Essential Anterior & Posterior Approaches to the Medial Malleolus
Key Takeaway
We review everything you need to understand about Essential Anterior & Posterior Approaches to the Medial Malleolus. The anterior and posterior approaches to the medial malleolus are primarily employed for open reduction and internal fixation of medial malleolar fractures, providing excellent visualization. The anterior incision offers a view of the anteromedial ankle joint and talus dome, whereas the posterior incision facilitates fracture fixation and visualization of the posterior tibia margin.
Essential Anterior & Posterior Approaches to the Medial Malleolus
Introduction & Epidemiology
Medial malleolar fractures represent a critical component of ankle trauma, frequently occurring in isolation or as part of more complex ankle fracture patterns (bimalleolar, trimalleolar, or pilon fractures). The medial malleolus, an integral part of the distal tibia, serves as the primary bony buttress to the talus medially and is the critical attachment site for the deltoid ligament complex. Displaced fractures of the medial malleolus disrupt the ankle mortise, leading to instability, incongruity of the talotibial articulation, and a propensity for post-traumatic osteoarthritis if not adequately managed.
Epidemiologically, ankle fractures are among the most common skeletal injuries, with an incidence of approximately 187 per 100,000 person-years. Medial malleolar involvement is seen in a significant proportion of these injuries, varying from 20% in isolated medial malleolus fractures to nearly all bimalleolar and trimalleolar fractures. The primary goal of surgical intervention for displaced medial malleolar fractures is anatomical reduction and stable internal fixation to restore the integrity of the ankle mortise, facilitate early mobilization, and minimize long-term sequelae.
The choice of surgical approach to the medial malleolus is dictated by the fracture morphology, degree of displacement, associated injuries (e.g., posterior malleolus involvement, syndesmotic injury), and surgeon preference. The anterior and posterior approaches are the predominant surgical corridors for open reduction and internal fixation (ORIF) of medial malleolar fractures. Each offers distinct advantages in terms of exposure and allows for direct visualization of the fracture site, essential for achieving anatomical reduction and secure fixation. The anterior approach typically provides excellent visualization of the anteromedial aspect of the malleolus and ankle joint, while the posterior approach is particularly advantageous for fractures with significant posterior extension or a large posterior malleolar component requiring a combined strategy.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy surrounding the medial malleolus is paramount to successful operative intervention and avoidance of complications.
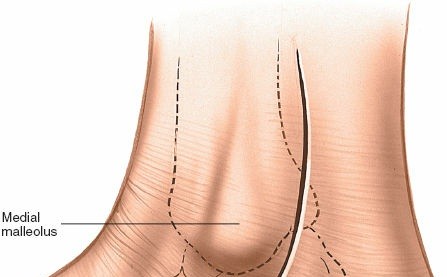
Bony Anatomy
The medial malleolus is the distal projection of the tibia on its medial aspect. It is approximately 2 cm in length and tapers distally. Its lateral surface is covered by hyaline cartilage, forming part of the ankle mortise and articulating with the medial facet of the talus. The medial malleolus has anterior and posterior colliculi, with the deep deltoid ligament inserting into the anterior colliculus and the superficial deltoid ligament inserting into the posterior colliculus and body of the malleolus. The superior aspect of the medial malleolus blends seamlessly with the distal tibial metaphysis. Fractures can occur at various levels, from the tip to the base, and can be transverse, oblique, vertical, or comminuted.
Ligamentous Anatomy
The deltoid ligament complex is a robust structure originating from the medial malleolus and fanning out to attach to the talus, navicular, and calcaneus. It is composed of superficial and deep components.
*
Superficial Deltoid Ligament:
Includes the tibiocalcaneal, tibionavicular, and tibiospring ligaments. These fibers provide stability against valgus stress and limit talar external rotation.
*
Deep Deltoid Ligament:
Consists of the anterior tibiotalar and posterior tibiotalar ligaments. These are the primary restraints to talar lateral displacement and external rotation, inserting into the medial body and posterior process of the talus, respectively.
Medial malleolar fractures often involve avulsion of these ligamentous attachments, leading to significant ankle instability.
Neurovascular Structures
Understanding the course of neurovascular structures is critical to minimize iatrogenic injury.
