Essential Dorsal Approach for Second, Third, Fourth MTP Joints
Key Takeaway
This topic focuses on Essential Dorsal Approach for Second, Third, Fourth MTP Joints, The dorsal approach exposes metatarsophalangeal joints of the second, third, fourth, and fifth toes. This surgical technique avoids incising plantar weight-bearing skin, reducing scarring. It is utilized for procedures such as excising metatarsal heads, performing distal metatarsal osteotomies, partial proximal phalangectomies, and capsulotomies, maintaining foot integrity.
Introduction & Epidemiology
The forefoot, particularly the metatarsophalangeal (MTP) joint complex, is a common site for degenerative, inflammatory, traumatic, and iatrogenic pathologies. Conditions affecting the second, third, and fourth MTP joints, such as hammertoe/claw toe deformities, Freiberg's infraction, MTP joint instability, synovitis, and bunionette deformities with concomitant lesser toe involvement, often necessitate surgical intervention. The dorsal approach to these joints offers a direct and versatile avenue for addressing a wide spectrum of these pathologies while judiciously avoiding the weight-bearing plantar skin.
Historically, surgical approaches to the MTP joints have varied, with plantar incisions favored for certain procedures like direct capsular repair for plantar plate tears. However, the inherent risk of painful scar formation, neuroma development, and potential alterations in foot biomechanics associated with plantar incisions has led to a paradigm shift towards dorsal or dorsomedial/dorsolateral approaches where feasible. The dorsal approach minimizes these plantar complications, providing excellent visualization of the MTP joint, distal metatarsal, and proximal phalanx. This allows for precise osseous resections, osteotomies, arthrodesis, and soft tissue releases, which are critical for restoring proper forefoot alignment and function.
Epidemiologically, lesser MTP joint pathology is prevalent. Hammertoe and claw toe deformities, often involving the second MTP joint due to its length and proximity to the hallux, affect a significant portion of the adult population, with increasing incidence with age. Freiberg's infraction, an osteochondrosis of the metatarsal head, most commonly affects the second metatarsal. MTP joint instability and synovitis, frequently encountered in the second MTP joint, are increasingly recognized as sources of chronic forefoot pain and deformity. Surgical correction via the dorsal approach aims to alleviate pain, correct deformity, and prevent progression of adjacent joint pathology, thereby improving patient mobility and quality of life.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy of the lesser MTP joints is paramount for safe and effective dorsal intervention.
Osseous Structures
The lesser MTP joints are condyloid joints formed by the articulation of the distal metatarsal head and the proximal phalanx base. The metatarsal heads possess a dorsal prominence and a relatively flatter plantar surface. The proximal phalanx base has a biconcave articular surface that articulates with the metatarsal head. The sesamoid bones, while prominent under the first MTP, are often rudimentary or absent under the lesser MTPs.
Ligamentous and Capsular Structures
The MTP joint capsule is a complex structure providing significant stability. It is reinforced dorsally by the extensor hood mechanism and collateral ligaments, and plantarly by the plantar plate and deep transverse metatarsal ligament (DTML).
*
Collateral Ligaments:
The medial and lateral collateral ligaments originate from the sides of the metatarsal head and insert onto the respective sides of the proximal phalanx base. They are taut in flexion and relaxed in extension.
*
Plantar Plate:
A thick fibrocartilaginous structure originating from the metatarsal neck and inserting onto the base of the proximal phalanx. It is a critical stabilizer against dorsal subluxation and hyperextension, and provides articulation for the flexor tendons.
*
Deep Transverse Metatarsal Ligament (DTML):
Connects the plantar plates and capsules of adjacent MTP joints, providing transverse stability to the forefoot and preventing splaying of the metatarsal heads. This ligament must often be incised or carefully retracted during dorsal approaches, especially when addressing multiple adjacent joints.
*
Extensor Hood Mechanism:
Formed by the extensor digitorum longus (EDL) and brevis (EDB) tendons, interossei, and lumbricals. It covers the dorsal aspect of the MTP joint, contributing to dorsal stability and facilitating toe extension. The sagittal bands, part of the extensor hood, originate from the extensor tendon and insert onto the plantar plate and DTML.
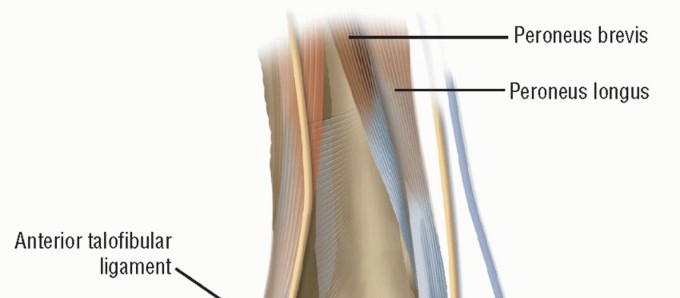
Tendinous Structures
- Extensor Digitorum Longus (EDL): Primary dorsiflexor of the MTPs and interphalangeal (IP) joints. It courses dorsally over the MTP joint.
