superficialis. This muscle possesses two distinct heads of origin, the humeroulnar head and the radial head. The median nerve and ulnar artery pass deep to the fibrous arch connecting these two heads, a critical anatomic relationship that must be respected during deep dissection or compartment syndrome decompression.

Deep Flexor Pronator Layer
The deep layer comprises three muscles. The flexor digitorum profundus and the flexor pollicis longus provide terminal flexion to the digits and thumb, respectively. Distally, the pronator quadratus spans the distal radius and ulna. While not strictly a flexor, the supinator muscle is intimately related to the deep anatomy of the proximal anterior forearm and is critical to surgical exposure. The deep layer is innervated primarily by the anterior interosseous nerve, a branch of the median nerve, with the exception of the ulnar half of the flexor digitorum profundus, which is innervated by the ulnar nerve.
Neurovascular Anatomy
The anterior compartment houses the primary vascular supply to the hand. The brachial artery bifurcates in the antecubital fossa into the radial and ulnar arteries. The radial artery travels distally under the cover of the brachioradialis. The ulnar artery dives deep to the pronator teres and travels distally between the flexor carpi ulnaris and the flexor digitorum profundus. The median nerve exits the antecubital fossa by passing between the two heads of the pronator teres, while the ulnar nerve enters the forearm between the two heads of the flexor carpi ulnaris.

Biomechanics of the Forearm Axis
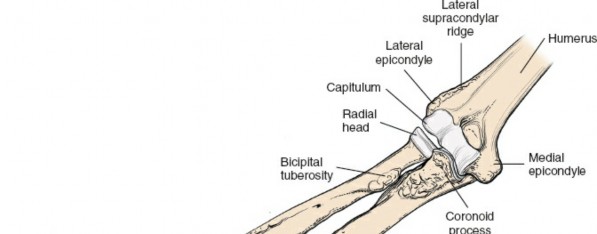
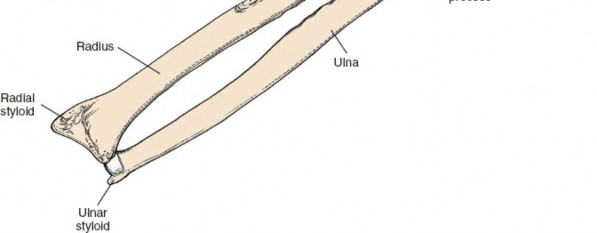
The forearm functions as a complex articulated ring, analogous to the pelvic ring. The radius and ulna articulate at the proximal and distal radioulnar joints, stabilized by the interosseous membrane. The radius possesses a distinct lateral and dorsal bow that is essential for generating the clearance required for full pronation and supination. Surgical restoration of this radial bow is a strict biomechanical requirement during osteosynthesis; failure to restore the anatomic contour directly correlates with a proportional loss of rotational arc.
Indications and Contraindications
Surgical intervention in the anterior compartment of the forearm is dictated by the need to restore skeletal stability, decompress neurovascular structures, or repair soft tissue disruptions. The classic volar approach to the radius provides unparalleled access to the diaphyseal and metaphyseal regions of the bone.
| Indication Category | Operative Indications | Non Operative Indications |
|---|---|---|
| Diaphyseal Fractures | Displaced both bone forearm fractures in adults | Nondisplaced or minimally displaced isolated ulnar shaft fractures |
| Isolated radial shaft fractures (Galeazzi variants) | Pediatric both bone fractures with acceptable angulation | |
| Open fractures requiring debridement | Fractures in patients with prohibitive medical comorbidities | |
| Compartment Syndrome | Clinical signs of acute volar compartment syndrome | Equivocal compartment pressures with improving clinical exam |
| Intracompartmental pressure within thirty millimeters of mercury of diastolic pressure | Chronic exertional compartment syndrome responsive to rest | |
| Soft Tissue Reconstruction | Acute laceration of flexor tendons or median and ulnar nerves | Partial tendon lacerations without triggering or weakness |
| Excision of volar compartment neoplasms | Small asymptomatic lipomas or benign cysts |
Absolute contraindications to the volar approach include active overlying soft tissue infection or compromised soft tissue envelopes that preclude safe surgical incisions. Relative contraindications include severe medical comorbidities precluding anesthesia.