*
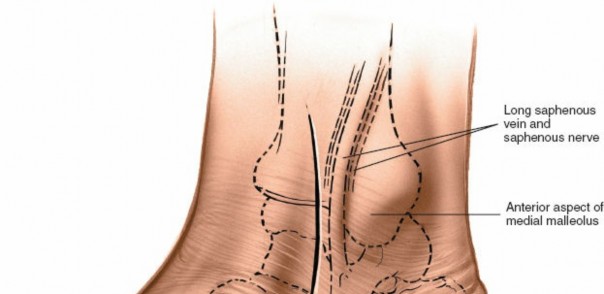
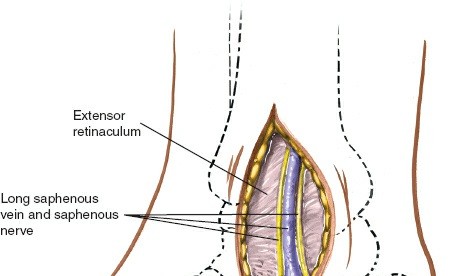
Saphenous Nerve and Great Saphenous Vein:
These structures run anteromedially to the medial malleolus. The saphenous nerve is a sensory nerve supplying the skin over the medial aspect of the leg and ankle. The great saphenous vein typically courses anterior to the medial malleolus. Both are vulnerable during anterior approaches and medial incisions.
*
Posterior Tibial Neurovascular Bundle:
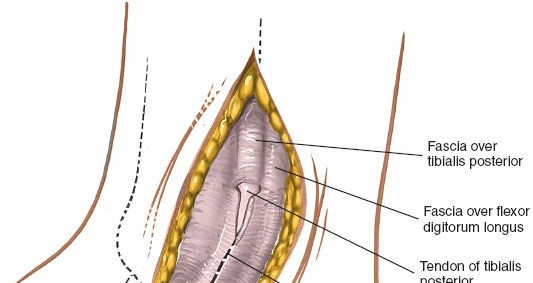
Located posteromedial to the ankle joint, within the tarsal tunnel. From anterior to posterior, the structures are the posterior tibial tendon (PTT), flexor digitorum longus (FDL) tendon, posterior tibial artery, posterior tibial nerve, and flexor hallucis longus (FHL) tendon. These structures are at risk during posterior (posteromedial) approaches.
Tendons
Three major tendons course around the medial malleolus:
*
Tibialis Posterior Tendon:
Passes directly behind the medial malleolus within its own sheath, attaching primarily to the navicular and cuneiforms.
*
Flexor Digitorum Longus Tendon:
Lies posterior to the tibialis posterior tendon, deep within the tarsal tunnel.
*
Flexor Hallucis Longus Tendon:
The most posterior of the three, located deepest within the tarsal tunnel.
Retraction of these tendons is often necessary during posterior approaches, requiring careful handling to prevent injury to their vascular supply and tenosynovium.
Biomechanics
The medial malleolus and its associated deltoid ligament complex are crucial for maintaining ankle mortise stability and resisting abnormal talar motion, particularly valgus and external rotation forces. Displaced medial malleolar fractures disrupt the bony buttress effect and compromise the deltoid ligament's function, leading to a widened mortise and potential for talar subluxation. Accurate reduction of the medial malleolus restores the anatomical congruity of the talotibial joint, allowing for proper load transmission and preventing abnormal stresses that can lead to early degenerative changes. Furthermore, stable fixation permits early motion, which is essential for cartilage health and prevention of stiffness.
Indications & Contraindications
The decision for operative versus non-operative management of medial malleolar fractures hinges on fracture stability, displacement, associated injuries, and patient factors.
Indications for Operative Fixation (ORIF)
- Displaced Fractures: Displacement of the medial malleolar fragment greater than 2 mm, especially if there is an articular step-off.
- Rotational Instability: Fractures demonstrating rotational instability despite fibular fixation (in bimalleolar injuries).
- Irreducible Talar Subluxation: Persistent talar subluxation or incongruity of the ankle mortise after closed reduction maneuvers.
- Open Fractures: All open fractures of the medial malleolus warrant surgical debridement and internal fixation, provided soft tissue conditions allow.
- Medial Malleolar Avulsion with Deep Deltoid Rupture: Avulsion fractures of the medial malleolus associated with persistent talar shift due to deep deltoid ligament disruption.