- Extensor Digitorum Brevis (EDB): Assists EDL in MTP dorsiflexion, typically inserting into the proximal phalanx or extensor hood.
- Flexor Digitorum Longus (FDL) and Brevis (FDB): Course plantarly, providing plantarflexion of the IP joints.
- Lumbricals and Interossei: Small intrinsic muscles contributing to MTP flexion and IP extension.
Neurovascular Structures
The dorsal aspect of the MTP joints harbors critical neurovascular structures.
*
Dorsal Digital Nerves:
Branches of the superficial peroneal nerve (for MTPs 2-4) or deep peroneal nerve (for the first web space) supply sensation to the dorsal aspect of the toes. These nerves course subcutaneously and are highly susceptible to iatrogenic injury during dorsal approaches. Care must be taken to identify and protect them.
*
Dorsal Metatarsal Arteries and Veins:
The dorsal metatarsal arteries, branches of the dorsalis pedis artery, and their accompanying veins supply the dorsal foot and toes. These vessels course deep to the extensor tendons and must be managed with meticulous hemostasis.
Biomechanics
The lesser MTP joints function as critical pivots in the gait cycle, undergoing complex motion including dorsiflexion, plantarflexion, abduction, and adduction. During toe-off, the MTP joints dorsiflex significantly, necessitating robust plantar plate and collateral ligament integrity. Pathologies disrupting this balance, such as plantar plate tears leading to MTP joint instability or rigid hammertoe deformities, alter forefoot load distribution, leading to pain, callosities, and progression of deformity. The dorsal approach, by allowing direct access for bony correction and soft tissue balancing, aims to restore normal joint kinematics and dynamic stability.
Indications & Contraindications
The dorsal approach to the second, third, and fourth MTP joints is versatile, indicated for a range of conditions requiring direct access to the joint, metatarsal head, or proximal phalanx. The primary advantage lies in avoiding incisions on the weight-bearing plantar skin.
Indications
-
Excision of Metatarsal Heads:
- Freiberg's Infraction: Advanced stages (stages III-V) with significant cartilage destruction, pain, and deformity.
- Refractory Metatarsalgia: Chronic pain unresponsive to conservative measures, often associated with prominent or hypertrophic metatarsal heads (e.g., secondary to Morton's neuroma, though the neuroma itself is often excised via a dorsal approach to the web space, the MTP joint pathology might be co-addressed).
- MTP Joint Arthritis: Severe degenerative changes or inflammatory arthritis causing pain and joint destruction.
-
Distal Metatarsal Osteotomy:
- Overlength Metatarsal: Corrective shortening osteotomies (e.g., Weil osteotomy) for MTP joint instability, plantar plate pathology, or refractory metatarsalgia due to an excessively long metatarsal.
- Metatarsal Head Deformity/Malalignment: Correction of angular or rotational deformities.
-
Partial Proximal Phalangectomy / PIP Joint Arthroplasty:
- Hammertoe/Claw Toe Deformity: Rigid deformities, typically for proximal interphalangeal (PIP) joint arthroplasty (resection of proximal phalanx head) or for MTP joint fusion in severe cases. This is primarily for PIP joint pathology, but access often involves MTP joint capsulotomy.
-
Fusion of Metatarsophalangeal Joints (Arthrodesis):
- Severe MTP Joint Arthritis: End-stage degenerative or inflammatory arthritis with intractable pain.
- Flail Toes / Neuropathic Toes: To provide stability and improve shoe wear in cases of severe instability or neuromuscular imbalance.
- Recurrent MTP Dislocation: Unreducible or recurrent dislocations after failed soft tissue procedures.
- Revision Surgery: For failed previous MTP joint procedures.
-
Capsulotomy of Metatarsophalangeal Joints:
- MTP Joint Contracture: Release of a tight dorsal capsule to improve plantarflexion or correct hyperextension deformities (e.g., dorsal bunionette, claw toe apex).
- MTP Joint Instability: Dorsal capsular plication for mild instability, often combined with plantar plate repair.
-
Muscle Tenotomy:
- Extensor Tendon Contracture: Lengthening or tenotomy of the extensor digitorum longus (EDL) and/or brevis (EDB) to address hammertoe/claw toe deformities at the MTP joint level, often performed in conjunction with other bony procedures.
-
Neurectomy:
- Interdigital Neuroma (Morton's Neuroma): While often approached through a dorsal incision in the web space, the dorsal approach to the MTP joint can provide access for neurectomy, particularly if concomitant MTP pathology is being addressed.
Contraindications
- Active Infection: Absolute contraindication; surgical debridement and antibiotic treatment required first.
- Severe Peripheral Vascular Disease: Compromised vascularity increases risk of wound healing complications and necrosis.
- Severely Compromised Soft Tissue Envelope: Inadequate skin coverage or chronic ulceration.