Pre Operative Planning and Patient Positioning
Thorough preoperative planning is essential for successful navigation of the anterior forearm. Standard orthogonal imaging, including true anteroposterior and lateral radiographs of the forearm, wrist, and elbow, must be obtained to assess the fracture pattern, identify radioulnar joint subluxation, and template for implant selection.
Digital Templating and Implant Selection
Digital templating is utilized to determine plate length and screw configuration. For diaphyseal forearm fractures, current standards dictate the use of three point five millimeter dynamic compression plates or locking compression plates. The surgeon must ensure a minimum of three bicortical screws, or six cortices, are placed on either side of the fracture to provide adequate biomechanical stability.
Patient Positioning and Setup
The patient is placed in the supine position on the operating table. The operative upper extremity is extended onto a radiolucent hand table. A pneumatic tourniquet is placed high on the brachium to provide a bloodless surgical field, though it should be used judiciously, particularly in cases of suspected compartment syndrome or prolonged microvascular reconstruction.

The arm is prepped and draped in a standard sterile fashion, allowing for free mobility of the elbow, forearm, and wrist. The ability to freely pronate and supinate the forearm during the procedure is critical, as dynamic positioning shifts the neurovascular structures and facilitates access to different aspects of the radial circumference.
Detailed Surgical Approach and Technique
The volar approach to the radius, commonly referred to as the Henry approach, is the workhorse exposure for the anterior compartment. It exploits the internervous plane between the radial nerve innervated musculature and the median nerve innervated musculature.
Incision and Superficial Dissection
The skin incision extends from the lateral aspect of the biceps tendon at the elbow flexion crease, coursing distally toward the radial styloid. The length of the incision is dictated by the pathology being addressed.

Following skin incision, the subcutaneous tissues are divided. Proximally, care must be taken to identify and protect the lateral antebrachial cutaneous nerve, which courses alongside the cephalic vein. Distally, the superficial branch of the radial nerve emerges from beneath the brachioradialis and must be meticulously protected.

Developing the Internervous Plane
The deep fascia is incised in line with the skin incision. The internervous plane is developed between the brachioradialis laterally and the pronator teres and flexor carpi radialis medially.

Proximally, the plane lies between the brachioradialis and the pronator teres. Distally, the plane transitions between the brachioradialis and the flexor carpi radialis. Retracting the brachioradialis laterally and the flexor pronator mass medially exposes the superficial radial nerve and the radial artery. The radial artery must be mobilized and retracted medially with the flexor muscles to protect it during the deeper dissection.

Deep Dissection and the Leash of Henry
Exposure of the proximal third of the radius requires managing the recurrent radial artery and its associated venae comitantes, collectively known as the leash of Henry. These vessels branch from the radial artery and fan out laterally across the operative field to supply the brachioradialis and mobile wad. They must be isolated, ligated, and divided to permit lateral retraction of the mobile wad and radial artery mobilization.

Once the leash is divided, the supinator muscle is visualized wrapping around the proximal radius. The deep branch of the radial nerve, or posterior interosseous nerve, traverses the substance of the supinator. To safely expose the proximal radius, the forearm is fully supinated to carry the posterior interosseous nerve laterally and away from the surgical field. The supinator is then sharply detached from its insertion on the anterior aspect of the radius and reflected laterally, providing a thick muscular cushion that protects the posterior interosseous nerve from retractor injury.
Exposing the Middle and Distal Radius
In the middle third of the forearm, the insertion of the pronator teres on the lateral convexity of the radius is encountered. For extensive exposures or fracture reduction, this insertion can be elevated in a step cut fashion to facilitate later repair, or elevated subperiosteally.
In the distal third of the forearm, the flexor pollicis longus and pronator quadratus cover the volar surface of the radius. The flexor pollicis longus can be retracted medially. The pronator quadratus is typically incised along its lateral and distal borders and elevated medially as an L shaped flap, exposing the distal radial metaphysis.
Volar Forearm Fasciotomy Technique
When acute compartment syndrome is diagnosed, a volar fasciotomy is mandated. The incision begins proximal to the elbow crease, extending distally over the volar forearm, and crossing the wrist crease obliquely to decompress the carpal tunnel. The superficial fascia is released over the entire length of the flexor carpi ulnaris and flexor carpi radialis.