- Entrapped Soft Tissue: Interposition of soft tissue (e.g., tibialis posterior tendon, periosteum) within the fracture site preventing anatomical reduction.
- Vertical Shear Fractures: Often unstable and prone to nonunion, requiring stable fixation, frequently with a buttress plate.
- Associated Posterior Malleolar Fractures: Large posterior malleolar fragments (typically >25% of articular surface or >2 mm displacement) often necessitate a posterior approach, which can be combined with a medial approach or managed through a posteromedial incision that allows access to both.
- Syndesmotic Instability: While primarily addressed via fibular and syndesmotic fixation, a stable medial malleolus is crucial for overall ankle stability.
Contraindications for Operative Fixation
-
Absolute Contraindications:
- Severe active infection at the surgical site.
- Severe soft tissue compromise (e.g., extensive skin necrosis, large open wounds unsuitable for primary closure) that precludes safe surgical exposure and closure.
- Severe peripheral vascular disease with questionable wound healing potential.
- Anesthetic contraindications due to severe medical comorbidities.
-
Relative Contraindications:
- Non-displaced or minimally displaced fractures (<2 mm) that are stable and maintain ankle mortise congruity.
- Significant patient comorbidities that substantially increase surgical risk (e.g., uncontrolled diabetes, severe osteopenia, severe peripheral neuropathy).
- Poor patient compliance or inability to adhere to post-operative rehabilitation protocols.
- Pre-existing severe neuropathy leading to a Charcot joint or insensate foot.
Table 1: Operative vs. Non-Operative Indications for Medial Malleolar Fractures
| Indication Type | Operative | Non-Operative |
|---|---|---|
| Fracture Displacement | >2 mm displacement or articular step-off | Undisplaced or minimally displaced (<2 mm) |
| Ankle Stability | Ankle instability after fibular fixation or persistent talar subluxation | Stable ankle mortise, intact deltoid ligament function |
| Articular Congruity | Articular incongruity leading to joint space widening or loss of parallel joint surfaces | Congruent joint surface, no significant widening of the medial clear space |
| Associated Injuries | Open fractures, irreducible talar subluxation, significant posterior malleolar component, trapped soft tissue | Isolated, stable fracture without significant associated soft tissue or bony injuries |
| Fracture Pattern | Vertical shear, comminuted, long oblique fractures, or avulsions leading to instability | Transverse, small avulsion fractures, or stable oblique patterns amenable to closed reduction and immobilization |
| Patient Factors | Medically fit, good surgical candidate, high functional demands | Significant comorbidities, severe osteopenia, poor skin integrity, low functional demands |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is crucial for optimizing outcomes and minimizing complications.
Clinical Assessment
A thorough history and physical examination are essential. Assess the skin integrity for any blistering, abrasions, or open wounds. Evaluate neurovascular status, including dorsalis pedis and posterior tibial pulses, and sensory examination of the foot. Document any pre-existing medical conditions, allergies, and current medications.
Imaging
- Standard Ankle Radiographs: Anteroposterior (AP), mortise, and lateral views are the initial imaging modalities. These help to identify the fracture pattern, degree of displacement, and presence of associated injuries (e.g., fibular fracture, posterior malleolus fracture, syndesmotic widening).
- Computed Tomography (CT) Scan: Highly recommended for complex fracture patterns, significant articular involvement, comminution, or suspected posterior malleolar fractures. CT provides detailed 3D information, aiding in surgical planning, especially for evaluating articular step-off and fragment size/orientation.
- Magnetic Resonance Imaging (MRI): Less commonly used in acute fracture management but may be indicated if significant ligamentous injury (e.g., deep deltoid rupture without bony avulsion) or occult osteochondral lesions are suspected.
Surgical Planning
Based on the clinical and imaging assessment, a detailed surgical plan is formulated:
1.
Choice of Approach:
*
Anterior Approach:
Preferred for transverse or short oblique fractures, particularly those in the lower or mid-malleolar region, allowing excellent visualization of the medial articular surface and talar dome.
*
Posterior (Posteromedial) Approach:
Ideal for vertical or long oblique medial malleolar fractures that extend proximally or posteriorly, often associated with a larger posterior malleolar fragment. It provides direct visualization of the posteromedial aspect of the tibia and facilitates fixation from posterior to anterior.