- Uncontrolled Diabetes Mellitus: Increased risk of infection and delayed wound healing.
- Severe Neuropathy/Insensate Foot: Increased risk of Charcot arthropathy or unrecognized complications.
- Extensive Plantar Scarring: While the dorsal approach avoids plantar scarring, existing severe plantar scarring or pathology might necessitate a specific plantar approach if the dorsal access is insufficient or inappropriate for the primary pathology.
- Patient Non-compliance: Inability to adhere to post-operative weight-bearing restrictions or rehabilitation protocols.
Table: Operative vs. Non-Operative Indications for Lesser MTP Joint Pathology
| Pathology Type | Operative Indications (via Dorsal Approach) | Non-Operative Indications |
|---|---|---|
| Hammertoe/Claw Toe | Rigid deformity, MTP hyperextension, painful callosities, failed conservative management, MTP joint instability. | Flexible deformity, mild symptoms, accommodative footwear, padding, toe exercises, splinting. |
| Freiberg's Infraction | Stages III-V (advanced collapse/arthritis), intractable pain, significant functional impairment. | Stages I-II (early changes), mild/intermittent pain, activity modification, stiff-soled shoes, orthotics. |
| MTP Joint Instability | Chronic pain, subluxation/dislocation, plantar plate tear (requiring repair or osteotomy), failed conservative management. | Mild instability, intermittent pain, taping, stiff-soled shoes, activity modification. |
| Refractory Metatarsalgia | Persistent localized pain under metatarsal head despite comprehensive conservative care (orthotics, injections, shoe modifications). | Mild to moderate pain, pain responsive to orthotics, shoe modifications, activity modification, NSAIDs. |
| MTP Joint Arthritis | End-stage pain, significant functional limitation, failed conservative management. | Mild to moderate pain, anti-inflammatory medications, injections, activity modification, stiff-soled shoes. |
| Interdigital Neuroma | Persistent pain/paresthesia despite conservative measures (orthotics, injections, shoe modification). | Initial presentation, mild/intermittent symptoms, responsive to conservative measures. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential for a successful outcome and to minimize complications.
Pre-Operative Planning
-
Clinical Assessment:
- Detailed History: Pain characteristics, duration, aggravating/alleviating factors, previous treatments, functional limitations, shoe wear issues.
- Physical Examination: Assess toe alignment, MTP joint range of motion (passive and active), reducibility of deformity, presence of callosities, neurovascular status (pulses, sensation), and assessment for any associated deformities (e.g., hallux valgus, pes planus). Specific tests for MTP joint instability (e.g., drawer test, vertical stress test) should be performed.
-
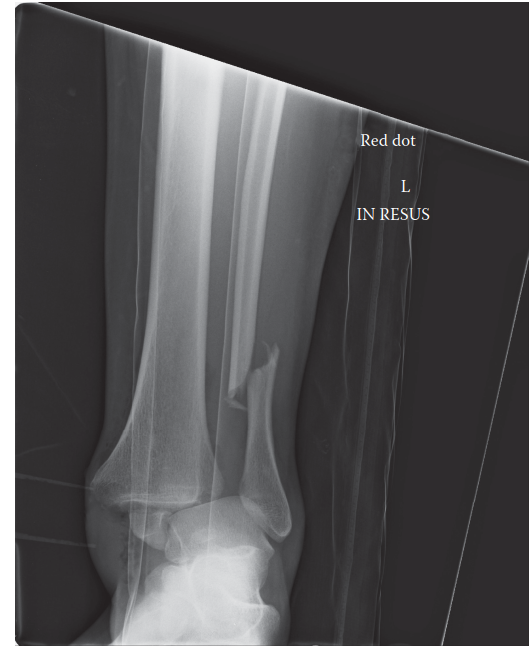
Imaging Studies:
- Weight-Bearing Radiographs: Essential. Anteroposterior (AP), lateral, and oblique views of the foot. Assess MTP joint alignment, metatarsal length parity, presence of arthritis, osteophytes, Freiberg's changes, and any pre-existing hardware.
- Stress Radiographs: May be useful in assessing MTP joint instability.
- MRI: Indicated for suspected plantar plate tears, synovitis, osteomyelitis, or complex soft tissue pathology (e.g., differentiating neuroma from other causes of metatarsalgia).
- CT Scan: Rarely needed, but useful for complex bony deformities, nonunion assessment, or pre-operative templating for arthrodesis in select cases.
-
Surgical Strategy:
- Determine the specific procedure(s) required (e.g., osteotomy, fusion, head excision, soft tissue release).
- Plan the exact incision placement and length.
- Select appropriate implants (e.g., K-wires, screws, plates) if internal fixation is anticipated.
- Anticipate potential challenges, such as severe stiffness, previous surgery, or poor bone quality.
