Complex Post-Traumatic Ankle Arthritis: Deformity, Malunion & Nonunion Management

Key Takeaway
Severe post-traumatic ankle arthritis stemming from an old fracture often presents with chronic pain, limited ROM, and deformity. Imaging reveals tricompartmental joint space narrowing, significant osteophyte formation, fibular nonunion, malunion of malleoli, chronic syndesmosis diastasis, and hindfoot varus. Pre-operative CT templating is crucial for complex deformity correction.
Patient Presentation & History
A 65-year-old male presents with chronic, progressively worsening right ankle pain and functional limitation, which has acutely exacerbated over the past six months following a minor ground-level fall. He reports a history of a right ankle fracture sustained 33 years prior, at the age of 32, following a motorcycle accident. At that time, the fracture was managed non-operatively with a long leg cast for 8 weeks, with no documented radiographic follow-up or formal rehabilitation. He recalls persistent swelling and occasional pain for many years following the initial injury but generally managed with activity modification. Over the last decade, pain has become more constant, significantly limiting his ambulation distance and requiring regular analgesics.
His current symptoms include severe, sharp pain in the right ankle with weight-bearing and ambulation, particularly on uneven surfaces. He experiences stiffness in the morning, which improves slightly with activity but worsens significantly by the end of the day. There is an associated sensation of instability and mechanical catching. He has resorted to using a cane for ambulation.
Relevant medical history includes well-controlled hypertension and Type 2 Diabetes Mellitus. He is a current smoker (15 pack-years), and his social history reveals an active lifestyle pre-injury, now severely curtailed. His primary occupation requires prolonged standing and walking.
Clinical Examination
Upon inspection of the right ankle, significant global swelling is noted, with evidence of chronic skin changes including a slightly hyperpigmented, thickened appearance over the anterior and lateral aspects. There is a palpable, diffuse prominence of the lateral malleolus. Gait analysis reveals a pronounced antalgic gait with reduced stance phase on the right, accompanied by a noticeable varus thrust at the ankle during weight-bearing. He uses a cane for support.
Palpation elicits diffuse tenderness along the ankle joint line, particularly anteromedially and anterolaterally. There is exquisite tenderness over the lateral malleolus, suggesting potential nonunion or severe osteophytic changes. A moderate joint effusion is present. Crepitus is palpable with passive motion. Distal pulses (dorsalis pedis, posterior tibial) are 2+ bilaterally, and capillary refill is brisk. Sensation is intact in all dermatomes distal to the ankle. There are no signs of active infection or skin breakdown.
Active and passive range of motion (ROM) is severely restricted and painful. Dorsiflexion is limited to 0-5 degrees (normal 20 degrees), plantarflexion to 10-15 degrees (normal 45 degrees). Inversion and eversion are almost entirely absent, with fixed hindfoot varus deformity evident. Subtalar motion is also notably restricted. He is unable to perform a single heel raise due to pain and weakness. Neurological examination of the lower extremity is otherwise unremarkable, ruling out overt nerve impingement.
Imaging & Diagnostics
Radiographs
Initial weight-bearing radiographs of the right ankle (AP, Mortise, Lateral views) demonstrated:
*
AP View:
Severe tibio-talar joint space narrowing, most pronounced medially, consistent with advanced tricompartmental post-traumatic ankle arthritis. Significant osteophyte formation along the anterior and medial joint margins. Varus talar tilt of approximately 12 degrees. Lateral malleolar nonunion with sclerotic fracture margins and significant fibular shortening (approximately 1.5 cm) relative to the distal tibia. Diastasis of the distal tibiofibular syndesmosis with lateral talar shift.
*
Mortise View:
Complete obliteration of the medial clear space and widening of the lateral clear space. Incongruity of the talar dome within the mortise, indicative of syndesmotic instability and chronic lateral talar shift.
*
Lateral View:
Significant anterior osteophyte formation (tibial spurring, "kissing" talar dome osteophyte). Dorsiflexion restriction due to anterior impingement. Subchondral sclerosis and cystic changes in both the distal tibia and talus. Posterior malleolar malunion with mild posterior displacement of the talus.
Computed Tomography (CT) Scan
A non-contrast CT scan of the right ankle was performed to further delineate the bony architecture, extent of articular destruction, and characteristics of the lateral malleolar nonunion.
