Lateral Approach to the Hindfoot: Surgical Anatomy, Biomechanics, and Clinical Applications
Key Takeaway
The lateral approach to the hindfoot is a key surgical technique, offering critical exposure for talocalcaneal, calcaneocuboid, and talonavicular pathologies like arthritis and deformities. Success demands thorough understanding of hindfoot anatomy, biomechanics, and precise neurovascular protection, especially of the vulnerable sural nerve.
Introduction & Epidemiology
The lateral approach to the hindfoot is a foundational surgical technique, providing critical exposure for addressing a spectrum of pathologies affecting the talocalcaneal (subtalar), calcaneocuboid, and talonavicular joints. As a workhorse approach, it facilitates interventions ranging from arthrodesis for end-stage arthritis or complex deformities to open reduction and internal fixation of certain calcaneal or talar fractures. Its versatility stems from its ability to provide direct visualization of the lateral hindfoot articulations while minimizing critical neurovascular compromise when executed meticulously.
Epidemiologically, the conditions most frequently necessitating a lateral hindfoot approach include post-traumatic arthritis (e.g., following calcaneal or talar fractures), primary degenerative osteoarthritis, inflammatory arthropathies, neuromuscular deformities (e.g., pes cavovarus), and failed previous hindfoot fusions. While the precise incidence of each individual pathology varies, the prevalence of hindfoot arthritis, particularly subtalar and calcaneocuboid involvement, steadily increases with age and history of trauma, making this approach highly relevant in a busy orthopedic practice. The lateral approach often serves as the primary gateway for procedures such as triple arthrodesis, a common salvage procedure for rigid, painful hindfoot deformities, with reported fusion rates typically exceeding 85%.
Surgical Anatomy & Biomechanics
A thorough understanding of the intricate anatomy and biomechanics of the hindfoot is paramount for successful execution of the lateral approach and optimal patient outcomes.
Osseous Structures
The primary osseous targets for this approach include the talus, calcaneus, and cuboid bone.
*
Talus:
The body of the talus articulates with the calcaneus inferiorly, forming the subtalar joint. Its head articulates with the navicular anteriorly and medially, forming part of the talonavicular joint, and also with the spring ligament.
*
Calcaneus:
The largest tarsal bone, it articulates with the talus superiorly (subtalar joint) and the cuboid anteriorly (calcaneocuboid joint). The lateral wall of the calcaneus is a key landmark and often the site of bone graft harvest or plate application.
*
Cuboid:
Articulates with the calcaneus posteriorly and the fourth and fifth metatarsals anteriorly. Its lateral border is easily palpable.
Articulations
The lateral approach provides excellent exposure of the following joints:
*
Talocalcaneal (Subtalar) Joint:
Formed by the inferior facet of the talus and the superior facets of the calcaneus. Motion primarily involves inversion and eversion of the hindfoot. The sinus tarsi, a conical canal between the talus and calcaneus, contains the interosseous talocalcaneal ligament and cervical ligament, crucial stabilizers that must be resected during subtalar arthrodesis.
*
Calcaneocuboid Joint:
A syndesmotic-type joint with limited motion, but critical for the transverse tarsal joint (Chopart's joint) complex, which allows for adaptive forefoot pronation/supination.
*
Talonavicular Joint:
While less directly exposed from a pure lateral approach, adequate distraction and manipulation of the calcaneus and midfoot often allow for preparation and fixation, particularly during a triple arthrodesis. It is a ball-and-socket joint, crucial for forefoot abduction/adduction and contributing significantly to the mobility of the medial longitudinal arch.
Ligamentous Structures
Key ligaments in the vicinity:
*
Interosseous Talocalcaneal Ligament (ITCL):
Located within the sinus tarsi, it is a strong, thick ligament vital for subtalar stability.
*
Cervical Ligament:
Also within the sinus tarsi, anterior to the ITCL.
*
Lateral Collateral Ligaments of the Ankle:
Calcaneofibular ligament (CFL) and anterior talofibular ligament (ATFL) are superficial to the surgical field but require careful handling if the incision is extended proximally.
*
Bifurcate Ligament:
Consists of the calcaneonavicular and calcaneocuboid ligaments, located on the dorsum of the midfoot, anterior to the sinus tarsi. Its division is often necessary to facilitate exposure of the talonavicular joint during a triple arthrodesis.
*
Dorsal Calcaneocuboid Ligament:
Reinforces the calcaneocuboid joint dorsally.
*
Long and Short Plantar Ligaments:
While on the plantar aspect, their integrity is important for overall foot stability and arch support, and care must be taken not to violate them unnecessarily.
Neurovascular Structures
- Sural Nerve: The most vulnerable structure in a lateral hindfoot approach. It originates from the tibial and common peroneal nerves, descends posterolaterally, and becomes subcutaneous as it crosses posterior to the lateral malleolus. It innervates the lateral aspect of the foot and fifth toe. Its course must be identified and protected, often lying within the subcutaneous fat or superficial fascia.
- Superficial Peroneal Nerve: Its terminal branches (intermediate dorsal cutaneous nerve and medial dorsal cutaneous nerve) may be at risk with more dorsal or extensive incisions, but generally lie anterior to the primary dissection plane.
- Peroneal Artery: Located deep within the posterior compartment, its perforating branches can be encountered in deep dissection, particularly near the lateral malleolus.