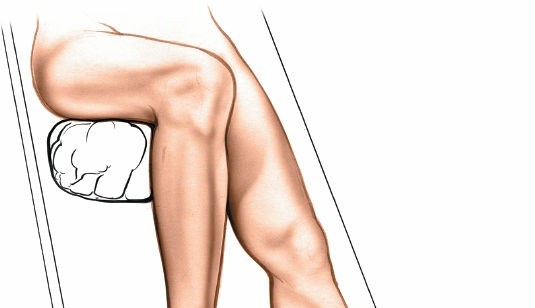
Patient Positioning
The patient is typically positioned supine on the operating table.
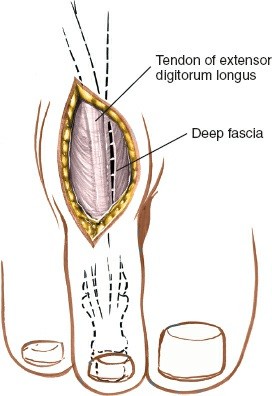
Figure: Patient positioned supine on the operating table with the affected foot draped and prepared for surgery. A tourniquet is applied proximally on the thigh or ankle.
- Anesthesia: General anesthesia or regional anesthesia (e.g., popliteal block, ankle block) is appropriate.
- Tourniquet: A pneumatic tourniquet is applied to the thigh or ankle to ensure a bloodless field, which is critical for meticulous dissection and identification of delicate neurovascular structures. The duration of tourniquet inflation should be monitored.
- Foot Preparation: The foot is prepped and draped in a sterile fashion, typically from the toes to the mid-calf.
- Foot Position: The foot is positioned at the end of the operating table, allowing for full range of motion and easy access to the dorsal aspect of the MTP joints. The knee may be flexed to allow the sole of the foot to rest flat on the table, or the leg may be elevated slightly with a sterile support.
-
Landmarks:
- Palpate each metatarsal head by placing a thumb on the plantar surface and an index finger on the dorsal surface of the foot. Any skin callosities under the heads can indicate areas of unaccustomed weight-bearing and potential underlying pathology.
- Palpate the tendons of the extensor digitorum longus (EDL) and extensor digitorum brevis (EDB) muscles on the dorsal aspect of the foot. These serve as crucial guides for incision planning and dissection.
Detailed Surgical Approach / Technique
The dorsal approach provides excellent exposure to the MTP joint. The technique involves a meticulous, layered dissection to minimize iatrogenic injury.
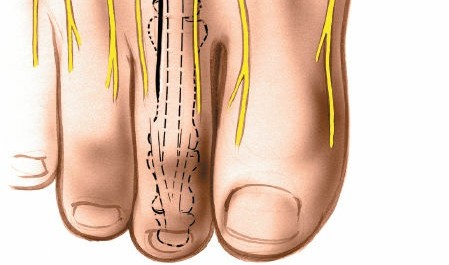
Landmarks and Incision
The incision must be carefully planned to provide adequate exposure while respecting critical neurovascular structures.
Figure: An example of a longitudinal skin incision planned for a dorsal approach to the second MTP joint, carefully placed to avoid crossing prominent neurovascular structures.
-
Incision Types:
- Longitudinal Incision: The most common approach for individual MTP joints (e.g., second MTP). It is centered over the affected MTP joint, typically in the intermetatarsal space or slightly medial/lateral to the extensor tendon, ensuring avoidance of the dorsal digital neurovascular bundles. For the second MTP, the incision is often placed just medial or lateral to the EDL tendon. Length typically 3-5 cm.
- Transverse Incision: Less commonly used for individual MTP joints but may be employed for cosmetic reasons or in cases where multiple adjacent MTP joints (e.g., 2nd, 3rd, 4th) need to be accessed through a single, broader incision. Care must be taken to avoid tension across the incision.
- Midline Extensor Tendon Incision: Directly over the extensor tendon for specific procedures like tenotomy or direct capsular access if the tendon is being split.
- Adjacent Joint Exposure: If two adjacent joints need to be exposed (e.g., 2nd and 3rd MTPs), a single longer longitudinal incision can be made in the intermetatarsal space between them, allowing retraction of the soft tissues to access both joints. Alternatively, two separate longitudinal incisions can be used to minimize soft tissue stripping.

Figure: Depiction of skin incisions for dorsal approaches. A single longitudinal incision (A) for a solitary MTP joint, or a longer incision (B) in the intermetatarsal space for multiple adjacent joints, as shown between the second and third MTPs.
Step-by-Step Dissection
-
Skin Incision and Subcutaneous Layer:
- Make the skin incision with a #15 scalpel, ensuring it is perpendicular to the skin to avoid beveling.
- Carefully dissect through the subcutaneous fat using a scalpel or Metzenbaum scissors. The dorsal digital nerves and veins course within this layer. Identify and meticulously protect these structures. Retract them gently using small blunt retractors or vessel loops. The dorsal veins are often ligated or cauterized if they obstruct the field.