*
Articular Surface:
Confirming severe tricompartmental chondral loss, subchondral cyst formation, and sclerosis of the distal tibial plafond and talar dome.
*
Deformity Analysis:
Quantified hindfoot varus deformity (12 degrees), fibular shortening (1.5 cm), and rotational malalignment of the fibula. Malunion of the posterior malleolus was confirmed with approximately 3 mm of posterior translation and angular deformity.
*
Nonunion Site:
The lateral malleolar fracture demonstrated a sclerotic nonunion with a small gap and no bridging callus, consistent with an oligotrophic nonunion. Significant bone loss was not evident at the fibular nonunion site.
*
Syndesmosis:
Chronic tibiofibular diastasis and heterotopic ossification within the interosseous membrane.

Magnetic Resonance Imaging (MRI)
An MRI was not primarily indicated for this advanced bony pathology but could have been considered if significant soft tissue concerns (e.g., tendon rupture, osteonecrosis not evident on CT) were suspected. Given the clear radiographic and CT findings of severe post-traumatic arthritis and malunion/nonunion, the MRI was deferred in favor of direct surgical planning.
Templating
Pre-operative templating using high-resolution CT images and radiographs was crucial.
*
Deformity Correction:
Identification of precise osteotomy planes for fibular lengthening and correction of hindfoot varus.
*
Bone Grafting:
Assessment of potential bone void after debridement and correction, necessitating autogenous bone graft.
*
Implant Selection:
Provisional sizing for a retrograde intramedullary nail (Tibiotalocalcaneal Arthrodesis – TTC fusion) given the severe deformity, bone loss, and need for robust fixation. Also, planning for ancillary screw fixation.
Differential Diagnosis
The patient's presentation of long-standing pain, deformity, and functional limitation following a remote ankle fracture, along with characteristic imaging findings, strongly points towards severe post-traumatic ankle arthritis with associated malunion and nonunion. However, it is essential to consider other pathologies that might present similarly or coexist.
| Feature | Post-Traumatic Ankle Arthritis with Malunion (Primary Diagnosis) | Ankle Nonunion (e.g., Lateral Malleolus with Instability) | Osteochondral Lesion of the Talus (OCLT) | Inflammatory Arthritis (e.g., Rheumatoid) |
|---|---|---|---|---|
| Onset | Gradual, progressive pain years after initial trauma | Persistent pain/instability post-injury; failure to unite | Often acute injury leading to chronic localized pain/clicking | Insidious, often symmetric joint involvement, systemic symptoms |
| Pain Characteristics | Diffuse ankle pain, worse with activity/weight-bearing, stiffness, mechanical symptoms | Localized pain over nonunion site, instability, persistent swelling | Localized pain, deep aching, catching, locking, effusions | Polyarticular pain, morning stiffness >30min, symmetrical swelling |
| Swelling | Generalized ankle swelling, synovitis | Localized swelling, can be generalized if chronic | Intermittent, often after activity | Symmetrical, warm, boggy joints |
| Deformity | Common (varus/valgus malalignment), limited ROM, fibular malunion/nonunion | Localized deformity, instability (e.g., fibular shortening), malunion | Rare, limited ROM if large lesion or degenerative changes occur | Joint destruction, subluxation, classic deformities (e.g., swan neck) |
| Imaging (X-ray) | Joint space narrowing, osteophytes, subchondral sclerosis, cysts, malalignment, nonunion | Sclerotic nonunion margins, gap, implant failure (if operated), malunion | May be subtle; subchondral lucency or sclerosis, loose body | Erosions, joint space narrowing, soft tissue swelling, osteopenia |
| Imaging (CT) | Gold standard for bone morphology, joint congruity, malunion assessment | Defines nonunion gap, bone loss, viability of fragments | Defines lesion size, depth, subchondral involvement | Joint destruction, subluxation, periarticular erosions |
| Imaging (MRI) | Synovitis, chondral damage, tendon pathology | Soft tissue interposition, bone marrow edema, vascularity | Defines cartilage integrity, subchondral edema, cyst formation, instability | Synovitis, erosions, bone marrow edema, tenosynovitis |
| History | Remote ankle fracture/trauma (e.g., 33 years prior) | Previous ankle fracture surgery or non-operative management | Ankle sprain or direct trauma | Systemic symptoms, family history, involvement of other joints |
| Treatment Implications | Salvage procedures (arthrodesis, arthroplasty), deformity correction | Revision ORIF, bone grafting, deformity correction | Debridement, microfracture, OATS, ACI | Medical management (DMARDs), joint-specific surgery for salvage |
Surgical Decision Making & Classification
Rationale for Operative Intervention
The decision for operative intervention was based on several critical factors:
1.
