Mastering Dorsomedial Approaches to the Metatarsophalangeal Joint of the Great Toe
Key Takeaway
Your ultimate guide to Mastering Dorsomedial Approaches to the Metatarsophalangeal Joint of the Great Toe starts here. The dorsomedial approach is a surgical technique to access the metatarsophalangeal joint of the great toe. It is commonly utilized for procedures treating bunions and hallux rigidus, offering direct access to exostoses. This method provides advantages such as avoiding terminal saphenous nerve branches, though considerations like skin healing around the joint of the great toe are noted.
Introduction & Epidemiology
The dorsomedial approach to the first metatarsophalangeal (MTP) joint is a versatile and frequently employed surgical pathway in orthopedic foot and ankle surgery. It provides direct access to the medial aspect of the joint, facilitating a broad spectrum of procedures for common pathologies such as hallux valgus and hallux rigidus. Its utility stems from its ability to expose the medial eminence of the first metatarsal head, the medial capsule, and the proximal phalanx, with minimal disruption to the critical dorsal neurovascular structures.
Hallux valgus, a complex triplanar deformity, affects a significant portion of the adult population, with reported prevalence rates ranging from 23% in adults aged 18-65 years to 35.7% in those over 65 years. Similarly, hallux rigidus, a degenerative arthritic condition of the first MTP joint, is the most common arthritic condition of the foot, affecting approximately 1 in 45 individuals over the age of 50. The increasing prevalence of these conditions, coupled with patient expectations for pain relief and functional restoration, underscores the importance of a mastery of surgical approaches like the dorsomedial incision. While the directness of this approach is a major advantage, surgeons must be cognizant of potential drawbacks, including the thinner and potentially more tenuous medial skin, which may impact wound healing and scar aesthetics. Understanding the intricate anatomy and biomechanics is paramount to optimizing outcomes with this approach.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy of the first MTP joint is critical for safe and effective utilization of the dorsomedial approach.
Bony Anatomy
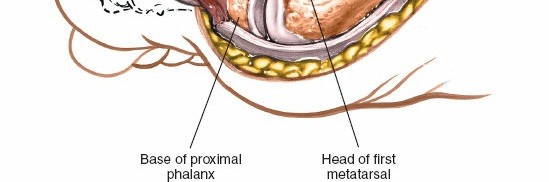
The first MTP joint is formed by the articulation of the head of the first metatarsal and the base of the proximal phalanx of the hallux.
*
First Metatarsal:
The metatarsal head is convex, with a characteristic medial flare that often forms the "bunion" in hallux valgus. Dorsally, the head can develop osteophytes in hallux rigidus. Plantarly, two distinct grooves accommodate the sesamoid bones, which are embedded within the conjoined tendon of the flexor hallucis brevis.
*
Proximal Phalanx:
The base of the proximal phalanx is concave, articulating with the metatarsal head. Its medial and lateral condyles provide attachment points for collateral ligaments and muscle tendons.
*
Sesamoids:
These two small bones are positioned within the plantar plate complex beneath the metatarsal head. They act as a fulcrum for the flexor hallucis brevis, increasing its mechanical advantage, and contribute significantly to MTP joint stability. Their position is often displaced laterally in hallux valgus.
Ligamentous and Capsular Structures
The MTP joint capsule is reinforced by several ligaments:
*
Collateral Ligaments:
Strong medial and lateral collateral ligaments connect the metatarsal head to the proximal phalanx, providing primary stability.
*
Plantar Plate:
A thick fibrocartilaginous structure on the plantar aspect of the joint, continuous with the joint capsule and firmly attached to the proximal phalanx base and the sesamoids. It resists dorsiflexion and provides stability.
*
Medial Capsular Structures:
The medial capsule is often attenuated and redundant in hallux valgus, allowing for medial deviation of the phalanx. Conversely, it can be hypertrophied and contracted in hallux rigidus.
Musculotendinous Structures
Several tendons traverse or insert around the first MTP joint:
*
Extensor Hallucis Longus (EHL):
Located dorsally, superficial to the joint capsule, responsible for dorsiflexion of the hallux. It courses across the dorsum of the MTP joint.
*
Flexor Hallucis Longus (FHL):
Located plantarly, deep to the sesamoids, responsible for plantarflexion of the hallux.