* For extensive comminution or involvement of both anterior and posterior aspects of the malleolus, a single comprehensive approach is usually preferred over dual incisions if adequate access can be obtained.
2.
Fixation Strategy:
*
Lag Screws:
Typically 3.5 mm or 4.0 mm partially threaded cannulated or non-cannulated screws. Used for most simple transverse or oblique fractures, inserted perpendicular to the fracture line to achieve interfragmentary compression.
*
Tension Band Wiring:
Effective for small avulsion fractures or comminuted tip fragments, particularly in conjunction with a K-wire.
*
Medial Buttress Plate:
Indicated for vertical shear fractures, comminuted fractures, or osteoporotic bone where screw fixation alone may be insufficient. Plates can be placed anteriorly or posteromedially, depending on the fracture pattern and chosen approach.
* Consider the need for supplemental fixation for syndesmotic instability or fibular fractures.
3.
Hardware Selection:
Prepare appropriate instruments, screws (length and diameter), K-wires, drills, and possibly plates.
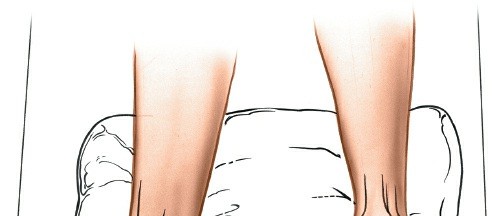
Patient Positioning
The patient is typically positioned supine on the operating table.
* For
anterior approaches
, the patient is positioned supine. A bolster can be placed under the ipsilateral hip to internally rotate the limb slightly, presenting the medial malleolus more anteriorly.
* For
posterior (posteromedial) approaches
, the patient can be positioned supine with the leg draped across the contralateral leg (allowing posterior access), or in a lateral decubitus position with the affected leg uppermost, or even in a prone position if significant posterior malleolus exposure is required. The choice depends on the surgeon's preference and the extent of posterior exposure needed.
* A tourniquet is applied high on the thigh.
* Image intensification (C-arm) should be readily available and positioned to obtain AP, mortise, and lateral views of the ankle without repositioning the patient.
* The limb is sterilely prepared and draped, ensuring freedom of movement for ankle positioning during reduction maneuvers.
Detailed Surgical Approach / Technique
Irrespective of the approach, general principles include tourniquet control, meticulous soft tissue handling, anatomical reduction, stable internal fixation, and layered wound closure.
General Principles
- Tourniquet Inflation: Inflate the thigh tourniquet to 250-300 mmHg (or 100 mmHg above systolic blood pressure) to create a bloodless field, which is essential for identifying anatomical structures and achieving precise reduction.
- Irrigation: Copious irrigation with sterile saline throughout the procedure helps to remove debris, dilute potential contaminants, and keep tissues moist.
- Soft Tissue Handling: Minimize retraction tension, avoid excessive electrocautery, and protect neurovascular structures to preserve soft tissue viability and reduce the risk of wound complications.
- Provisional Fixation: K-wires are invaluable for temporarily holding reduced fragments, allowing for confirmation of reduction with fluoroscopy before definitive fixation.
- Definitive Fixation: Choose appropriate hardware based on fracture pattern and bone quality, aiming for rigid fixation that allows early mobilization.
Anterior Approach to the Medial Malleolus
This approach provides excellent visualization of transverse, short oblique, or vertical fractures of the medial malleolus, particularly those involving the anteromedial aspect of the talar dome or capsule.
-
Incision:
- Make a longitudinal or slightly curvilinear incision centered over the medial malleolus, typically 5-8 cm in length.
- Start approximately 2-3 cm proximal to the tip of the medial malleolus and extend distally 2-3 cm below the tip, paralleling the anterior border of the malleolus.
-
Alternatively, the incision can be slightly more anterior to facilitate inspection of the anteromedial ankle joint.
 - Carefully incise the skin and subcutaneous tissue.
-
Dissection:
- Identify and protect the great saphenous vein and saphenous nerve. These structures typically course anterior to the incision or can be retracted anteriorly.
- Deepen the incision through the superficial fascia.
- The periosteum over the medial malleolus is then incised longitudinally directly over the fracture line.