-
Extensor Tendon Layer:
- Identify the extensor digitorum longus (EDL) tendon and often the extensor digitorum brevis (EDB) tendon.
- For most procedures, the EDL tendon is retracted. If a longitudinal incision was made just medial or lateral to the tendon, retract it to the opposite side.
- If the incision was made directly over the tendon, a longitudinal split in the EDL tendon may be performed, especially for capsulotomy or arthrodesis. The split should be carefully repaired at closure. Alternatively, the tendon can be detached distally and repaired later. For hammertoe correction, an EDL tenotomy may be performed proximally to the MTP joint.
- The extensor hood mechanism, including the sagittal bands, will be encountered. These may need to be incised longitudinally to expose the joint capsule.
-
Joint Capsule Exposure:
- Once the extensor tendons and hood are retracted or incised, the MTP joint capsule is exposed.
-
Capsulotomy:
A longitudinal, transverse, or H-shaped capsulotomy can be performed.
- Longitudinal: A straight incision along the dorsal midline of the joint provides direct access.
- Transverse: Often used for MTP joint fusions or for extensive exposure of the metatarsal head.
- H-shaped: Allows for elevation of dorsal capsular flaps, providing good visualization and facilitating subsequent repair or plication for instability.
- Elevate the capsular flaps and carefully excise any dorsal osteophytes to improve exposure.
- Maintain careful hemostasis throughout, as the joint capsule has a rich blood supply.
Specific Procedures (via Dorsal Approach)
1. Excision of Metatarsal Heads
- Indication: Severe Freiberg's infraction, advanced MTP arthritis, intractable metatarsalgia.
-
Technique:
After capsulotomy, hyperflex the toe to expose the metatarsal head. Use an osteotome or sagittal saw to resect the distal metatarsal head. The amount of bone resected depends on the pathology and desired outcome (e.g., typically 5-8 mm for a Weil osteotomy, or complete head excision for severe arthritis). Ensure smooth bone edges to prevent impingement.

Figure: Intraoperative view during metatarsal head excision. The MTP joint is exposed, and the diseased or prominent metatarsal head is resected using a saw.
2. Distal Metatarsal Osteotomy (e.g., Weil Osteotomy)
- Indication: Overlength metatarsal, plantar plate pathology, MTP joint instability, metatarsalgia.
- Technique: After joint exposure, identify the metatarsal neck. Using a sagittal saw, perform an osteotomy in a controlled manner, typically parallel to the weight-bearing surface and angled slightly dorsal-proximal to plantar-distal. The amount of shortening is measured and removed. The distal fragment is then translated proximally.
-
Fixation:
Secure the osteotomy with a small screw (e.g., 2.0 mm or 2.7 mm cortical screw) or K-wire to maintain the desired shortening and plantarflexion.
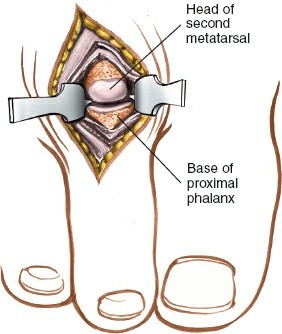
Figure: Surgical technique for a distal metatarsal osteotomy (e.g., Weil osteotomy). The osteotomy is performed, and the fragment is translated and then stabilized with internal fixation.
3. Partial Proximal Phalangectomy / PIP Joint Arthroplasty
- Indication: Rigid hammertoe/claw toe deformity, often for the PIP joint but accessed through the MTP approach.
-
Technique:
The MTP joint is exposed. For a rigid hammertoe, the MTP joint is often dorsiflexed to expose the PIP joint indirectly. A dorsal longitudinal incision over the PIP joint itself may also be used in conjunction. Resection of a portion of the proximal phalanx head (for PIP arthroplasty) aims to correct the PIP flexion deformity.
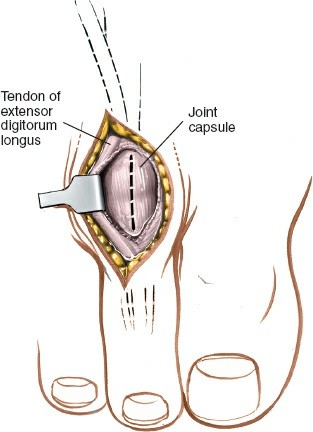
Figure: Resection of the proximal phalanx head for a PIP joint arthroplasty, often performed as part of a hammertoe correction. The joint capsule and collateral ligaments are released.
4. Fusion of Metatarsophalangeal Joints (Arthrodesis)
- Indication: End-stage arthritis, severe instability, neuropathic joint, failed previous surgery.
- Technique: After exposing the MTP joint, resect the articular cartilage from both the metatarsal head and the base of the proximal phalanx, creating cancellous bone surfaces. Shape the surfaces for optimal contact (e.g., convex-concave, chevron, or flat-on-flat). Position the toe in slight plantarflexion (typically 10-15 degrees) to allow for ground clearance and proper shoe wear.