*
Abductor Hallucis:
Originates from the medial tubercle of the calcaneus, inserts into the medial aspect of the base of the proximal phalanx and the medial sesamoid. Its tendon courses medially to the joint, often displaced dorsally in severe hallux valgus.
*
Adductor Hallucis:
Composed of oblique and transverse heads, inserting into the lateral aspect of the base of the proximal phalanx and the lateral sesamoid. It is a primary deforming force in hallux valgus.
*
Flexor Hallucis Brevis:
A bipartite muscle with medial and lateral heads, inserting into the medial and lateral sesamoids, respectively, and contributing to plantarflexion and MTP joint stability.
Neurovascular Structures
The dorsomedial approach requires careful attention to critical neurovascular structures:
*
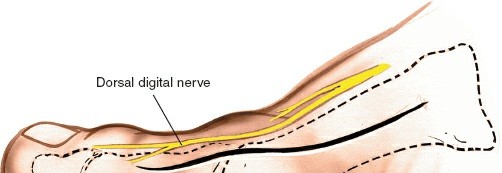
Medial Dorsal Cutaneous Nerve:
A branch of the superficial fibular (peroneal) nerve, it typically runs dorsally over the first metatarsal shaft. Its terminal branches often cross the surgical field dorsomedially.
*
Saphenous Nerve:
A terminal sensory branch from the femoral nerve, it courses along the medial aspect of the foot, deep to the abductor hallucis muscle and dorsal to the flexor hallucis longus tendon. Its terminal branches can provide innervation to the medial skin of the great toe.
*
Dorsal Digital Artery and Vein (First Dorsal Metatarsal Artery):
These vessels run dorsally, with branches supplying the first web space and the medial aspect of the great toe.
The major advantage of the dorsomedial skin incision is that it gives direct access to the exostosis and is anatomically farther away from the terminal branches of the saphenous nerve and the main trunks of the medial dorsal cutaneous nerve compared to a purely dorsal incision, although smaller branches may still be encountered.
Biomechanics
The first MTP joint functions as a critical component of the foot's propulsion mechanism during gait.
*
Weight Bearing:
During the stance phase, the MTP joint absorbs significant load.
*
Windlass Mechanism:
During toe-off, dorsiflexion of the MTP joint tightens the plantar fascia, raising the medial longitudinal arch and rigidifying the foot for propulsion. This mechanism is often impaired in hallux rigidus and can be affected by hallux valgus.
*
Deformity in Hallux Valgus:
In hallux valgus, the first metatarsal typically adducts and pronates, while the hallux abducts and pronates. The medial eminence becomes prominent, the sesamoids sublux laterally, and the adductor hallucis and EHL contribute to the deformity.
*
Pathology in Hallux Rigidus:
Characterized by progressive degeneration of the articular cartilage, often initiating with dorsal impingement due to osteophyte formation, leading to pain, stiffness, and restricted dorsiflexion.
Indications & Contraindications
The dorsomedial approach provides excellent access for a variety of surgical procedures addressing pathologies of the first MTP joint.
Indications
Its use includes the following:
1.
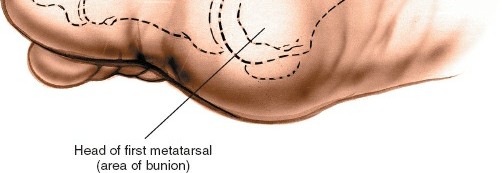
Excision of exostosis of the first metatarsal (bunionectomy):
Primarily for the symptomatic medial eminence in hallux valgus.
2.
Chevron or Scarf osteotomies:
For correction of mild to moderate hallux valgus, involving an osteotomy of the first metatarsal.
3.
Akin osteotomy:
A medial closing wedge osteotomy of the proximal phalanx, often performed adjunctively with metatarsal osteotomies for correction of hallux valgus interphalangeus.
4.
Excision of the proximal part of the proximal phalanx of the hallux (Keller procedure):
A resectional arthroplasty for severe hallux rigidus or severe hallux valgus in the elderly, low-demand patient.
5.
Procedures on the medial joint capsule, including reefing and V-Y plasties:
For capsular plication in hallux valgus or capsular release in hallux rigidus.
6.
Arthrodesis of the metatarsophalangeal joint:
A definitive salvage procedure for severe hallux rigidus, post-traumatic arthritis, or failed MTP joint surgery.
7.