-
Carefully elevate the periosteum with a small periosteal elevator to expose the fracture fragments. Avoid excessive stripping, which can compromise blood supply.
-
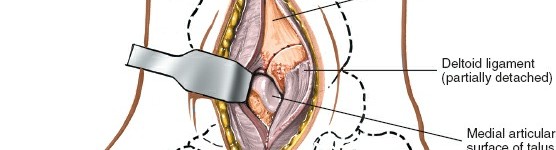
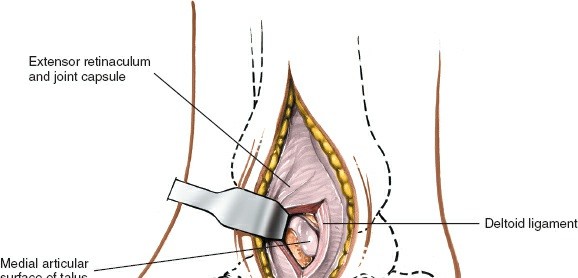
Exposure:
- With gentle retraction, the medial malleolus fracture fragments are exposed.
-
The anteromedial capsule of the ankle joint can be opened if necessary to inspect the articular surface of the talus and the joint congruity, especially in cases of talar dome injury or suspected interposed soft tissue.

-
Reduction:
- Inspect the fracture site for any interposed soft tissue (e.g., periosteum, deltoid ligament fibers), which must be removed to achieve an anatomical reduction.
- Use small pointed reduction clamps, bone hooks, or K-wires to manipulate the fragments into anatomical alignment.
- Confirm reduction visually and with fluoroscopy (AP, mortise, and lateral views). Ensure there is no articular step-off or gap.
- Provisionally fix the reduced fragments with one or two K-wires, ensuring they do not interfere with definitive screw placement.
-
Fixation:
-
Lag Screws:
For most transverse or short oblique fractures, two 3.5 mm or 4.0 mm partially threaded cancellous screws are commonly used. These are inserted from the medial malleolar fragment into the distal tibial metaphysis, aiming perpendicular to the fracture line to maximize interfragmentary compression. Ensure screw length is adequate to engage the far cortex without excessively protruding.
 - Tension Band Wiring: For small avulsion fragments or highly comminuted tips not amenable to screw fixation, a tension band construct can be employed, using K-wires and a figure-of-eight wire loop.
-
Medial Buttress Plate:
For vertical shear fractures or highly comminuted patterns, a small medial buttress plate (e.g., 1/3 tubular plate, specialized medial malleolus plate) may be required. The plate is contoured to the medial malleolus and distal tibia, providing additional stability. Screws are placed through the plate to engage both the fragment and the main tibial shaft.
 -
Confirm final fixation and joint congruity with fluoroscopy.
-
Lag Screws:
For most transverse or short oblique fractures, two 3.5 mm or 4.0 mm partially threaded cancellous screws are commonly used. These are inserted from the medial malleolar fragment into the distal tibial metaphysis, aiming perpendicular to the fracture line to maximize interfragmentary compression. Ensure screw length is adequate to engage the far cortex without excessively protruding.
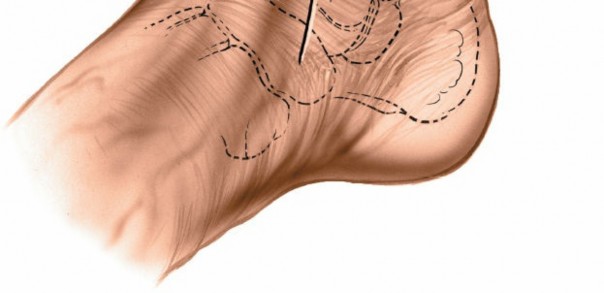
Posterior (Posteromedial) Approach to the Medial Malleolus
This approach is advantageous for vertical or long oblique medial malleolar fractures that extend proximally and/or posteriorly, or when there is an associated posterior malleolar fracture component requiring direct visualization and fixation.
-
Incision:
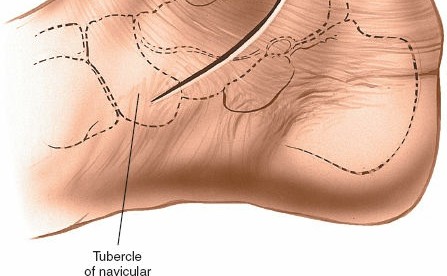
- Make a 10-cm curvilinear incision on the medial side of the ankle.