- Peroneal Tendons (Peroneus Longus and Brevis): These tendons run posterior to the lateral malleolus within a common sheath, then diverge; the brevis inserts on the base of the fifth metatarsal, and the longus passes into the cuboid groove. They are typically retracted dorsally or posteriorly to access the underlying calcaneus and cuboid.
Muscular Structures
- Extensor Digitorum Brevis (EDB): Originates from the anterior superior calcaneus within the sinus tarsi. Its muscle belly lies within the deep fascia. It is often elevated from its origin and retracted dorsally/anteriorly to expose the sinus tarsi and subtalar joint capsule.
Biomechanics
The hindfoot acts as a stable platform for the foot during gait. The subtalar joint allows for pronation and supination, critical for absorbing ground reaction forces and adapting to uneven terrain. The calcaneocuboid joint, while possessing limited motion, contributes to the overall flexibility of the transverse tarsal joint. Fusion of these joints, particularly a triple arthrodesis, sacrifices motion for stability and pain relief. Understanding the coupled motions (e.g., subtalar pronation involves calcaneal eversion, abduction, and dorsiflexion; supination involves calcaneal inversion, adduction, and plantarflexion) is crucial for correcting deformities and achieving optimal anatomical alignment during arthrodesis.
Indications & Contraindications
The lateral approach to the hindfoot is indicated for a variety of conditions, predominantly those requiring arthrodesis of the subtalar and/or calcaneocuboid joints, and often in conjunction with talonavicular arthrodesis as part of a triple fusion.
Indications
-
Arthritis:
- Post-traumatic arthritis: Secondary to calcaneal fractures, talar fractures, or subtalar dislocations, leading to pain and dysfunction.
- Primary degenerative osteoarthritis: Isolated to the subtalar or calcaneocuboid joints.
- Inflammatory arthritis: Rheumatoid arthritis, seronegative arthropathies affecting the hindfoot.
-
Deformity Correction:
- Pes cavovarus: Severe, rigid hindfoot varus and forefoot supination, often requiring subtalar and calcaneocuboid arthrodesis with osteotomies.
- Pes planovalgus: Rigid flatfoot deformities, though often requiring a combination of approaches.
- Neuromuscular deformities: Charcot-Marie-Tooth disease, cerebral palsy, or poliomyelitis leading to intractable pain and instability.
- Instability: Chronic subtalar instability refractory to non-operative treatment, often in the setting of ligamentous laxity or previous trauma.
- Failed Previous Surgery: Revision arthrodesis for nonunion or malunion of the subtalar or calcaneocuboid joints.
- Avascular Necrosis: Of the talus or calcaneus, if leading to end-stage joint destruction and pain.
- Sinus Tarsi Syndrome: Though often managed non-operatively, persistent symptoms may warrant exploration, debridement, or denervation via this approach.
-
Select Fractures:
- Certain calcaneal fracture patterns (e.g., tongue-type, specific joint depression patterns) when open reduction and internal fixation is indicated.
- Lateral talar body fractures.
- Irreducible subtalar dislocations.
Contraindications
-
Absolute Contraindications:
- Active infection (osteomyelitis, cellulitis) in the surgical field.
- Severe vascular compromise precluding adequate healing.
- Uncorrected coagulopathy.
- Severe soft tissue compromise (e.g., extensive ulceration, devitalized tissue).
-
Relative Contraindications:
- Mild, non-progressive arthritis or deformity amenable to non-operative management.
- Patients with significant medical comorbidities that increase surgical risk (ASA Class IV or V).
- Severe, uncontrolled diabetes.
- Heavy smoking, which significantly increases nonunion rates.
- Patients unwilling or unable to comply with postoperative rehabilitation protocols.
- Isolated talonavicular arthritis (a medial or dorsal approach is generally preferred for this joint).
Operative vs. Non-Operative Indications
| Indication Category | Operative (Lateral Approach) | Non-Operative |
|---|---|---|
| Arthritis | End-stage, painful arthritis (post-traumatic, degenerative, inflammatory) of subtalar, calcaneocuboid, or talonavicular joints, unresponsive to conservative care. | Mild to moderate arthritis; initial symptoms; managed with NSAIDs, activity modification, custom orthotics, ankle-foot orthoses (AFO), corticosteroid injections, physical therapy. |
| Deformity | Rigid, painful hindfoot deformities (e.g., severe cavovarus or planovalgus) causing functional impairment, gait disturbance, and skin breakdown. | Flexible deformities; mild to moderate symptoms; managed with shoe modifications, orthotics, bracing, physical therapy to improve strength and flexibility. |
| Instability | Chronic, symptomatic subtalar instability refractory to bracing and rehabilitation. | Acute sprains; mild recurrent instability managed with bracing, physical therapy, proprioceptive training. |
| Fractures | Specific calcaneal (e.g., displaced intra-articular) or talar body fractures requiring open reduction and internal fixation for joint reconstruction. | Non-displaced or minimally displaced fractures, stable subtalar dislocations, managed with immobilization (cast/boot) and protected weight-bearing. |
| Avascular Necrosis | End-stage collapse and pain of the talus or calcaneus involving joint destruction. | Early stages, asymptomatic AVN, or those amenable to core decompression if joint integrity is preserved. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are critical steps to ensure optimal exposure, minimize complications, and facilitate a successful surgical outcome.
Pre-Operative Planning
- Clinical Assessment: A comprehensive history and physical examination are essential to fully characterize the patient's symptoms, functional limitations, and deformity. Neurovascular status must be thoroughly assessed.