Insertion of total joint replacements or interpositional arthroplasty:
For MTP joint arthritis, offering pain relief and motion preservation in select cases.
8.
Dorsal wedge osteotomy of the proximal phalanx in cases of hallux rigidus (Moberg osteotomy):
To improve dorsiflexion by changing the orientation of the articular surface of the proximal phalanx.
9.
Cheilectomy:
Debridement of dorsal osteophytes from the metatarsal head and proximal phalanx for early to moderate hallux rigidus.
10.
Resection of benign medial soft tissue masses or osteochondromas.
Contraindications
Absolute contraindications for any elective foot surgery apply, including:
* Active infection in the surgical field or systemic sepsis.
* Severe peripheral vascular disease with compromised circulation to the foot.
* Uncontrolled diabetes mellitus.
* Coagulopathy refractory to correction.
* Acute Charcot neuroarthropathy.
* Severe skin compromise over the surgical site (e.g., ulceration, severe scarring from previous surgery, impending skin necrosis).
Relative contraindications include:
* Patient non-compliance with post-operative protocols.
* Unrealistic patient expectations.
* Significant immunosuppression.
* Severe obesity.
* Nicotine use (increases risk of wound healing complications and nonunion).
* Certain neuromuscular disorders affecting gait and balance.
* Severe flatfoot deformity requiring complex hindfoot reconstruction.
Operative vs. Non-Operative Indications
| Indication Type | Operative Management | Non-Operative Management |
|---|---|---|
| Hallux Valgus | - Painful medial eminence | - Wide toe box shoes |
| - Progressive deformity with MTP subluxation | - Orthotics (arch support, toe spacers) | |
| - Failure of conservative measures | - NSAIDs, icing | |
| - Associated MTP joint arthritis or instability | - Activity modification | |
| Hallux Rigidus | - Persistent pain despite conservative treatment | - Stiff-soled shoes, rocker-bottom shoes |
| - Impingement symptoms (cheilectomy) | - Orthotics (carbon fiber plate) | |
| - Significant loss of MTP joint motion impacting function | - NSAIDs, corticosteroid injections | |
| - Advanced arthritis (arthrodesis, arthroplasty) | - Activity modification | |
| MTP Joint Arthritis | - Chronic pain and functional limitation | - Activity modification |
| - Failure of conservative management | - NSAIDs, corticosteroid injections | |
| - Bone-on-bone changes (arthrodesis, arthroplasty) | - Shoe modifications | |
| Other Deformities | - Painful congenital deformities | - Custom orthotics, bracing |
| - Significant functional impairment from deformity | - Physical therapy for muscle balance | |
| - Large, symptomatic benign masses | - Observation for asymptomatic lesions |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential for successful outcomes.
Pre-Operative Planning
-
Clinical Assessment:
- History: Detailed history of pain, duration, aggravating/alleviating factors, functional limitations, previous treatments, and relevant comorbidities (diabetes, neuropathy, vascular disease).
-
Physical Examination:
- Gait analysis, assessment of foot posture (pes planus, cavus).
- Visual inspection for skin integrity, callus formation, hammer toes, lesser toe deformities.
- Palpation for tenderness, especially over the medial eminence, MTP joint line, and sesamoids.
- Range of motion (ROM) of the first MTP joint (dorsiflexion, plantarflexion, abduction, adduction) – both passive and active, weight-bearing and non-weight-bearing. Assess for crepitus.
- Assessment of reducible vs. fixed deformity (e.g., in hallux valgus, does the deformity correct passively?).
- Neurovascular status: Dorsalis pedis and posterior tibial pulses, capillary refill, sensation (light touch, sharp/dull, two-point discrimination).
- Tinel's sign over neural pathways, if nerve entrapment is suspected.
-
Radiographic Evaluation:
-
Weight-bearing Anteroposterior (AP), Lateral, and Oblique Views:
These are mandatory.
- AP View: Assess hallux valgus angle (HVA), intermetatarsal angle (IMA), distal articular set angle (DASA), proximal articular set angle (PASA), congruity of the MTP joint, sesamoid position (Hardy and Clapham scale), and presence of medial eminence/osteophytes.
- Lateral View: Assess MTP joint space, dorsal osteophytes (for hallux rigidus), metatarsal elevation/depression, and alignment of the proximal phalanx.
- Oblique View: Can further assess metatarsal head morphology, sesamoid integrity, and osteophytes.
