Ankle Fractures: Comprehensive Guide to Epidemiology, Classification, Anatomy & Biomechanics

Key Takeaway
Ankle fractures are classified by systems like Danis-Weber (fibular fracture level), Lauge-Hansen (injury mechanism), and AO/OTA (fracture morphology). These categorize common patterns such as isolated malleolar, bimalleolar, and trimalleolar fractures. Understanding epidemiology, surgical anatomy, and biomechanics is vital for accurate diagnosis and optimal management.
Introduction & Epidemiology
Ankle fractures represent a spectrum of injuries involving the osseous components of the tibiotalar joint. The ankle is a critical articulation comprising the distal tibia (forming the medial malleolus and tibial plafond), the distal fibula (forming the lateral malleolus), and the talus. Stability is maintained by a robust ligamentous complex, including the syndesmotic ligaments and the collateral ligaments. Disruption of these structures, often concomitant with an osseous injury, dictates stability and treatment.
The epidemiology of ankle fractures demonstrates a bimodal distribution. Younger, active individuals often sustain these injuries during sports or high-energy trauma, characterized by twisting mechanisms. A second peak occurs in the elderly population, frequently due to low-energy falls, often compounded by osteopenia or osteoporosis. The global incidence is significant, estimated at 100-200 per 100,000 person-years, with substantial socioeconomic implications due to treatment costs and potential long-term morbidity.
Classification systems are fundamental for diagnosis, prognosis, and treatment planning. The Danis-Weber classification, based on the level of the fibular fracture relative to the syndesmosis, broadly categorizes fractures as:
*
Weber A:
Infrasyndesmotic fibular fracture, typically stable.
*
Weber B:
Transsyndesmotic fibular fracture, with variable syndesmotic integrity.
*
Weber C:
Suprasyndesmotic fibular fracture, inherently unstable due to syndesmotic disruption.
The Lauge-Hansen classification, based on the mechanism of injury and the position of the foot at the time of injury, provides a more detailed, albeit more complex, framework for understanding injury progression. While clinically useful for interpreting plain radiographs, it is less frequently used for direct surgical planning than the simpler Danis-Weber or the comprehensive AO/OTA classification. The AO/OTA system provides a alphanumeric code reflecting the bone involved, the segment, and the fracture morphology (e.g., A, B, C for simple, wedge, complex).
Common fracture patterns include:
*
Isolated Lateral Malleolus Fractures:
These are breaks in the distal fibula. The stability of the ankle joint largely depends on the integrity of the deltoid ligament and the syndesmosis.

*
Isolated Medial Malleolus Fractures:
These involve the distal tibia. They are often associated with lateral ligamentous injury or syndesmotic disruption.

*
Bimalleolar Fractures:
Characterized by fractures of both the lateral and medial malleoli. These are inherently unstable injuries, often requiring operative intervention.