Crucially, the deep compartments must also be released. The epimysium of the flexor digitorum superficialis is incised, and the muscle bellies are retracted to expose the deep compartment containing the flexor digitorum profundus and flexor pollicis longus. The fascial envelopes of these deep muscles are systematically opened. The median nerve must be decompressed throughout its course, particularly at the bicipital aponeurosis, the pronator teres, and the fibrous arch of the flexor digitorum superficialis.
Complications and Management
Surgical intervention in the anterior compartment carries inherent risks due to the dense concentration of vital structures. Meticulous surgical technique and a profound understanding of three dimensional anatomy are required to minimize these complications.
| Complication | Estimated Incidence | Prevention and Salvage Strategies |
|---|---|---|
| Posterior Interosseous Nerve Palsy | One to five percent | Supinate forearm during supinator reflection. Avoid aggressive lateral retractor placement. Observe for spontaneous recovery; explore if no clinical improvement by three months. |
| Superficial Radial Nerve Injury | Two to four percent | Meticulous superficial dissection distally. Avoid vigorous traction. Treat painful neuromas with excision and proximal burying into muscle. |
| Radioulnar Synostosis | Two to six percent | Utilize separate incisions for radius and ulna fractures. Avoid dissecting through the interosseous membrane. Treat with delayed surgical excision after skeletal maturity and maturation of heterotopic ossification. |
| Nonunion or Malunion | Three to ten percent | Ensure rigid fixation with absolute stability for simple patterns. Restore the anatomic radial bow. Treat with revision osteosynthesis, autologous bone grafting, and correction of deformity. |
| Radial Artery Injury | Less than one percent | Careful identification and medial retraction. Ligate the leash of Henry meticulously. If lacerated, perform primary microvascular repair or ligate if collateral ulnar flow is robust based on Allen testing. |
Neurologic Complications
Neurologic injury remains one of the most devastating complications of anterior forearm surgery. The posterior interosseous nerve is at highest risk during proximal radius exposure. Traction injuries or direct laceration during supinator elevation can result in a loss of digital and thumb extension.

The superficial branch of the radial nerve is vulnerable in the distal half of the incision. Injury to this sensory nerve can lead to debilitating neuromas. The anterior interosseous nerve can be injured during deep retraction of the flexor digitorum profundus or pronator quadratus, leading to weakness in terminal thumb and index finger flexion.

Osseous Complications
Failure to restore the anatomic bow of the radius will predictably result in a loss of forearm rotation. Studies have demonstrated that a malreduction altering the maximum radial bow by more than a few millimeters significantly restricts the arc of pronation and supination. Nonunion is typically the result of inadequate mechanical stability or compromised biology. Revision surgery requires meticulous debridement of the nonunion site, rigid plate fixation, and often the application of autologous iliac crest bone graft to stimulate osteogenesis.
Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol is heavily dependent on the stability of the internal fixation and the status of the soft tissue envelope. The primary goal is to restore the functional arc of motion while protecting the osteosynthesis construct.
Phase One Immediate Post Operative Period
For the first ten to fourteen days, the forearm is typically immobilized in a well padded short arm or long arm splint, depending on the fracture configuration and surgeon preference. Elevation and active digital range of motion are initiated immediately to control edema and prevent flexor tendon adhesions.

Phase Two Early Range of Motion
Upon suture removal at two weeks, provided rigid internal fixation was achieved, the patient is transitioned to a removable orthosis. Active and active assisted range of motion exercises for the wrist, forearm, and elbow are commenced. Pronation and supination exercises are emphasized, as rotation is the most difficult motion to regain following anterior compartment surgery.
Phase Three Strengthening
At six to eight weeks postoperatively, clinical and radiographic assessments are performed to evaluate fracture consolidation. Once bridging callus is evident or the fracture lines are obscuring on radiographs, progressive strengthening exercises are initiated. Full, unrestricted activity and return to heavy manual labor or contact sports are generally delayed until twelve to sixteen weeks, contingent upon complete radiographic union.
Summary of Key Literature and Guidelines
The surgical management of the anterior compartment of the forearm is built upon decades of anatomic and biomechanical research. The foundational anatomic descriptions by A.K. Henry remain the gold standard for the volar approach to the radius, detailing the critical internervous planes and the management of the recurrent radial vessels.

Biomechanical studies by Anderson et al. established the modern principles of compression plating for diaphyseal forearm fractures, demonstrating the necessity of rigid internal fixation to achieve primary bone healing and permit early mobilization. Furthermore, literature by Schemitsch and Richards highlighted the critical importance of restoring the anatomic radial bow to preserve the functional arc of forearm rotation. In the context of compartment syndrome, guidelines established by Mubarak and Hargens dictate the thresholds for intracompartmental pressure monitoring and the necessity of complete fascial release of all volar compartments to prevent irreversible ischemic contracture. Adherence to these established academic principles ensures that the orthopedic surgeon can safely unlock the anterior compartment and achieve optimal patient outcomes.
You Might Also Like