- Additional Imaging: CT or MRI may be useful for complex deformities, suspected avascular necrosis, osteochondral lesions, or tumor evaluation, but are not routinely required for standard hallux valgus or rigidus.
-
Weight-bearing Anteroposterior (AP), Lateral, and Oblique Views:
These are mandatory.
-
Surgical Plan Formulation:
- Based on clinical and radiographic findings, determine the primary pathology and secondary deformities.
- Select the appropriate procedure (e.g., cheilectomy vs. arthrodesis for hallux rigidus; chevron vs. scarf for hallux valgus).
- Plan osteotomy cuts, fixation methods (screws, plates, wires), and necessary soft tissue releases (e.g., lateral capsular release, adductor tenotomy).
- Consider implant size and type if arthroplasty or arthrodesis is planned.
Patient Positioning
Place the patient supine on the operating table.
* The operative leg should be externally rotated and the foot positioned comfortably on the table or an optional foot holder to allow for unimpeded access to the medial aspect.
* A padded thigh tourniquet is typically applied to the middle of the thigh after exsanguination with an Esmarch bandage. Alternatively, an ankle tourniquet can be used for shorter procedures or in patients where a thigh tourniquet is contraindicated, although this limits the operative field for proximal procedures if needed. Tourniquet time should be carefully monitored.
*
Sterile Prep and Drape:
The foot and ankle are meticulously prepped with an antiseptic solution (e.g., chlorhexidine or povidone-iodine) and draped in a sterile fashion, ensuring adequate exposure of the entire forefoot and distal ankle. The use of a sterile stockinette or impervious drape around the tourniquet can help maintain sterility.
*
C-arm Placement:
If intraoperative fluoroscopy is anticipated (common for osteotomies, arthrodesis, or complex reconstructions), the C-arm should be positioned for easy access to obtain AP and lateral views of the first MTP joint without compromising the sterile field.
Detailed Surgical Approach / Technique
The dorsomedial approach allows for a systematic dissection to the first MTP joint. The description below outlines a generalized technique, with specific procedural variations noted.
Incision
-
Skin Incision:
A longitudinal incision is typically made along the dorsomedial aspect of the first MTP joint. It begins approximately 1-2 cm proximal to the joint line, along the shaft of the first metatarsal, extending distally across the joint and terminating just proximal to the interphalangeal joint of the hallux. The length is generally 4-6 cm, tailored to the specific procedure and required exposure. The incision is usually made just medial to the EHL tendon to minimize injury to the medial dorsal cutaneous nerve and its branches, which commonly run dorsally.
Superficial Dissection
- Subcutaneous Tissue: The incision is deepened through the skin and subcutaneous fat. Meticulous hemostasis is maintained.
-
Identification of Neurovascular Structures:
The most critical step at this stage is to identify and protect the terminal branches of the medial dorsal cutaneous nerve and potentially the saphenous nerve. These delicate sensory nerves typically lie within the subcutaneous tissue or superficial fascia. They should be carefully identified, mobilized, and retracted dorsally and/or medially. Injury to these nerves can lead to painful neuromas or persistent sensory deficits.

- Note: The seed content correctly highlights that this approach is anatomically farther away from the main saphenous nerve branches, reducing the risk compared to a more medial or plantar incision.
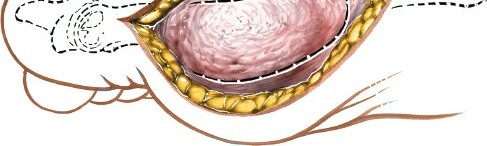
Deep Dissection and Capsular Exposure
- Superficial Fascia: The superficial fascia is incised, exposing the underlying joint capsule and the medial eminence of the first metatarsal. The abductor hallucis tendon may be visualized medially, often retracted dorsally in hallux valgus.
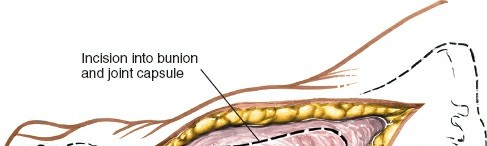
-
Joint Capsule:
The medial aspect of the joint capsule is now fully exposed. The type of capsular incision depends on the pathology and planned procedure:
- Longitudinal Incision: A straight longitudinal incision through the capsule from the metatarsal shaft to the proximal phalanx, parallel to the EHL tendon. This provides direct access for exostectomy and joint inspection.