- Begin approximately 5 cm proximal to the ankle joint on the posterior border of the tibia.
- Curve the incision distally and anteriorly, following the posterior border of the medial malleolus.
-
Continue the curve below the malleolus to end approximately 5 cm distal to its tip. (This description closely matches the seed content).
 - Incise the skin and subcutaneous tissue.
-
Dissection:
- The saphenous vein and nerve are typically located more anteriorly and should be identified and protected, usually retracted anteriorly.
- Deepen the incision through the superficial fascia.
- The interval for this approach is typically between the posterior border of the tibia/medial malleolus and the tibialis posterior tendon sheath.
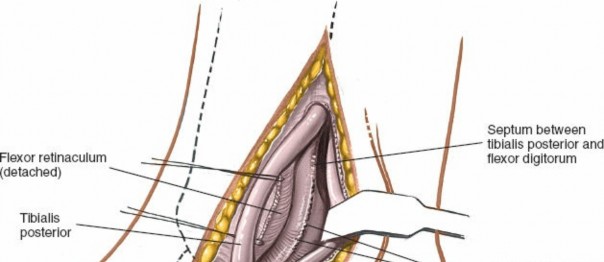
- The tibialis posterior tendon is identified and carefully retracted anteriorly/laterally. This exposes the posterior aspect of the medial malleolus and the distal tibia.
-
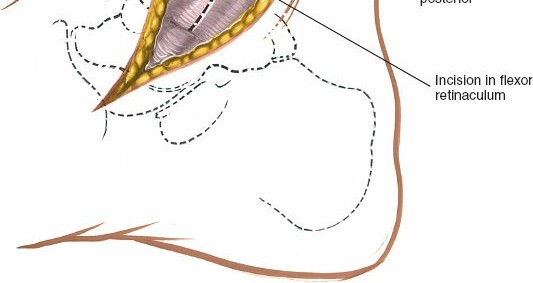
Alternatively, for more posterior access or in cases with a large posterior malleolar fragment, the interval can be created between the tibialis posterior and the flexor digitorum longus, or even posterior to the flexor hallucis longus if direct posterior malleolar access is paramount. Meticulous identification and protection of the posterior tibial neurovascular bundle (artery, nerve, FDL, FHL) located posterior to the tibialis posterior tendon are critical. These structures are typically retracted posteriorly or anteriorly as a bundle, depending on the desired exposure.

-
Exposure:
- The posterior aspect of the medial malleolus and the distal tibia are exposed.
-
This approach offers direct visualization of vertical medial malleolar fractures and can also provide access to associated posterior malleolar fragments without a separate incision.

-
Reduction:
- Clear the fracture site of any interposed soft tissues.
- Use reduction clamps, pointed reduction forceps, or bone hooks to achieve anatomical reduction of the medial malleolar fragment.
- For vertical fractures, direct compression and manipulation may be required.
-
Confirm reduction visually and with fluoroscopy in multiple planes.

-
Fixation:
-
Lag Screws:
Two 3.5 mm or 4.0 mm partially threaded cancellous screws can be placed from posterior to anterior, perpendicular to the fracture line, to achieve interfragmentary compression. Care must be taken to avoid violating the ankle joint surface and to ensure proper screw length.
 - Posteromedial Plate: For vertical shear fractures or significantly comminuted fragments, a small contourable plate (e.g., 1/3 tubular, specialized medial plate) can be applied to the posteromedial aspect of the malleolus and distal tibia, acting as a buttress. Screws are carefully placed to avoid injury to adjacent neurovascular structures and tendons.
-
Confirm final fixation and joint congruity with fluoroscopy.

-
Lag Screws:
Two 3.5 mm or 4.0 mm partially threaded cancellous screws can be placed from posterior to anterior, perpendicular to the fracture line, to achieve interfragmentary compression. Care must be taken to avoid violating the ankle joint surface and to ensure proper screw length.
Wound Closure (Both Approaches)
- Thorough irrigation of the surgical field.
- Check for hemostasis.
- Reapproximate the periosteum if possible.
- Close the subcutaneous tissue layer using absorbable sutures.