-
Imaging Review:
- Standard Radiographs: Weight-bearing anteroposterior, lateral, and oblique views of the foot and ankle are mandatory. Specific hindfoot views (e.g., Harris heel view for calcaneal alignment, Canale view for talar neck) may be beneficial. Assess joint space narrowing, osteophytes, subchondral sclerosis, cyst formation, and overall alignment.
- Computed Tomography (CT) Scan: The gold standard for evaluating joint congruity, bone stock, precise fracture patterns (if applicable), and extent of arthritis. 3D reconstructions can be invaluable for understanding complex deformities and planning osteotomies.
- Magnetic Resonance Imaging (MRI): Less commonly used for routine arthrodesis planning but useful for assessing soft tissue pathologies, cartilage status, osteonecrosis, stress fractures, or occult lesions.
- Deformity Analysis: Precisely quantify the degree of varus or valgus, equinus, or abduction/adduction deformity. This dictates the amount and location of corrective osteotomies or bone resection.
- Templating: Use radiographs or CT images to template potential implant sizes and positions (e.g., screw length and trajectory, plate contour). Identify potential hardware conflict or need for specific instrumentation (e.g., low-profile plates).
- Soft Tissue Envelope Assessment: Examine for any skin compromise, edema, or previous incisions that might influence surgical approach or incision placement.
- Bone Grafting Strategy: Determine if local autograft (from calcaneus or iliac crest), allograft, or bone graft substitutes will be required, especially for large defects or revision cases.
Patient Positioning
The lateral approach to the hindfoot is typically performed with the patient in a supine position.
- Operating Table Setup: The patient is positioned supine on the operating table.
- Limb Preparation: The affected limb is prepared and draped to allow full visualization from the proximal calf to the toes, facilitating manipulation of the foot and ankle.
-
Internal Rotation:
To bring the lateral aspect of the hindfoot forward and optimize exposure:
- A large sandbag or bump is placed beneath the affected ipsilateral buttock. This internally rotates the entire lower extremity, making the lateral malleolus and lateral aspect of the hindfoot more accessible.
- Further internal rotation can be achieved by tilting the operating table away from the surgeon.
-
The knee is typically flexed slightly, and the hip externally rotated relative to the internally rotated lower leg to achieve a neutral and stable position of the foot.
Figure 1A: Patient positioned supine on the operating table. A sandbag is placed under the ipsilateral buttock to internally rotate the leg, presenting the lateral aspect of the hindfoot for the approach.
-
Tourniquet Application:
A pneumatic tourniquet is routinely applied to the thigh to facilitate a bloodless surgical field, which is crucial for identifying anatomical structures and minimizing blood loss.
- The limb is exsanguinated either by elevating it for 3-5 minutes or by applying a soft rubber bandage (e.g., Esmarch bandage) prior to tourniquet inflation.
-
Tourniquet pressure is set according to institutional protocols and patient's blood pressure (typically 250-350 mmHg for thigh tourniquets). A distal ankle tourniquet can also be considered for shorter procedures to minimize thigh discomfort, but may limit the ability to extend the incision proximally if needed.
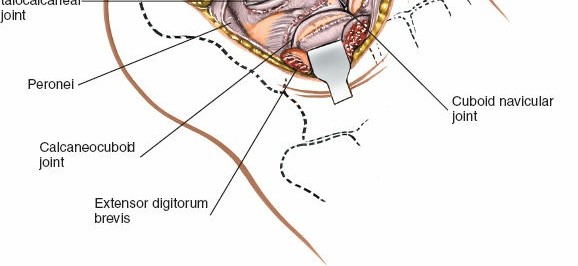
Figure 1B: The limb is exsanguinated using an Esmarch bandage prior to inflation of a pneumatic tourniquet applied to the thigh.
- Sterile Preparation and Draping: The limb is prepped with an antiseptic solution from the mid-calf to the toes, including the ankle joint. Sterile drapes are applied to allow full mobility of the foot and ankle, often using an impermeable stockinette and additional sterile towels.
Detailed Surgical Approach / Technique
The lateral approach to the hindfoot is typically performed with a curvilinear incision centered over the sinus tarsi, extending distally to the calcaneocuboid joint. Careful dissection and anatomical awareness are paramount.
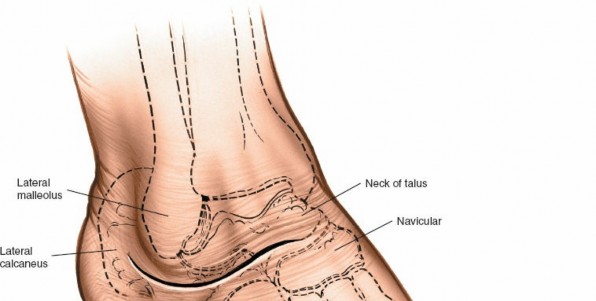
Landmarks and Incision
The relevant palpable landmarks are crucial for accurate incision placement.
* The
lateral malleolus
is the palpable distal end of the fibula.
* The
lateral wall of the calcaneus
is subcutaneous and palpable inferior to the lateral malleolus.
* The
sinus tarsi
is identified as a soft tissue depression just anterior to the lateral malleolus. To palpate, stabilize the foot with one hand, holding the calcaneus, and place the thumb of the free hand in the depression. This depression lies directly over the sinus tarsi.
The most common incision for the lateral approach, particularly for triple arthrodesis, is often referred to as the
Ollier incision
or a modified Ollier incision.
1.