- Inverted L-shaped Capsulotomy: A longitudinal incision is made over the medial aspect of the metatarsal head, and then extended transversely plantarwards at the level of the metatarsal neck or distal to the medial eminence. This allows for excellent exposure of the medial eminence and plantar plate.
- H-shaped Capsulotomy: Two longitudinal incisions connected by a transverse incision. This creates two capsular flaps, useful for procedures requiring later capsular reefing or plication.
- V-Y Capsuloplasty: A V-shaped incision with the apex proximal, allowing for lengthening of the capsule upon closure, useful in cases of a tight capsule or for providing additional exposure.
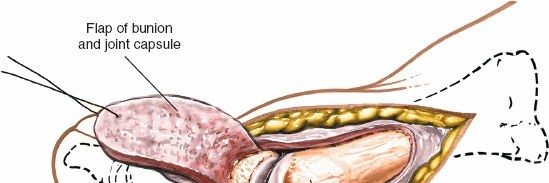
-
Reflection of Capsular Flaps:
Once the capsulotomy is performed, the capsular flaps are carefully elevated from the underlying bone using a periosteal elevator, exposing the medial eminence of the first metatarsal head and the MTP joint line.

Operative Procedures (via Dorsomedial Approach)
1. Exostectomy (Bunionectomy)
-
With the medial eminence fully exposed, an oscillating saw or osteotome is used to resect the prominent medial exostosis. The cut is made parallel to the medial shaft of the first metatarsal, ensuring that the sagittal groove for the medial sesamoid is not violated and that adequate bone is left for soft tissue reattachment.
- The bone edges are then carefully rasped smooth to prevent soft tissue irritation.
2. Cheilectomy for Hallux Rigidus
- After capsular exposure, the MTP joint is dorsiflexed to identify dorsal osteophytes on both the metatarsal head and the proximal phalanx base.
- An oscillating saw or osteotome is used to remove these osteophytes, typically excising 25-30% of the dorsal articular surface of the metatarsal head. This increases the dorsal space, improving dorsiflexion.
- Any hypertrophic synovium or loose bodies are debrided. The range of motion is then assessed.
3. Chevron Osteotomy (for Hallux Valgus)
- Following medial eminence resection, a V-shaped osteotomy is performed in the metatarsal head. The apex of the "V" is usually distal, just proximal to the articular cartilage, and the limbs extend proximally at 60-70 degree angles.
- The distal fragment is then translated laterally to correct the hallux valgus deformity and improve the intermetatarsal angle.
- Fixation is typically achieved with a single K-wire or 1-2 small screws (e.g., 2.7 mm or 3.0 mm cortical screws), ensuring adequate compression and stability.
4. Scarf Osteotomy (for Hallux Valgus)
- This Z-shaped osteotomy allows for significant correction in the sagittal and transverse planes.
- Two longitudinal cuts are made on the dorsal and plantar aspects of the metatarsal shaft, connected by an oblique cut through the center.
- The metatarsal head fragment is then translated laterally and potentially rotated to correct deformity.
- Fixation usually involves two cortical screws (e.g., 2.7 mm or 3.0 mm), one dorsal and one plantar.
5. Akin Osteotomy
- A medial closing wedge osteotomy of the proximal phalanx, usually performed distal to the MTP joint.
- A small wedge of bone is removed from the medial aspect of the proximal phalanx, with the base of the wedge directed medially and the apex laterally.
- The osteotomy is closed and fixed with a K-wire, small screw, or cerclage wire.
6. Keller Resectional Arthroplasty
- After medial capsular exposure, a portion (typically 25-50%) of the base of the proximal phalanx is resected with an oscillating saw.
- The amount resected depends on the severity of the arthritis and the desired amount of decompression.
- Often, the remaining capsule is interposed into the joint space (capsular interposition) or a portion of the FHB tendon.
7. MTP Joint Arthrodesis
- The articular cartilage surfaces of both the first metatarsal head and the proximal phalanx base are resected, exposing cancellous bone.
-
The bone ends are contoured for optimal contact and stability, often with opposing convex/concave surfaces (cup-and-cone) or flat cuts, to achieve a functional position (typically 10-15 degrees dorsiflexion and 5-10 degrees valgus).