-
Close the skin with non-absorbable sutures or staples.
 -
Apply a sterile dressing and soft padded splint or a controlled ankle motion (CAM) walker boot.
Complications & Management
Despite meticulous surgical technique, complications can arise following ORIF of medial malleolar fractures. Awareness and timely management are crucial for optimal patient outcomes.
Common Complications
- Surgical Site Infection: Ranges from superficial cellulitis to deep osteomyelitis.
- Wound Dehiscence: Breakdown of the incision, particularly problematic in areas of compromised soft tissue or high tension.
- Saphenous Nerve Injury: Sensory neuropathy (numbness, dysesthesia) along the medial aspect of the ankle and foot due to traction, compression, or direct transection.
- Hardware Irritation/Prominence: Screws or plates can be palpable or irritate adjacent tendons, skin, or the saphenous nerve.
- Nonunion/Malunion: Failure of the fracture to heal or healing in an unacceptable anatomical position. Nonunion is more common with vertical fracture patterns or inadequate fixation.
- Post-Traumatic Arthritis: Long-term complication, even after anatomical reduction, due to initial cartilage damage or subtle residual incongruity.
- Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE): Thromboembolic events, though relatively low with appropriate prophylaxis.
- Complex Regional Pain Syndrome (CRPS): A rare but debilitating neuropathic pain condition.
Table 2: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (Approx.) | Salvage / Management Strategy |
|---|---|---|
| Surgical Site Infection | 1-5% | Superficial: Oral antibiotics, local wound care. Deep: Surgical debridement, IV antibiotics, irrigation, culture-directed therapy. Implant retention considered if stable and no gross pus; otherwise, implant removal, external fixation, and delayed reimplantation/reconstruction. |
| Wound Dehiscence | 2-10% | Minor: Local wound care, serial debridement, secondary intention healing. Major: Delayed primary closure, skin grafting, local flap coverage, or negative pressure wound therapy (NPWT). |
| Saphenous Nerve Injury | 5-15% (sensory deficit) | Neuropraxia/Axonotmesis: Observation, desensitization exercises, gabapentin/pregabalin for neuropathic pain. Severed nerve/Neuroma: Surgical neurolysis or excision of symptomatic neuroma; potential nerve graft in rare cases for extensive defects. |
| Hardware Irritation/Prominence | 10-30% | If symptomatic and fracture has united, hardware removal (typically 6-12 months post-op). |
| Nonunion/Malunion | 1-5% | Nonunion: Revision ORIF with bone grafting (autograft or allograft), plate fixation. Symptomatic Malunion: Corrective osteotomy and re-fixation. In severe, recalcitrant cases, ankle arthrodesis may be considered. |
| Post-Traumatic Arthritis | 10-20% (long-term) | Early: Conservative management (NSAIDs, PT, activity modification), intra-articular injections (corticosteroids, hyaluronic acid). Advanced: Arthroscopic debridement, osteotomies for realignment, distraction arthroplasty, or ultimately ankle arthrodesis or total ankle arthroplasty for end-stage disease. |
| Deep Vein Thrombosis (DVT)/PE | <1% (with prophylaxis) | Therapeutic anticoagulation. Consider inferior vena cava (IVC) filter if anticoagulation is contraindicated or recurrent PE. |
| Complex Regional Pain Syndrome (CRPS) | <1-5% | Multidisciplinary approach: pharmacotherapy (neuropathic agents, regional blocks), physical therapy, occupational therapy, psychological support. Referral to a pain specialist is essential. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is critical for achieving optimal functional recovery and minimizing stiffness. Protocols are individualized based on fracture stability, fixation achieved, and surgeon preference. The following outlines a general progressive rehabilitation protocol.
Phase 1: Immediate Post-Operative (Weeks 0-2)
- Goals: Protect surgical repair, minimize swelling and pain, maintain extremity circulation.
- Weight Bearing: Non-weight bearing (NWB) on the affected limb.
- Immobilization: Short-leg posterior splint or removable controlled ankle motion (CAM) walker boot, typically in a neutral position.
-
Management:
- Strict elevation above the heart.
- Cryotherapy (ice) regularly.
- Pain medication as prescribed.
- Maintain range of motion (ROM) of knee and hip.
- Toe wiggles to promote circulation.