Incision Planning:
A curvilinear incision is made, starting approximately 1.5 cm proximal and posterior to the tip of the lateral malleolus. It curves distally, crossing the sinus tarsi, and continues along the lateral wall of the calcaneus, terminating at the calcaneocuboid joint or the base of the fifth metatarsal. The total length is typically 8-10 cm. The curvature should be gentle to avoid tension at the apex of the incision.

Figure 2A: Anatomic landmarks for the lateral approach to the hindfoot, including the lateral malleolus, calcaneus, and sinus tarsi. The planned curvilinear incision for optimal exposure is marked.
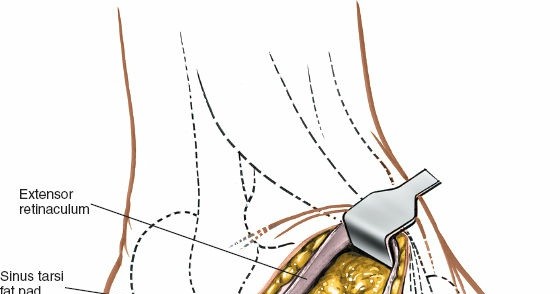
Figure 2B: The planned skin incision extending from the lateral malleolus, curving over the sinus tarsi, and distally towards the calcaneocuboid joint.
Superficial Dissection
-
Skin Incision:
Incise the skin and subcutaneous tissues down to the level of the deep fascia. Use careful hemostasis.
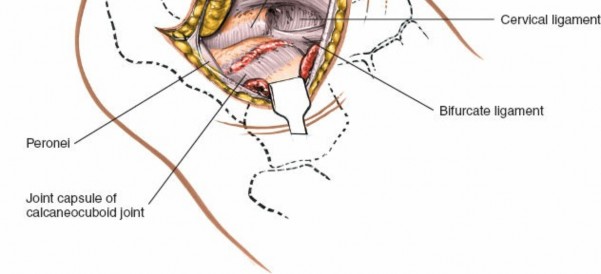
Figure 3A: Initial skin incision performed meticulously with a scalpel, ensuring precise alignment with pre-operative markings.
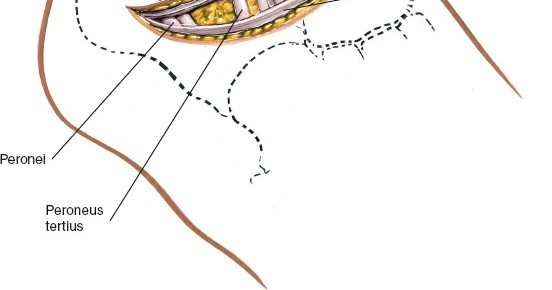
Figure 3B: Deepening the incision through the subcutaneous tissue, exposing the underlying fascia. -
Sural Nerve Identification:
The most critical step in superficial dissection is the identification and protection of the sural nerve. This nerve courses superficial to the deep fascia, typically within the subcutaneous fat, approximately 1-2 cm posterior to the incision line. It should be identified and carefully retracted either superiorly or inferiorly, away from the operative field. Avoid aggressive retraction, which can lead to neuropraxia.
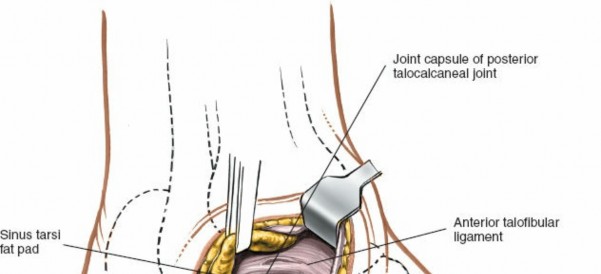
Figure 4A: Identification of the sural nerve (yellow loop) within the subcutaneous fat layer, often posterior to the main incision. This nerve must be carefully protected.
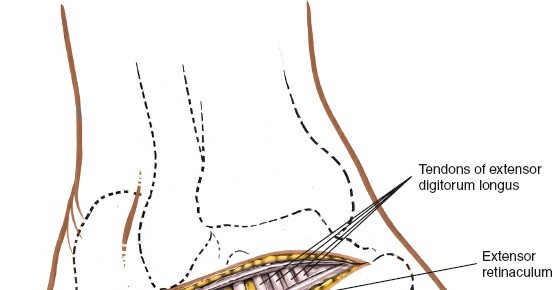
Figure 4B: The sural nerve is retracted gently using a vessel loop or similar instrument to prevent injury during deeper dissection. - Deep Fascia Incision: Once the sural nerve is protected, incise the deep fascia longitudinally, parallel to the skin incision. This exposes the underlying muscle and tendon structures.
Deep Dissection and Exposure
-
Peroneal Tendons and Retinaculum:
The peroneus brevis and longus tendons, encased in their common sheath, lie posterior to the surgical corridor. The inferior peroneal retinaculum courses obliquely over the tendons.
-
Incise the retinaculum and carefully retract the peroneal tendons posteriorly using a blunt retractor (e.g., Hohmann). This exposes the lateral wall of the calcaneus.

Figure 5A: After fascial incision, the peroneal tendons (peroneus longus and brevis) are identified and carefully retracted posteriorly, exposing the lateral wall of the calcaneus.
-
Incise the retinaculum and carefully retract the peroneal tendons posteriorly using a blunt retractor (e.g., Hohmann). This exposes the lateral wall of the calcaneus.