-
Fixation is achieved with a combination of screws (e.g., 3.5 mm or 4.0 mm cancellous screws) and/or a dorsal locking plate. The aim is rigid internal fixation to promote fusion.
8. Total Joint Arthroplasty
- Resection of the diseased articular surfaces of the metatarsal head and proximal phalanx base, similar to arthrodesis preparation.
- Precision bone cuts are made to accommodate the selected prosthetic components (e.g., silicone, titanium, pyrocarbon).
- Implants are typically press-fit or cemented into place.
Capsular and Soft Tissue Management
- Capsular Plication/Reefing: In hallux valgus procedures, after osteotomy and correction, the medial capsular flaps are often tightened (plicated or reefed) to maintain the correction and stabilize the joint. This can be done with non-absorbable sutures.
- Capsular Release: In hallux rigidus, capsular release may be necessary to improve joint motion.
- Lateral Release: While not directly part of the dorsomedial approach, a lateral capsular release and adductor hallucis tenotomy are often performed through a separate plantar-lateral stab incision or via plantar dissection to address the lateral soft tissue contracture in hallux valgus correction.
Closure
- Capsular Closure: The capsular flaps are meticulously repaired or plicated using absorbable sutures (e.g., 2-0 or 3-0 absorbable suture). This helps to stabilize the correction and prevent recurrence.
- Subcutaneous Tissue: The subcutaneous layer is closed with interrupted absorbable sutures to reduce dead space and provide a secure foundation for skin closure.
- Skin Closure: The skin is closed with fine non-absorbable sutures or staples. Careful attention to skin edge eversion and tension-free closure is crucial for optimal wound healing and cosmesis.
- Dressing: A sterile, bulky dressing is applied, often incorporating soft padding and compression. A modified "bunion dressing" or a splint may be applied to maintain the corrected position, especially after osteotomies or soft tissue balancing.
Complications & Management
Despite meticulous surgical technique, complications can arise following procedures utilizing the dorsomedial approach. Proactive management and patient education are key.
| Complication | Incidence (Approximate) | Salvage Strategies |
|---|---|---|
| Wound Healing Issues | 5-15% | - Local wound care, debridement |
| (dehiscence, infection, superficial) | - Antibiotics for infection | |
| - Surgical debridement for deep infections | ||
| - Skin grafting/flaps for severe dehiscence | ||
| Nerve Injury | 1-10% | - Observation (most neurapraxias resolve) |
| (medial dorsal cutaneous, saphenous) | - Neurolysis or neurectomy for persistent painful neuroma | |
| Recurrence of Deformity | 10-25% (Hallux Valgus) | - Revision osteotomy |
| - Arthrodesis | ||
| - Arthroplasty | ||
| MTP Joint Stiffness/Arthrosis | 5-20% | - Physical therapy, mobilization exercises |
| - Cheilectomy or lysis of adhesions | ||
| - Arthrodesis or arthroplasty (for severe arthrosis) | ||
| Avascular Necrosis (AVN) | 1-5% (osteotomies) | - Conservative management for mild cases |
| - Debridement and bone grafting | ||
| - Arthrodesis or arthroplasty for severe AVN | ||
| Hardware Complications | 5-15% | - Symptomatic hardware removal (after bone healing) |
| (prominence, loosening) | - Revision fixation for loosening/nonunion | |
| Nonunion/Malunion | 2-10% (osteotomies/arthrodesis) | - Non-operative for asymptomatic malunion (orthotics) |
| - Revision osteotomy for symptomatic malunion | ||
| - Revision arthrodesis with bone grafting/plates for nonunion | ||
| Complex Regional Pain Syndrome (CRPS) | <1% (rare but devastating) | - Multimodal pain management (medications, nerve blocks) |
| - Physical therapy, psychological support | ||
| Metatarsalgia/Transfer Lesion | 5-15% | - Shoe modifications, orthotics |
| - Lesser metatarsal osteotomies for severe cases |
Specific Management Considerations:
- Wound Healing: The seed content accurately notes that the medial skin is thinner and may not heal as well. This requires careful tissue handling, tension-free closure, and vigilant post-operative wound care. Smoking cessation is paramount pre-operatively.
- Nerve Injury: Prevention is key, with meticulous identification and protection of superficial nerve branches. If a painful neuroma develops, conservative measures (injections, desensitization) are attempted first, followed by surgical excision or neurolysis if refractory.