-
Fixation:
Secure the fusion site with K-wires, interfragmentary screws, or a dorsal plate and screws.

Figure: Example of MTP joint fusion with internal fixation. The articular surfaces are prepared, the joint is positioned, and then compressed and stabilized with a dorsal plate and screws.
5. Capsulotomy of Metatarsophalangeal Joints
- Indication: MTP joint contracture, dorsal bunionette.
- Technique: After exposure, perform a precise longitudinal or transverse incision of the dorsal MTP joint capsule to release contracture and allow for increased plantarflexion. Ensure release of any tight collateral ligaments if necessary.
6. Muscle Tenotomy
- Indication: Extensor contracture in hammertoe/claw toe.
- Technique: Proximal to the MTP joint, isolate the EDL tendon. Perform a Z-lengthening or complete tenotomy, depending on the severity of contracture. For complete tenotomy, ensure adequate lengthening and check for passive correction of the deformity. The EDB tendon may also require tenotomy.
7. Neurectomy (Interdigital Neuroma)
- Indication: Symptomatic interdigital neuroma. While often through a specific dorsal web space incision, it can be combined.
- Technique: Access the intermetatarsal space. Identify the interdigital nerve and resect the neuroma proximally to the DTML to bury the stump in soft tissue or muscle. Protect adjacent neurovascular structures.
Closure
- Capsular Repair: If a capsulotomy was performed and the capsule is healthy, repair it with absorbable sutures (e.g., 2-0 or 3-0 absorbable suture). This helps restore joint stability. If dorsal capsular plication is indicated for instability, perform it at this stage.
- Extensor Tendon Repair: If the EDL tendon was split or detached, repair it with non-absorbable or absorbable sutures (e.g., 2-0 or 3-0 non-absorbable) under appropriate tension. If a tenotomy was performed, no repair is necessary.
- Subcutaneous Layer: Close the subcutaneous layer with interrupted absorbable sutures (e.g., 3-0 or 4-0 absorbable) to obliterate dead space and reduce tension on the skin.
-
Skin Closure:
Close the skin with non-absorbable sutures (e.g., 3-0 or 4-0 nylon) using an interrupted or running subcuticular technique.
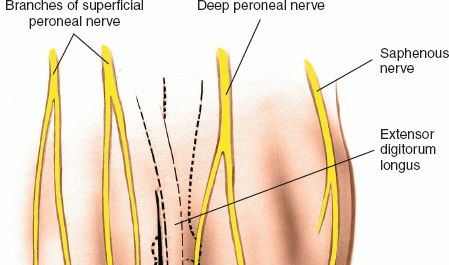
Figure: Final skin closure after a dorsal MTP joint procedure. The incision is meticulously closed in layers to minimize scar formation. - Dressing: Apply a sterile, non-compressive dressing, typically involving cotton between the toes to maintain alignment, and a soft compressive dressing around the forefoot. Splinting or taping may be used to maintain toe position, especially after hammertoe correction or fusion.
Complications & Management
Despite meticulous surgical technique, complications can arise. Recognition and appropriate management are crucial for optimal outcomes.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (Approx.) | Management Strategy | Salvage Strategy |
|---|---|---|---|
| Infection | 1-5% | Superficial: Oral antibiotics, local wound care. Deep: Surgical debridement, intravenous antibiotics, wound culture, possible implant removal. | Persistent deep infection: Repeat debridement, long-term antibiotics, flap coverage, MTP fusion (if joint preservation initially failed), or in severe cases, amputation. |
| Neurovascular Injury | <1% (nerve) | Dorsal digital nerve neurapraxia: Observation, nerve protection, pain management. Laceration: Primary repair (micro-neurosurgical), neurolysis if entrapment. Vascular injury: Direct repair, ligation (if collateral circulation sufficient), or vascular consultation. | Persistent painful neuroma: Surgical neuroma excision (proximal burial), targeted nerve cryoablation or radiofrequency ablation. Chronic paresthesia/dysesthesia: Pain management specialist referral. |
| Metatarsalgia (Transfer) | 5-20% | Post-operative plantar callosities/pain under adjacent metatarsal heads due to altered load. Initial management: Orthotics, shoe modifications, metatarsal pads. | Persistent/severe transfer metatarsalgia: Revision surgery with osteotomy of the adjacent offending metatarsal (e.g., Weil osteotomy), possibly requiring revision of the initial procedure. |
| Stiffness/Reduced ROM | 5-15% | Post-operative scarring, prolonged immobilization. Initial management: Physical therapy, manual mobilization, stretching exercises. | Persistent stiffness impacting function: Manipulation under anesthesia, arthrolysis, capsular release, tenolysis. In severe cases, consideration of arthrodesis or implant removal. |
| Recurrence of Deformity | 5-10% | Inadequate correction, persistent muscle imbalance, plantar plate insufficiency. Initial management: Taping, bracing, orthotics. | Persistent or severe recurrence: Revision surgery (e.g., repeat osteotomy, MTP fusion, plantar plate repair), often addressing contributing factors like metatarsal length or soft tissue imbalance. |