Failure of Conservative Management:
The patient had exhausted all non-operative modalities, including NSAIDs, activity modification, bracing, and local injections, with no sustained improvement in pain or function.
2.
Severe Pain and Functional Limitation:
His pain was debilitating, significantly impacting his quality of life, ambulation, and ability to perform his occupation.
3.
Advanced Post-Traumatic Ankle Arthritis (PTAA):
Imaging demonstrated severe, tricompartmental joint destruction with significant osteophyte formation and subchondral changes.
4.
Complex Deformity and Instability:
The combination of fibular nonunion, fibular shortening, chronic syndesmotic diastasis, and significant hindfoot varus led to persistent mechanical instability and altered joint biomechanics, accelerating degenerative changes.
5.
Age and Activity Level:
Despite his age, the patient was otherwise medically optimized and desired to return to a more active lifestyle, making salvage surgery a viable option.
Classification and Surgical Plan
Given the severe, end-stage PTA, complex deformity (varus malalignment, fibular shortening/nonunion), and patient's high demand, a Tibiotalocalcaneal (TTC) Arthrodesis with fibular reconstruction and bone grafting was selected as the most appropriate surgical solution. This procedure provides robust stability, corrects deformity, and eliminates the painful joint motion, offering predictable pain relief and functional improvement in severe cases. Total Ankle Arthroplasty (TAA) was considered but deemed less suitable due to the severe deformity, significant bone loss, chronic syndesmotic instability, and the presence of a lateral malleolar nonunion, which would complicate implant alignment and longevity.
Specific aspects of the surgical plan included:
1.
Fibular Nonunion Management:
Excision of sclerotic nonunion fragments, freshening of bone ends, and primary union with bone graft and plate fixation to restore fibular length and rotational alignment. This is crucial for mortise stability and to address the underlying cause of lateral talar shift.
2.
Deformity Correction:
Resection of articular cartilage and subchondral bone from the distal tibia, talus, and superior aspect of the calcaneus, followed by meticulous alignment correction in all planes (neutral dorsiflexion, 5-7 degrees of hindfoot valgus, neutral rotation).
3.
Bone Grafting:
Autogenous cancellous bone graft, harvested from the ipsilateral iliac crest, to fill bone defects and promote fusion.
4.
Internal Fixation:
Retrograde intramedullary (IM) nail for a TTC fusion, providing superior stability and compression, particularly advantageous in cases with significant bone loss, poor bone quality, or complex deformity.
Surgical Technique / Intervention
Patient Positioning and Preparation
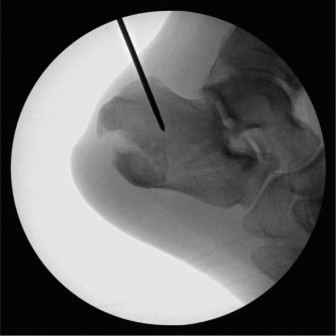
The patient was positioned supine on a radiolucent table. A thigh tourniquet was applied. All bony prominences were meticulously padded. A bolster was placed under the ipsilateral hip to allow for full internal rotation of the limb for optimal imaging of the hindfoot. The entire limb was prepped and draped in a sterile fashion from the mid-thigh to the toes. Image intensification was readily available and positioned to allow for AP, lateral, and oblique views of the ankle and hindfoot.
Approach and Debridement
- Fibular Reconstruction: A standard curvilinear incision was made along the posterior border of the fibula. The fibular nonunion site was exposed. Sclerotic bone ends were resected and freshened back to bleeding bone. A small amount of corticotomy was performed to allow for lengthening. An autogenous bone graft (iliac crest) was packed into the nonunion gap. A reconstruction plate (e.g., 1/3 tubular plate or specific fibular plating system) was applied to achieve length restoration and stable fixation of the fibula.