-
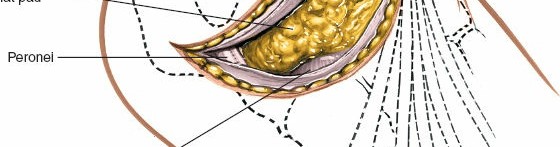
Extensor Digitorum Brevis (EDB) Muscle:
The EDB muscle originates from the anterior superior aspect of the calcaneus within the sinus tarsi. It lies anterior to the peroneal tendons.
-
Elevate the EDB muscle subperiosteally from its origin on the calcaneus using an elevator (e.g., periosteal elevator or Cobb). Retract the EDB muscle and its associated neurovascular bundle (deep peroneal nerve branch, anterior tibial artery branch) anteriorly/dorsally. This provides excellent exposure of the sinus tarsi and the capsules of the subtalar and calcaneocuboid joints.
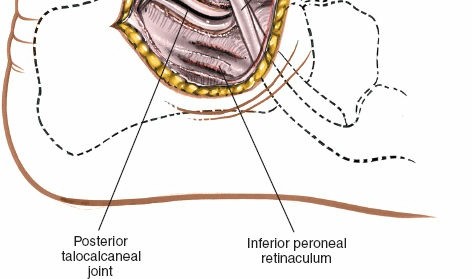
Figure 5B: The extensor digitorum brevis muscle is elevated subperiosteally from its origin on the calcaneus and retracted dorsally/anteriorly, revealing the contents of the sinus tarsi.
-
Elevate the EDB muscle subperiosteally from its origin on the calcaneus using an elevator (e.g., periosteal elevator or Cobb). Retract the EDB muscle and its associated neurovascular bundle (deep peroneal nerve branch, anterior tibial artery branch) anteriorly/dorsally. This provides excellent exposure of the sinus tarsi and the capsules of the subtalar and calcaneocuboid joints.
- Sinus Tarsi and Joint Capsules: With the EDB retracted, the floor of the sinus tarsi is visible, revealing the interosseous talocalcaneal ligament and cervical ligament. The capsules of the subtalar and calcaneocuboid joints are now accessible.
Joint Preparation for Arthrodesis
The goal for arthrodesis is to remove all articular cartilage and subchondral bone down to bleeding cancellous bone, creating a raw surface for fusion. The sequence of joint preparation is critical.
-
Subtalar Joint Preparation:
- Perform a capsulotomy of the subtalar joint.
- Incise and resect the interosseous talocalcaneal ligament and cervical ligament using osteotomes, curettes, or small rongeurs. Complete resection of these ligaments is essential to allow adequate joint distraction and correction of deformity.
- Use oscillating saws, osteotomes, and curettes to meticulously remove all articular cartilage from the talar and calcaneal facets. Ensure removal extends to all three facets (anterior, middle, posterior) if a complete subtalar fusion is intended.
- Be mindful of the posterior facet's obliquity. Preserve as much bone stock as possible, only removing enough to expose healthy cancellous bone.
-
A laminar spreader or a small distractor can be used to open the joint space for better visualization and debridement. This also helps in correcting any varus/valgus deformity.
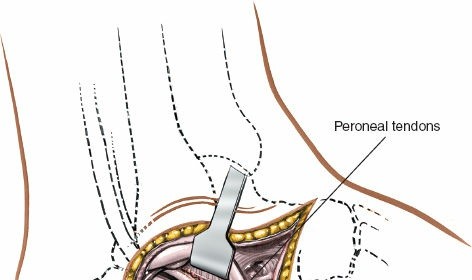
Figure 6A: The subtalar joint capsule has been incised, and the interosseous talocalcaneal ligament resected. Articular cartilage is being removed from the talar and calcaneal surfaces using an oscillating saw.

Figure 6B: Further debridement of the articular surfaces of the subtalar joint, exposing bleeding cancellous bone. A laminar spreader can assist in joint distraction for thorough preparation.
-
Calcaneocuboid Joint Preparation:
- Perform a capsulotomy of the calcaneocuboid joint.
-
Resect articular cartilage from the anterior calcaneal and posterior cuboid surfaces. This is typically straightforward from the lateral approach.
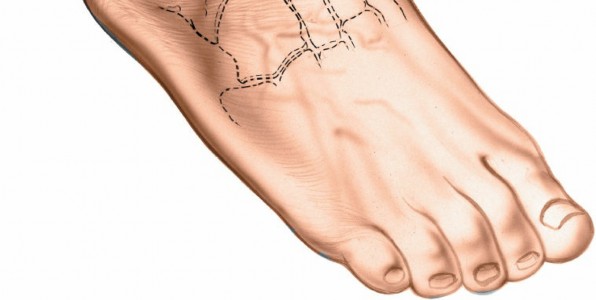
Figure 7A: The calcaneocuboid joint is exposed, and articular cartilage is being removed from its surfaces using an osteotome or saw.
-
Talonavicular Joint Preparation (for Triple Arthrodesis):
- Access to the talonavicular joint from a purely lateral approach is challenging but feasible, particularly after the subtalar and calcaneocuboid joints are prepared and the foot can be manipulated. Strong inversion and plantarflexion of the midfoot may improve access.
- Often, the lateral approach is extended more dorsally, or a small separate anterolateral incision may be considered to directly address the talonavicular joint, especially if significant deformity correction is needed at this joint.
- Resect the calcaneonavicular component of the bifurcate ligament if necessary for exposure.
- Remove articular cartilage from the talar head and navicular facet. Correct any midfoot abduction/adduction deformity by resecting appropriate wedges.