| Nonunion/Malunion (Fusion) | 5-15% (fusion) | Nonunion: Delayed weight-bearing, bone stimulation. Malunion: Mild malalignment - accommodative footwear, orthotics. | Nonunion: Revision fusion with bone grafting, stable internal fixation. Symptomatic malunion: Corrective osteotomy and refusion. |
| Hardware Complications | 2-10% | Prominent hardware (painful): Hardware removal once bone healing is complete. Breakage: Removal and potential revision surgery if healing is compromised. Infection: See "Infection" above. | Hardware removal and management of any underlying bone pathology (e.g., nonunion requiring further fixation). |
| Swelling/Edema | Common | Prolonged and excessive. Initial management: Elevation, compression, gentle range of motion exercises, anti-inflammatory medication. | Persistent edema with skin changes: Lymphatic massage, referral to lymphedema specialist. Rule out DVT/infection. |
| Complex Regional Pain Syndrome (CRPS) | <1% | Early recognition. Initial management: Aggressive pain management, physical therapy, nerve blocks, multidisciplinary approach. | Persistent CRPS: Specialized pain clinic management, spinal cord stimulators, psychological support. |
| DVT/PE | Rare | Prophylaxis (early mobilization, chemical if high risk). Suspected DVT: Duplex ultrasound, anticoagulation. Suspected PE: CT pulmonary angiography, anticoagulation. | Long-term anticoagulation, management of post-thrombotic syndrome. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is critical for optimizing outcomes, restoring function, and preventing recurrence. Protocols vary based on the specific procedure performed, patient factors, and surgeon preference.
General Principles
- Pain Management: Multimodal analgesia (oral opioids, NSAIDs, acetaminophen, nerve blocks if still effective) is crucial to facilitate early mobilization and patient comfort.
- Edema Control: Strict elevation of the operative foot above heart level, especially for the first 1-2 weeks. Compression dressings and early gentle ankle range of motion exercises help reduce swelling.
- Wound Care: Incision kept clean and dry. Dressings changed as per surgeon's instruction, typically at 1-2 weeks post-op. Sutures or staples removed at 2-3 weeks.
- Protection: The operative foot is protected in a post-operative shoe, surgical boot, or cast as indicated.
Specific Protocols by Procedure Type
1. Distal Metatarsal Osteotomy (e.g., Weil Osteotomy)
-
Weeks 0-2:
- Weight-Bearing (WB): Partial weight-bearing (PWB) in a rigid-soled post-operative shoe or surgical boot, initially focusing on heel-walking. Some surgeons allow immediate full weight-bearing (FWB) in a boot, if stability is good.
- Motion: Gentle passive and active range of motion (ROM) of the MTP joint, starting after 1 week if soft tissue healing allows. Avoid excessive dorsiflexion.
- Dressing: Soft compressive dressing, protective cotton between toes.
-
Weeks 2-6:
- WB: Progress to FWB in post-operative shoe/boot.
- Motion: Continue MTP ROM exercises, focusing on regaining plantarflexion and dorsiflexion within pain limits. Gentle manual mobilization.
- Activity: Avoid high-impact activities.
-
Weeks 6-12:
- WB: Transition to wide, comfortable athletic shoes. Orthotics may be prescribed if needed.
- Motion: Progressive strengthening and flexibility exercises for the forefoot and ankle.
- Activity: Gradually return to activities of daily living. Low-impact exercise may begin.
-
3+ Months:
- Return to sport and higher-impact activities, guided by pain, swelling, and functional recovery.
2. MTP Joint Fusion (Arthrodesis)
-
Weeks 0-6:
- WB: Non-weight-bearing (NWB) or touch-down weight-bearing (TDWB) in a cast or surgical boot. K-wires (if used) are typically removed at 4-6 weeks, if fusion is consolidated.
- Motion: No MTP joint motion. Maintain ROM of ankle and IP joints.
- Radiographs: Follow-up X-rays at 4-6 weeks to assess for early signs of fusion.
-
Weeks 6-12:
- WB: Progress to PWB in a walking boot, then to FWB in a rigid-soled shoe, as radiographic evidence of fusion allows.
- Motion: No forced MTP motion.
- Activity: Gradually increase activity level, avoiding high impact.
-
3-6+ Months:
- Transition to comfortable, wide-toed shoes. Continue with low-impact activities. Fusion typically takes 3-6 months or longer to fully consolidate.
3. Excision of Metatarsal Head / Partial Proximal Phalangectomy
-
Weeks 0-2:
- WB: PWB in a rigid-soled post-operative shoe or surgical boot.
- Motion: Gentle passive MTP ROM exercises, focusing on preventing stiffness.
-
Weeks 2-6:
- WB: Progress to FWB in a post-operative shoe/boot.
- Motion: Continue MTP ROM exercises.