- Recurrence of Deformity: Proper patient selection, adequate bony correction, and balanced soft tissue tension are crucial. Recurrence may necessitate revision surgery, potentially involving more aggressive osteotomies or arthrodesis.
- MTP Joint Stiffness: Early protected range of motion, once soft tissue healing allows, is important. Physical therapy, mobilization, and NSAIDs can help. In severe, recalcitrant cases, lysis of adhesions or a cheilectomy may be considered.
- Avascular Necrosis (AVN) of the Metatarsal Head: This is a rare but serious complication, especially after distal metatarsal osteotomies (e.g., chevron). Meticulous technique to preserve vascularity (e.g., preserving plantar periosteum, minimizing periosteal stripping) is vital. Management depends on severity, ranging from protected weight-bearing to arthrodesis or arthroplasty.
Post-Operative Rehabilitation Protocols
Rehabilitation protocols vary significantly based on the specific procedure performed, the stability of fixation, and surgeon preference. However, general principles apply.
Phase 1: Immediate Post-Operative (Weeks 0-2)
- Goal: Pain control, protect surgical site, minimize swelling, maintain stable fixation.
-
Weight-Bearing:
- Bunionectomy/Osteotomy (e.g., Chevron, Scarf): Protected weight-bearing in a post-operative shoe (hard-soled, flat-bottomed) or walking boot, often with heel-only weight-bearing for 2-4 weeks.
- Arthrodesis: Typically non-weight-bearing (NWB) in a boot or cast for 4-6 weeks, sometimes longer depending on fixation and surgeon preference.
- Cheilectomy/Keller: Weight-bearing as tolerated (WBAT) in a post-operative shoe.
- Dressings: Maintain sterile surgical dressing. Non-absorbable sutures are typically removed at 10-14 days.
- Elevation & Ice: Strict elevation above the heart for the first 3-5 days, then intermittently. Regular icing to reduce swelling and pain.
- Pain Management: Opioids initially, transitioning to NSAIDs and acetaminophen as pain subsides.
- Range of Motion: Gentle, passive, or active range of motion (ROM) of the interphalangeal joint (if not involved in surgery) and ankle. MTP joint ROM is generally restricted or initiated cautiously based on the procedure (e.g., after cheilectomy, early active dorsiflexion is encouraged; after osteotomy, MTP ROM is typically protected).
Phase 2: Early Mobilization (Weeks 2-6)
- Goal: Gradual increase in weight-bearing, restore protected MTP joint ROM, reduce swelling, improve soft tissue healing.
- Weight-Bearing: Progress from protected to full weight-bearing in a post-operative shoe or walking boot as tolerated and as per surgeon's protocol and radiographic evidence of healing.
-
Physical Therapy (PT):
- ROM: Initiate gentle, progressive active and passive MTP joint ROM exercises. Focus on dorsiflexion and plantarflexion.
- Scar Management: Gentle scar massage once wound is fully healed.
- Edema Control: Continued elevation, compression stockings.
- Shoe Wear: Transition from surgical shoe/boot to a wider, supportive athletic shoe or comfort shoe by the end of this phase, provided swelling has significantly decreased and bone healing is progressing.
Phase 3: Intermediate Rehabilitation (Weeks 6-12)
- Goal: Restore full MTP joint ROM (if motion-sparing procedure), improve strength, normalize gait.
- Weight-Bearing: Full weight-bearing in supportive athletic shoes.
-
Physical Therapy:
- Strengthening: Initiate intrinsic and extrinsic foot muscle strengthening exercises (e.g., towel scrunches, marble pick-ups, theraband exercises).
- Proprioception: Balance and proprioceptive exercises (e.g., single-leg stance).
- Gait Training: Focus on normalizing gait pattern and progression to push-off phase.
- Flexibility: Continue MTP joint and ankle ROM exercises.
- Activity: Gradually return to activities of daily living. Low-impact activities (swimming, cycling) may be initiated.
Phase 4: Advanced Rehabilitation and Return to Activity (Months 3-6+)
- Goal: Maximize functional outcomes, return to sport/high-impact activities (where appropriate).
-
Physical Therapy:
- Sport-Specific Training: For athletes, progressive return to running, jumping, and agility drills.
- Strength and Conditioning: Continue strengthening and conditioning of the foot, ankle, and lower extremity.