Deformity Correction, Reduction, and Fixation
-
Deformity Correction:
Address any pre-existing hindfoot deformity (e.g., varus or valgus).
- For cavovarus feet , a lateral closing wedge osteotomy of the calcaneus (removing more bone laterally) or a medial opening wedge can correct varus.
- For planovalgus feet , a lateral opening wedge or medial closing wedge might be considered, though a medial approach is often more direct for planovalgus reconstruction.
- Careful intraoperative fluoroscopy is essential to ensure proper alignment in all planes (AP, lateral, and axial heel views).
-
Bone Grafting:
After joint preparation and deformity correction, the joint spaces may contain gaps. Fill these with autograft (harvested from the calcaneal body or distal tibia) or allograft chips to promote fusion.
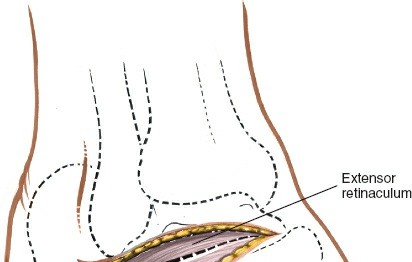
Figure 8A: Bone graft material (autograft or allograft chips) is packed into the prepared joint spaces to enhance fusion. - Temporary Fixation: Use K-wires to temporarily stabilize the joints in the desired anatomical position. Confirm alignment with fluoroscopy.
-
Definitive Fixation:
- Subtalar Joint: Typically fixed with one or two large cancellous screws (e.g., 6.5 mm or 7.3 mm). Screws are usually placed from the posterior calcaneus, crossing the subtalar joint into the talar body. Alternatively, they can be placed from the talar neck into the calcaneus, or from the lateral calcaneal wall into the talus. A lateral compression plate can also be used, especially in osteoporotic bone or for additional stability.
- Calcaneocuboid Joint: Fixed with one or two cancellous screws, often oriented from the cuboid into the calcaneus or vice versa. A small plate on the lateral aspect can also provide robust fixation.
- Talonavicular Joint (if applicable): Fixed with one or two small cancellous screws, typically from the navicular into the talar head, or from the talar neck into the navicular.
-
Triple Arthrodesis Fixation Sequence:
Often the subtalar joint is fixed first, followed by the calcaneocuboid, and then the talonavicular. This sequence allows for stepwise correction and stabilization.

Figure 9A: Definitive internal fixation of the subtalar and calcaneocuboid joints using cancellous screws. Fluoroscopic guidance is essential to confirm screw placement and joint alignment.

Figure 9B: Final intraoperative fluoroscopic image demonstrating optimal screw placement across the subtalar and calcaneocuboid joints, confirming satisfactory alignment and reduction.
Wound Closure
- Irrigation: Thoroughly irrigate the wound with sterile saline.
- Muscle and Fascia: Reapproximate the extensor digitorum brevis muscle over the sinus tarsi region if possible without tension. Close the deep fascia, if substantial, with absorbable sutures.
- Subcutaneous Layer: Close the subcutaneous fat layer using inverted absorbable sutures to reduce dead space and tension on the skin.
- Skin Closure: Close the skin with non-absorbable sutures or staples.
- Dressing and Splint: Apply a sterile dressing. A well-padded plaster or fiberglass splint (e.g., posterior slab with sugar tong) is applied, maintaining the hindfoot in a neutral position to protect the fusion sites and prevent early motion.
Complications & Management
Despite meticulous surgical technique, complications can arise following a lateral hindfoot approach and subsequent arthrodesis. Awareness of these and prompt, appropriate management are crucial for salvage.
Common Complications and Salvage Strategies
| Complication | Incidence | Management / Salvage Strategy |
|---|---|---|
| Nonunion / Malunion | Variable; 5-20% for triple arthrodesis, higher in smokers/revisions. | Nonunion: Revision arthrodesis with robust debridement, bone grafting (autograft preferred), rigid internal fixation (often plating). Consider electrical stimulation or BMP. Malunion: Corrective osteotomy and revision arthrodesis. |
| Infection | <5% (superficial), <2% (deep) | Superficial: Oral antibiotics, local wound care. Deep: Surgical irrigation and debridement, intravenous antibiotics, hardware retention if stable and infection controlled, or removal if unstable/persistent. May require staged reconstruction. |
| Sural Nerve Injury | 10-20% (neuropraxia), <5% (permanent neuroma) | Neuropraxia: Conservative management (observation, NSAIDs, nerve gliding exercises). Neuroma: Excision of neuroma and nerve relocation, or grafting if a gap exists. May require neurolysis. |
| Wound Dehiscence / Soft Tissue Necrosis | <5% | Local wound care, serial debridement. If significant, may require wound VAC, local flap coverage (e.g., reverse sural flap), or free flap reconstruction. |
| Hardware Irritation | 5-10% | Typically managed with hardware removal after documented fusion, usually 12-18 months post-op. |
| Complex Regional Pain Syndrome (CRPS) | <2% | Multimodal approach: early diagnosis, physical therapy, neuropathic pain medications (gabapentin, pregabalin), regional nerve blocks, sympathetic blocks, psychological support. Referral to pain management specialist. |
| Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE) | <1% (with prophylaxis) | DVT: Anticoagulation. PE: Emergency anticoagulation, supportive care. Prevention with pharmacologic (lovenox, aspirin) and mechanical (SCDs) prophylaxis is critical. |
| Adjacent Joint Arthritis | 20-40% over 10-20 years (post-triple arthrodesis) | Non-operative management initially (NSAIDs, orthotics, injections). If refractory, fusion of the adjacent joint (e.g., ankle arthrodesis after triple arthrodesis) or joint replacement (rarely indicated in the hindfoot due to high failure rates). |
| Implant Malposition / Breakage | Rare | Malposition: Revision surgery for repositioning or removal of symptomatic hardware. Breakage: May indicate nonunion or excessive load. Revision arthrodesis and hardware exchange are typically required. |
| Neurovascular Injury (other) | Very rare (deep peroneal nerve, vascular) | Immediate exploration and repair if identified intraoperatively. Post-operative deficits require neurological consultation and potential referral for nerve repair. |
Specific Considerations
- Tobacco Use: Smoking cessation is paramount pre-operatively and post-operatively, as it is a major independent risk factor for nonunion and wound complications.