-
TTC Fusion:
A straight anterior incision was made, centered over the tibio-talar joint. Dissection was carried down through subcutaneous tissue, carefully protecting the superficial peroneal nerve branches and neurovascular structures. The anterior capsule was incised, and the ankle joint was exposed. Osteophytes, hypertrophic synovium, and remnants of articular cartilage were meticulously débrided from the distal tibia and talar dome. Similarly, a separate posterolateral approach or a medial approach might be required to adequately debride the subtalar joint and correct hindfoot deformity. For this case, a medial approach was used for calcaneal preparation.
- Joint Preparation: A lamina spreader was used to distract the ankle and subtalar joints. The cartilage was removed down to bleeding subchondral bone using oscillating saws, osteotomes, and curettes. Care was taken to preserve as much subchondral bone as possible while achieving broad, cancellous bone apposition surfaces.
- Deformity Correction: The hindfoot varus deformity was corrected by careful bone resection and precise alignment. The goal was to achieve a neutral ankle dorsiflexion, neutral rotation, and approximately 5-7 degrees of hindfoot valgus for optimal weight distribution and gait mechanics. This often involves wedge resections or differential bone removal.
Fixation Construct (Retrograde Tibiotalocalcaneal Nailing)
- Entry Point: A longitudinal incision was made on the plantar aspect of the heel, centered between the calcaneal tuberosities, just anterior to the weight-bearing fat pad. The calcaneal entry point for the intramedullary nail was established using an awl.
- Reaming: A guide wire was inserted into the calcaneus, through the talus, and into the medullary canal of the tibia. This was meticulously guided under fluoroscopic control to ensure proper trajectory and central placement. Sequential reaming was performed over the guide wire to the appropriate diameter, typically 10-13 mm, across the calcaneus, talus, and into the tibial medullary canal.
- Nail Insertion: The appropriately sized retrograde IM nail was selected and inserted over the guide wire, extending proximally into the tibia and distally into the calcaneus. The nail was advanced until it was flush or slightly recessed from the calcaneal plantar surface.
- Locking Screws: Distal locking screws were inserted from medial to lateral across the calcaneus and talus, engaging both cortices. Proximal locking screws were inserted across the distal tibia. Static locking was preferred to provide maximum rotational stability and compression across the fusion sites.
- Compression: Compression was applied across the fusion sites using the integrated compression mechanism of the IM nail, further enhancing stability and promoting union.
- Bone Grafting: Autogenous cancellous bone graft, harvested from the ipsilateral posterior iliac crest, was packed liberally into all joint spaces and around the fibular nonunion site to augment healing.
- Closure: Meticulous layered closure was performed, paying careful attention to subcutaneous tissue and skin to minimize wound complications. A sterile dressing and a well-padded splint were applied.
Post-Operative Protocol & Rehabilitation
Immediate Post-Operative Period (Weeks 0-6)
- Immobilization: The ankle was immobilized in a non-weight-bearing (NWB) posterior splint for 2 weeks, then transitioned to a NWB short leg cast or CAM boot.
- Weight-Bearing: Strictly non-weight-bearing on the operative limb.
- Elevation & Pain Management: Continuous elevation of the limb to reduce swelling. Aggressive pain management, including multimodal analgesia.
- DVT Prophylaxis: Pharmacological DVT prophylaxis (e.g., LMWH) was initiated and continued for 4-6 weeks.
- Wound Care: Close monitoring of the surgical incisions for signs of infection or dehiscence. Suture removal at 2-3 weeks post-op.
- Rehabilitation: Gentle range of motion exercises for the knee and hip on the operative side, and all joints of the contralateral limb. Isometric quad and gluteal exercises. Upper extremity strengthening for crutch ambulation.
Early Rehabilitation (Weeks 6-12)
- Imaging: Repeat radiographs at 6 weeks post-op to assess early signs of fusion and hardware position.
- Weight-Bearing: If radiographs show initial signs of healing and fixation is secure, protected weight-bearing (PWB) in a CAM boot (25% body weight) can be initiated, gradually progressing over the next 4-6 weeks to 50% weight-bearing.
- Immobilization: Continue CAM boot.