- Instruct on signs of complications (infection, DVT, nerve irritation).
Phase 2: Early Mobilization & Protected Weight Bearing (Weeks 2-6)
- Goals: Gradually restore ankle ROM, initiate protected weight-bearing, reduce swelling.
- Weight Bearing: Progression to protected weight bearing (PWB) in a CAM boot or cast, typically 25% weight-bearing at 2-3 weeks, advancing to 50% by 4-6 weeks, as tolerated and based on radiographic signs of healing.
- Immobilization: Continue CAM boot.
-
Exercises (as tolerated and surgeon-approved):
- Gentle active and passive ankle dorsiflexion/plantarflexion within pain-free limits, out of the boot.
- Ankle circumduction.
- Soft tissue massage to scar.
- Stationary bike with light resistance (seated, NWB initially, progressing to PWB).
Phase 3: Strengthening & Proprioception (Weeks 6-12)
- Goals: Restore full ankle ROM, improve strength, enhance proprioception and balance.
- Weight Bearing: Progress to full weight-bearing (FWB) out of the boot, as tolerated, provided radiographs show adequate healing.
-
Exercises:
- Continue full ankle ROM exercises.
- Theraband exercises for all ankle movements (dorsiflexion, plantarflexion, inversion, eversion).
- Calf raises (bilateral to unilateral).
- Balance and proprioceptive training: single-leg stance, wobble board, uneven surfaces.
- Gait training to normalize walking pattern.
- Initiate light impact activities as appropriate.
Phase 4: Return to Activity & Sport-Specific Training (Weeks 12+)
- Goals: Return to pre-injury activity levels, optimize dynamic stability and power.
- Weight Bearing: Full weight bearing without restrictions.
-
Exercises:
- Advanced strengthening exercises (e.g., plyometrics, resistance training).
- Agility drills, sport-specific exercises (running, jumping, cutting).
- Continue proprioceptive training.
- Gradual return to high-impact activities and sports, typically after 3-6 months, depending on healing and functional recovery.
- Considerations: Patients should be counseled on the potential for persistent swelling, stiffness, or discomfort for up to 12 months post-operatively. Hardware removal may be considered for symptomatic patients after full fracture union, usually after 6-12 months.
Summary of Key Literature / Guidelines
The management of medial malleolar fractures is guided by a substantial body of orthopedic literature and consensus guidelines. Key principles emphasize anatomical reduction, stable fixation, and early mobilization to achieve optimal long-term outcomes and mitigate the risk of post-traumatic arthrosis.
Fracture classification systems, such as the Lauge-Hansen and Danis-Weber classifications, provide a framework for understanding injury mechanisms and often dictate the need for medial malleolar fixation in the context of broader ankle injuries. Current evidence strongly supports operative intervention for displaced medial malleolar fractures (>2mm displacement or articular step-off) or those causing ankle instability. Non-operative management is reserved for truly non-displaced and stable fractures.
Studies comparing various fixation methods (lag screws, tension band, plates) suggest that while lag screws are the workhorse for most transverse and oblique fractures, tension band wiring is a viable option for small avulsion fragments, and buttress plating is increasingly favored for vertical shear or comminuted patterns to provide enhanced stability and prevent subsidence. The choice of anterior versus posterior (posteromedial) approach is guided by fracture morphology, particularly the presence of posterior extension or a concomitant posterior malleolar fragment. The posterior approach is gaining favor for certain complex fracture patterns due to direct visualization of the posteromedial aspect of the tibia and malleolus.
Long-term studies have highlighted the importance of achieving and maintaining an anatomical reduction, as even minor residual displacement or articular incongruity can predispose to post-traumatic osteoarthritis. Complication rates, while manageable, necessitate thorough pre-operative planning and meticulous surgical technique. Wound complications and hardware irritation remain common, often necessitating hardware removal. Neurovascular injuries, particularly to the saphenous nerve, are also recognized risks.
Rehabilitation protocols, universally, prioritize immediate post-operative protection, followed by a phased progression of range of motion, protected weight bearing, strengthening, and proprioceptive training. The goal is to safely restore function and facilitate a timely return to activity. Adherence to these principles, informed by robust clinical evidence, forms the cornerstone of contemporary medial malleolar fracture management.
Clinical & Radiographic Imaging

You Might Also Like