-
Weeks 6-12:
- WB: Transition to wide, comfortable athletic shoes.
- Activity: Gradual return to activities.
4. Soft Tissue Procedures (Capsulotomy, Tenotomy, Neurectomy)
-
Weeks 0-2:
- WB: PWB as tolerated in a rigid-soled post-operative shoe.
- Motion: Gentle passive and active ROM, particularly to maintain the corrected position after tenotomy/capsulotomy.
-
Weeks 2-6:
- WB: FWB in a post-operative shoe, then transition to comfortable athletic shoes.
- Motion: Progressive MTP ROM and gentle strengthening.
-
6+ Weeks:
- Return to full activity as tolerated.
Overall Goal: The rehabilitation process is tailored to the individual, aiming to restore pain-free function, optimize MTP joint mechanics, and ensure long-term stability and comfort. Patient education regarding activity modification, proper footwear, and adherence to physical therapy is paramount.
Summary of Key Literature / Guidelines
The dorsal approach to the lesser MTP joints is a well-established technique supported by extensive orthopedic literature, particularly for hammertoe correction, metatarsal osteotomies, and MTP joint stabilization.
1. Metatarsal Osteotomies (Weil Osteotomy):
* The
Weil osteotomy
, a distal oblique shortening osteotomy of the metatarsal, is one of the most widely studied procedures performed via a dorsal approach. Initial studies by Weil (1995) demonstrated its effectiveness in correcting metatarsalgia and MTP joint instability.
* Literature supports its efficacy in reducing plantar pressure beneath the resected metatarsal head. However,
transfer metatarsalgia
to adjacent metatarsals remains a documented complication, with reported incidences varying from 5% to 20%. Studies emphasize precise shortening and appropriate plantarflexion of the metatarsal head to minimize this risk.
* The impact of
fixation
(screw vs. K-wire) on union rates and recurrence has been studied, with screws generally offering more stable fixation, potentially allowing earlier weight-bearing.
2. Hammertoe and Claw Toe Correction:
* Dorsal approaches are fundamental for
proximal interphalangeal (PIP) joint arthroplasty
(resection of the proximal phalanx head) or
arthrodesis
in rigid hammertoe deformities.
* For complex
MTP joint hyperextension/dorsal subluxation
component of claw toes, the dorsal approach allows for direct visualization and release of the dorsal capsule and extensor tendons (extensor tenotomy/lengthening) and concomitant metatarsal osteotomy (e.g., Weil) to decompress the MTP joint.
* Outcomes generally report high patient satisfaction, pain relief, and improved shoe wear, though residual stiffness and recurrence remain potential issues.
3. MTP Joint Instability and Plantar Plate Pathology:
* While direct plantar plate repair is traditionally approached plantarly, many surgeons utilize the dorsal approach for
indirect management
of MTP joint instability, especially for the second MTP.
* This involves
distal metatarsal shortening osteotomy (Weil)
to decompress the joint and allow the plantar plate to assume its normal load-bearing position. Concomitant
dorsal capsular plication
(tightening) and
extensor tendon lengthening
can be performed.
* Comparative studies evaluating dorsal osteotomy-based techniques versus direct plantar plate repair are ongoing, with both showing favorable results depending on the severity and chronicity of the instability. The dorsal approach avoids plantar scarring but does not directly address the plantar plate tear itself unless specific modifications are made.
4. MTP Joint Arthrodesis:
* The dorsal approach is the standard for MTP joint fusion for severe arthritis, instability, or neuropathic deformities.
* Literature confirms high fusion rates (typically >90%) with appropriate surgical technique and stable internal fixation. Functional outcomes are generally good, with patients reporting pain relief and improved stability for shoe wear.
* Complications such as nonunion or malunion are well-documented, emphasizing the importance of meticulous joint preparation and appropriate positioning (slight plantarflexion, minimal valgus).
5. General Considerations and Guidelines:
*
Avoidance of Plantar Skin:
A consistent theme in the literature is the advantage of the dorsal approach in minimizing plantar scarring, neuroma formation, and potential dysesthesias in weight-bearing areas.
*
Neurovascular Protection:
Emphasis on careful identification and retraction of dorsal digital nerves and veins is a recurring guideline across all described techniques.
*
Post-operative Management:
Standardized post-operative protocols incorporating elevation, early mobilization (where appropriate), and gradual weight-bearing progression are critical for preventing complications like stiffness, edema, and recurrence.
In conclusion, the dorsal approach to the second, third, and fourth MTP joints is a robust and versatile technique. While specific procedural outcomes vary, the general principles of precise surgical anatomy, meticulous dissection, and individualized post-operative rehabilitation are consistently highlighted as cornerstones for achieving optimal functional and symptomatic relief in patients with forefoot pathology. Continuous research aims to refine indications, surgical techniques, and long-term outcomes for these frequently encountered conditions.
Clinical & Radiographic Imaging
You Might Also Like