- Bone Quality: Osteoporosis increases the risk of implant failure and nonunion. Careful bone preparation, robust fixation (e.g., locking plates, cement augmentation), and systemic management of osteoporosis are important.
- Systemic Illnesses: Patients with diabetes, rheumatoid arthritis, or other inflammatory conditions have a higher risk of complications and slower healing. Aggressive management of these underlying conditions is vital.
- Revision Surgery: Patients undergoing revision arthrodesis for nonunion have significantly higher complication rates and lower success rates compared to primary fusions. Extensive debridement and potent biological augmentation are often required.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following a lateral hindfoot approach, particularly after arthrodesis, is critical for achieving successful fusion, protecting the surgical repair, and optimizing long-term functional outcomes. Protocols vary based on the procedure performed (e.g., simple debridement vs. multi-joint arthrodesis), bone quality, and surgeon preference, but generally follow a structured, progressive approach.
General Principles
- Protection: The primary goal in the early phase is to protect the fusion site and allow for biologic healing.
- Non-Weight Bearing (NWB): Essential in the initial phase to prevent excessive stress on the fusion.
- Elevation & Edema Control: Crucial to minimize swelling, which can compromise wound healing and delay rehabilitation.
- Gradual Progression: Weight-bearing, range of motion (ROM), and strengthening are advanced incrementally based on clinical and radiographic evidence of healing.
Phase 1: Immediate Post-Operative (Weeks 0-6)
-
Immobilization:
- Day 0-14: Initial well-padded posterior splint and sugar tong splint (or similar) to provide rigid immobilization in a neutral position.
- Week 2-6: Conversion to a non-weight-bearing cast (e.g., short leg cast) or a controlled ankle motion (CAM) boot locked at neutral.
- Weight Bearing: Strict non-weight bearing (NWB) on the operative extremity. Ambulation with crutches or a knee scooter.
-
Activity:
- Strict elevation of the limb above heart level (especially for the first 1-2 weeks) to control edema.
- Gentle ankle dorsiflexion/plantarflexion (if ankle not fused) and toe wiggles while in splint/cast to promote circulation.
- No active or passive range of motion of the fused joints.
- Wound Care: Monitor incision for signs of infection or dehiscence. Dressing changes as per protocol. Suture/staple removal at 2-3 weeks.
- Pain Management: Opioid and non-opioid analgesics, nerve blocks as needed.
Phase 2: Early Healing & Gradual Weight Bearing (Weeks 6-12)
- Clinical Assessment: Evaluate wound healing. Radiographs obtained at week 6 to assess for early signs of fusion (bridging callus, obliteration of joint space).
- Immobilization: Continue with CAM boot or cast, typically worn full-time.
-
Weight Bearing Progression:
- Week 6-8: Begin touch-down weight bearing (TDWB) to 25% weight bearing in a CAM boot or walking cast, as tolerated and only if radiographs show adequate healing.
- Week 8-12: Progress to 50% weight bearing in a CAM boot or walking cast, then to full weight bearing (FWB) as pain and radiographic healing allow.
-
Activity:
- Continue elevation as needed for edema.
- Initiate gentle range of motion exercises for the ankle and forefoot (if not fused), avoiding stress on the fused joints.
- Initiate isometric strengthening of thigh and hip musculature.
- Physical Therapy: May begin formal physical therapy focusing on gait training with assistive devices, balance, and proprioception as weight-bearing progresses.
Phase 3: Advanced Healing & Strengthening (Weeks 12-24)
- Clinical Assessment: Serial radiographs (every 4-6 weeks) to monitor fusion progress. Clinical examination for tenderness, swelling, and stability.
-
Immobilization:
- Discontinue CAM boot/cast if radiographic fusion is confirmed. Transition to supportive shoe wear with an orthosis (e.g., custom molded orthotic, ankle brace) as needed.
- Weight Bearing: Full weight bearing.
-
Physical Therapy:
Intensive rehabilitation focused on:
- Gradual progression of strengthening exercises for the entire lower extremity.
- Balance and proprioceptive training.
- Gait mechanics retraining.
- Endurance activities (e.g., stationary bike, elliptical, swimming).
- Progressive return to activities of daily living (ADLs).
- Activity: Avoid high-impact activities, running, or jumping until 6 months post-op and only with definitive radiographic fusion and clinical clearance.
Phase 4: Long-Term Recovery & Return to Activity (Months 6+)
- Clinical Assessment: Final radiographic assessment of fusion. Evaluation of any residual pain or functional deficits.
-
Activity:
- Gradual return to desired recreational activities, guided by pain and functional tolerance. High-impact sports may be restricted or modified long-term.