- Rehabilitation: Focus on gait training with assistive devices. Strengthening exercises for the entire lower kinetic chain. No active or passive ankle ROM exercises (as the joint is fused). Proprioceptive training can be initiated once full weight-bearing is tolerated.
Advanced Rehabilitation (Weeks 12-24 and Beyond)
- Imaging: Repeat radiographs at 12 and 24 weeks. Fusion is typically evident by 3-6 months.
- Weight-Bearing: Progress to full weight-bearing (FWB) out of the boot once solid radiographic fusion is confirmed.
- Rehabilitation: Continue with progressive strengthening, balance, and proprioceptive exercises. Emphasis on endurance and functional activities. Return to light activities.
- Return to Activity: Gradual return to work and recreational activities. Full recovery can take 6-12 months. Impact activities should be avoided long-term to protect adjacent joints.
- Long-Term Follow-up: Regular clinical and radiographic follow-up to monitor for complications such as nonunion, infection, implant failure, or adjacent joint arthritis.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls for Ankle Arthrodesis in Complex Cases:
- Pre-operative Planning is Paramount: Utilize 3D CT reconstructions for precise deformity assessment and templating. Understand the magnitude of coronal, sagittal, and rotational malalignment.
- Restore Alignment: The primary goal is a plantigrade, pain-free foot. Aim for neutral dorsiflexion, 5-7 degrees of hindfoot valgus, and neutral rotation. Over-correction or under-correction of deformity will lead to compensatory issues in adjacent joints (subtalar, midfoot, knee, hip).
- Aggressive Debridement: Ensure complete removal of articular cartilage, subchondral sclerosis, and osteophytes to expose viable, bleeding cancellous bone surfaces. This is critical for achieving a successful fusion.
- Bone Grafting: Autogenous bone graft (e.g., iliac crest or distal tibia/calcaneus local graft) is essential for filling defects, stimulating osteogenesis, and promoting robust union, especially in cases of significant bone loss or revision surgery. Allograft can be used as an extender.
- Rigid Fixation: Achieve maximal compression and rigidity across the fusion site. Retrograde intramedullary nails are excellent for multi-segmental fusions (TTC) and complex deformities, offering biomechanical advantages over plate and screw constructs in many settings.
- Soft Tissue Management: Meticulous handling of soft tissues, thoughtful incision placement (avoiding previous scars if possible), and careful skin closure are crucial to prevent wound complications, especially in patients with comorbidities or previous surgeries.
- Fibular Reconstruction (if applicable): Address fibular malunion or nonunion. Restoration of fibular length and rotational alignment contributes to mortise stability and overall foot function, even in a fused ankle.
Pitfalls to Avoid:
- Inadequate Deformity Correction: Failure to achieve a neutral, plantigrade foot can lead to persistent pain, abnormal gait, compensatory stresses on adjacent joints (e.g., subtalar, midfoot, knee), and ultimately patient dissatisfaction.
- Nonunion: The most common complication, with rates varying depending on patient factors (e.g., smoking, diabetes, poor bone quality) and surgical technique. Inadequate debridement, poor apposition, insufficient compression, or unstable fixation are primary causes.
- Infection: A devastating complication that can compromise the fusion and necessitate further surgery, potentially leading to limb loss. Strict sterile technique and appropriate prophylactic antibiotics are essential.
- Malposition/Malunion of Fusion: Fusing the ankle in varus, equinus, or external rotation can severely impair function and lead to calluses, skin breakdown, and painful ambulation.
- Adjacent Joint Arthritis: Fusion of the ankle places increased stress on the subtalar and midfoot joints. While often unavoidable, it is a long-term complication that patients must be counselled about. This is particularly relevant in patients with existing subtalar pathology.
- Neurovascular Injury: Careful identification and protection of superficial peroneal, sural, saphenous nerves, and their associated vessels during approach and dissection.
- Implant-Related Issues: Prominent hardware causing pain, requiring removal. While retrograde IM nails are mostly buried, screws can occasionally be problematic.
- Patient Expectations: Clearly communicate realistic outcomes regarding pain relief, activity levels, and potential long-term issues. Ankle arthrodesis is a salvage procedure, not a restoration of normal ankle motion.
Clinical & Radiographic Imaging