- Shoe Wear: Patients should generally be advised to wear supportive, comfortable shoes with a wide toe box long-term. High heels should be avoided or limited.
-
Long-Term:
- Continued vigilance for recurrent deformity or symptoms.
- Orthotic use may be recommended for ongoing support or pain relief.
- Follow-up radiographs at 6 months and 1 year to assess healing and joint status.
Note: For arthrodesis, the primary goal is rigid fusion, and early weight-bearing and aggressive ROM are contraindicated. Rehabilitation focuses on protecting the fusion site until radiographic consolidation is achieved, typically 8-12 weeks, followed by a gradual return to activity.
Summary of Key Literature / Guidelines
The dorsomedial approach remains a cornerstone for first MTP joint surgery, and its applications are supported by decades of research and clinical experience.
Hallux Valgus Correction:
*
Chevron Osteotomy:
Considered the gold standard for mild-to-moderate hallux valgus with good long-term outcomes, as evidenced by studies from Austin and McInnes (1976), and more recently, comparative studies showing its effectiveness against other osteotomies. A systematic review by Trnka et al. (2007) highlighted excellent pain relief and correction with low complication rates for distal metatarsal osteotomies.
*
Scarf Osteotomy:
Popularized by Barouk (1995), it offers greater correction potential than the chevron, particularly for moderate-to-severe deformities, due to its inherent stability and ability for multiplanar correction. Comparative studies (e.g., Coetzee et al., 2008) suggest similar or slightly superior correction rates compared to chevron, with good patient satisfaction but a potentially steeper learning curve.
*
Akin Osteotomy:
Often an adjunct to metatarsal osteotomies, the medial closing wedge osteotomy of the proximal phalanx, initially described by Akin (1925), is critical for correcting hallux valgus interphalangeus and maintaining toe alignment.
Hallux Rigidus Management:
*
Cheilectomy:
For early-to-moderate hallux rigidus (Grade I-II Coughlin and Shurnas), cheilectomy is highly effective in relieving dorsal impingement and improving motion. Studies (e.g., Hattrup and Johnson, 1988; Easley et al., 1999) demonstrate good-to-excellent results in 70-90% of patients, with long-term durability.
*
Moberg Osteotomy:
A dorsal closing wedge osteotomy of the proximal phalanx enhances dorsiflexion and is often combined with cheilectomy for Grade II-III hallux rigidus.
*
Keller Resectional Arthroplasty:
A historical procedure for severe hallux rigidus or valgus in low-demand patients, providing pain relief by joint decompression. However, it is associated with shortening, weakness, and transfer metatarsalgia. Its use has declined in favor of arthrodesis or arthroplasty for active patients.
*
MTP Joint Arthrodesis:
Considered the gold standard for end-stage hallux rigidus, severe MTP joint arthritis, or failed previous MTP joint surgeries. High fusion rates (90-95%) and excellent pain relief are reported. Key literature (e.g., Brodsky et al., 2007) emphasizes proper positioning (10-15 degrees dorsiflexion, 5-10 degrees valgus) for optimal functional outcomes.
Arthroplasty:
*
Interpositional Arthroplasty:
Utilizes soft tissue or synthetic spacers after resection, aiming for pain relief and motion preservation.
*
Total Joint Arthroplasty:
While initial designs had high failure rates, newer implant designs show promise, especially for select low-demand patients where motion preservation is prioritized over fusion. Long-term data is still evolving, but studies by Glazebrook et al. (2012) and Townley et al. (2007) provide insights into outcomes and challenges.
General Considerations:
*
Wound Healing:
Studies consistently identify smoking, diabetes, and peripheral vascular disease as significant risk factors for wound complications, particularly relevant given the thinner skin on the medial aspect.
*
Nerve Injury:
Incidence of nerve irritation or neuroma is a concern, reinforcing the need for meticulous soft tissue dissection and nerve protection.
*
Evidence-Based Guidelines:
Many professional societies (e.g., AAOS, AOFAS) provide clinical practice guidelines emphasizing the importance of shared decision-making, considering patient activity levels, and utilizing objective radiographic and clinical measures for surgical planning. The dorsomedial approach, when applied judiciously and with a nuanced understanding of its advantages and limitations, remains a highly effective surgical tool in the academic orthopedic surgeon's armamentarium.
Clinical & Radiographic Imaging