- Ongoing use of supportive footwear and custom orthotics is often recommended.
- Patient Education: Long-term implications of hindfoot fusion, including potential for adjacent joint arthritis, should be discussed.
- Maintenance: Continue home exercise program for strength and flexibility.
Important Notes:
*
Individualization:
Protocols must be individualized based on patient factors (age, comorbidities, bone quality), surgeon preference, and intraoperative findings.
*
Radiographic Evidence:
Progression from NWB to FWB should always be guided by clinical assessment and radiographic evidence of healing. Premature weight-bearing is a significant risk factor for nonunion.
*
Pain Management:
Chronic pain management strategies may be necessary for some patients, especially those with pre-existing complex regional pain syndrome or significant psychosocial factors.
Summary of Key Literature / Guidelines
The lateral approach to the hindfoot, particularly for arthrodesis, is a well-established procedure supported by decades of clinical research. Key literature and guidelines focus on surgical indications, techniques, and outcomes, with an emphasis on achieving durable fusion and functional improvement.
-
Triple Arthrodesis Outcomes: Numerous studies have demonstrated the efficacy of triple arthrodesis (talocalcaneal, calcaneocuboid, and talonavicular fusions) for correcting rigid hindfoot deformities and relieving pain from end-stage arthritis.
- Fusion Rates: Historically, fusion rates for triple arthrodesis range from 85% to 95% in primary cases. Factors affecting nonunion include smoking, corticosteroid use, revision surgery, and significant bone loss.
- Functional Outcomes: While motion is sacrificed, patients typically report significant pain relief and improved stability, leading to better walking ability and quality of life. Long-term follow-up studies (20+ years) show durable results for pain relief and function.
- Adjacent Joint Arthritis (AJA): A recognized long-term sequela, with studies reporting AJA in the ankle or midtarsal joints in 20-40% of patients over 10-20 years. This is thought to be due to increased stress and altered biomechanics in the unfused joints. The ankle joint is most commonly affected.
-
Subtalar Arthrodesis Outcomes: Isolated subtalar fusion is effective for isolated subtalar arthritis or instability.
- Fusion Rates: Similar to triple arthrodesis, fusion rates generally exceed 90%.
- Functional Impact: Patients experience improved pain and stability, but some compensatory motion may occur at the ankle and midfoot.
- AJA: Adjacent ankle arthritis is a concern, though perhaps less pronounced than after triple arthrodesis.
-
Fixation Methods: A variety of fixation techniques are employed, with cannulated screws being the most common.
- Screws: Multiple parallel screws provide compression and rotational stability. The typical configuration involves two or three large fragment cancellous screws across the subtalar joint (often posterior-to-anterior into the talus), and one or two across the calcaneocuboid joint.
- Plates: Low-profile lateral plates, particularly those designed for hindfoot arthrodesis, offer rigid construct stability, which can be advantageous in osteoporotic bone, large defects, or revision cases. Plates often supplement screws.
- Intramedullary Nails: Primarily used for ankle-hindfoot fusions but can be used for subtalar fusion with extension into the tibia. Not typically the primary fixation for isolated subtalar or triple arthrodesis via a lateral approach.
- Evidence: Comparative studies have not consistently shown a significant difference in fusion rates between screw-only and screw-plus-plate constructs, but plates may offer superior biomechanical stability in certain settings.
-
Bone Grafting: The role of bone grafting to enhance fusion is widely accepted.
- Autograft: Autogenous bone graft, particularly from the ipsilateral calcaneus or distal tibia, remains the gold standard due to its osteoconductive, osteoinductive, and osteogenic properties.
- Allograft & Substitutes: Allograft (demineralized bone matrix, cancellous chips) and synthetic bone graft substitutes (calcium phosphate, calcium sulfate) are used, often as extenders or standalone agents, especially if autograft harvest is undesirable or limited. The evidence for their equivalence to autograft is evolving, with many studies suggesting acceptable fusion rates but potentially slightly lower than autograft.
-
Complication Rates:
- Nonunion: The most common major complication, consistently reported as higher in smokers and those with systemic comorbidities.
- Sural Neuroma: A frequent, though often temporary, complication due to the superficial course of the sural nerve. Meticulous soft tissue handling and careful nerve retraction are critical.
- Wound Complications: Rates are generally low but are elevated in patients with diabetes, peripheral vascular disease, or poor soft tissue envelopes.
-
Evolving Concepts:
- Minimally Invasive Approaches: While challenging for multi-joint arthrodesis, percutaneous or arthroscopic assistance for subtalar fusion may be considered in select cases to minimize soft tissue dissection.
- Biologics: The use of platelet-rich plasma (PRP) or bone morphogenetic proteins (BMPs) is still under investigation, with varying evidence for their benefit in routine hindfoot arthrodesis. Their role is often reserved for high-risk patients or revision cases.
- Deformity Correction Principles: A growing emphasis on achieving optimal anatomical alignment through meticulous pre-operative planning and intraoperative fluoroscopic guidance. This includes correcting varus/valgus, equinus, and translational deformities to improve long-term outcomes and reduce AJA.
In summary, the lateral approach to the hindfoot is a robust and effective surgical pathway for addressing complex hindfoot pathologies. Its success hinges on a profound understanding of surgical anatomy, meticulous technique, appropriate patient selection, and comprehensive post-operative management, all supported by a strong foundation of clinical evidence.
Clinical & Radiographic Imaging

You Might Also Like