*
Trimalleolar Fractures:
Involve fractures of the lateral malleolus, medial malleolus, and the posterior malleolus (posterior aspect of the tibial plafond). These injuries represent a high degree of instability and often have worse prognoses due to articular involvement.
The etiology of ankle fractures primarily stems from trauma. These can range from low-energy twisting mechanisms, such as inversion or eversion injuries, to high-energy axial loading or direct impact. Underlying conditions such as osteoporosis, metabolic bone diseases, or neurological disorders (e.g., Charcot arthropathy) can predispose individuals to fragility fractures. Participation in high-impact or pivoting sports significantly elevates the risk.
Surgical Anatomy & Biomechanics
A thorough understanding of the ankle's surgical anatomy and biomechanics is paramount for successful fracture management. The ankle joint is a highly congruent hinge joint, primarily allowing dorsiflexion and plantarflexion, with limited inversion and eversion provided by the subtalar joint.
Osseous Anatomy
- Tibia: The distal tibia forms the tibial plafond superiorly and the medial malleolus medially. The tibial plafond articulates with the talar dome, providing the primary weight-bearing surface. The medial malleolus extends distally, forming a buttress against talar eversion and providing attachment for the deltoid ligament. Posteriorly, the posterior malleolus forms part of the ankle mortise and can be involved in fractures, particularly trimalleolar patterns.
- Fibula: The distal fibula forms the lateral malleolus, which extends more distally and posteriorly than the medial malleolus. It articulates with the lateral aspect of the talus and is a crucial component of the ankle mortise, preventing talar displacement. The lateral malleolus serves as the attachment site for the lateral collateral ligaments (anterior talofibular, posterior talofibular, calcaneofibular).
- Talus: The talus is unique in that it has no muscular attachments. Its superior surface (talar dome) is cartilaginous and articulates with the tibial plafond. The lateral and medial facets articulate with the malleoli, forming the mortise. The shape of the talus, wider anteriorly, contributes to the inherent stability of the ankle in dorsiflexion.
Ligamentous Anatomy
The stability of the ankle joint relies heavily on its robust ligamentous structures:
-
Syndesmotic Ligaments: These fibrous connections bind the distal tibia and fibula, maintaining the integrity of the ankle mortise. Key components include:
- Anterior Inferior Tibiofibular Ligament (AITFL): Connects the anterior tubercle of the tibia to the anterior aspect of the lateral malleolus.
- Posterior Inferior Tibiofibular Ligament (PITFL): Connects the posterior tubercle of the tibia to the posterior aspect of the lateral malleolus.
- Interosseous Ligament: A strong fibrous continuation of the interosseous membrane, located superior to the AITFL and PITFL, providing significant stability.
- Transverse Ligament: The deepest and most inferior fascicle of the PITFL.
Disruption of the syndesmosis, often indicated by an increased medial clear space on plain radiographs, leads to widening of the ankle mortise and instability.
2. Medial Collateral Ligament (Deltoid Ligament): A strong, triangular ligament with superficial and deep components.
* Superficial Layer: Attaches from the medial malleolus to the navicular, spring ligament, and calcaneus.
* Deep Layer: Attaches from the medial malleolus to the body of the talus. This layer is crucial for tibiotalar stability.
The deltoid ligament resists eversion and external rotation forces.
3. Lateral Collateral Ligaments: Composed of three distinct bands:
* Anterior Talofibular Ligament (ATFL): Weakest of the three, connecting the fibula to the talus, resists inversion and internal rotation.
* Calcaneofibular Ligament (CFL): Connects the fibula to the calcaneus, resists inversion.
* Posterior Talofibular Ligament (PTFL): Strongest, connecting the fibula to the talus, resists extreme dorsiflexion and internal rotation.
These ligaments resist inversion forces and internal rotation.
Biomechanics of Ankle Stability
The ankle mortise functions as a tight, congruent articulation. Normal weight-bearing stresses are distributed evenly across the talar dome. Any disruption, such as a displaced fracture or ligamentous injury, can lead to altered contact pressures and kinematics.
*
Mortise Integrity:
The key to ankle stability is the maintenance of the talus within the mortise. A 1mm lateral shift of the talus can reduce the tibiotalar contact area by up to 42%, significantly increasing joint contact pressures and predisposing to post-traumatic arthritis.
*
Syndesmosis Role:
The syndesmosis acts as a spring, allowing physiological widening and narrowing of the distal tibiofibular joint during ankle motion, particularly dorsiflexion. Its integrity is crucial for resisting external rotation and controlling fibular position.
*
Malleolar Buttressing:
The malleoli act as bony buttresses preventing talar subluxation. Loss of these buttresses, especially the lateral malleolus, compromises stability.
Indications & Contraindications
The decision-making process for operative versus non-operative management of ankle fractures is complex and multifactorial, considering fracture morphology, stability, patient comorbidities, and soft tissue status. The primary goal of operative fixation is to restore anatomical alignment, achieve rigid fixation, and facilitate early functional rehabilitation to prevent post-traumatic arthritis and long-term disability.
Indications for Operative Management
Operative fixation is generally indicated for unstable ankle fractures. Instability can be defined by:
1.
Fracture Displacement:
Any significant displacement (>2mm) of articular surfaces or malleolar fragments.
2.
Mortise Instability:
Widening of the medial clear space (>4mm on stress views, or >2mm compared to contralateral), talar shift, or syndesmotic disruption.
3.
Specific Fracture Patterns:
* Bimalleolar and trimalleolar fractures.
* Displaced medial malleolus fractures.
* Displaced lateral malleolus fractures (Weber B or C) with evidence of deltoid injury (medial clear space widening) or syndesmotic instability.
* Displaced posterior malleolus fractures involving >25-30% of the articular surface or causing talar subluxation.
* Open fractures (requiring urgent debridement and stabilization).
* Fracture-dislocations.
* Pilon fractures (distal tibial plafond fractures) with articular incongruity.
* Ankle fractures in polytrauma patients where early mobilization is desired.
* Fractures in patients with neuropathic conditions (e.g., Charcot arthropathy) where rigid fixation is critical.
Contraindications for Operative Management
Absolute contraindications for operative fixation are rare and typically relate to the patient's physiological status. Relative contraindications necessitate careful risk-benefit analysis:
- Severe Comorbidities: Uncontrolled diabetes, severe peripheral vascular disease, end-stage renal disease, or other systemic conditions that significantly increase surgical risk (e.g., high ASA score).
- Poor Soft Tissue Envelope: Severe blistering, significant skin avulsion, or extensive swelling precluding safe surgical incision and wound closure. In such cases, a staged approach (e.g., temporary external fixation followed by definitive ORIF once soft tissues improve) may be considered.
- Active Infection: Cellulitis or osteomyelitis in the surgical field.
- Non-displaced, Stable Fractures: Stable, isolated lateral malleolus (Weber A, or some Weber B without deltoid/syndesmotic injury) or isolated medial malleolus fractures that remain anatomically reduced and stable.
- Non-ambulatory Patients: For patients with extremely limited functional demands or non-ambulatory status, non-operative management might be preferred if fracture stability allows.
- Extremely Advanced Age/Frailty: In select cases, the risks of surgery may outweigh the potential benefits for frail elderly patients with low functional expectations, assuming the fracture can be managed non-operatively without severe pain or skin breakdown.
Operative vs. Non-Operative Indications: Summary
| Feature | Operative Indications | Non-Operative Indications |
|---|---|---|
| Fracture Type | Bimalleolar, Trimalleolar, Displaced Malleolar (Medial, Lateral), Displaced Posterior Malleolus (>25-30% articular surface), Open fractures, Fracture-dislocations, Pilon fractures. | Isolated, non-displaced lateral malleolus fractures (Weber A, or stable Weber B without medial clear space widening), Isolated, non-displaced medial malleolus fractures, Isolated, non-displaced posterior malleolus fractures (<25% articular surface), Stress fractures. |
| Stability | Unstable ankle mortise (talar shift >1-2mm, medial clear space widening >4mm, positive stress tests for syndesmotic or deltoid instability). | Stable ankle mortise (no talar shift, normal medial clear space, stable with stress). |
| Displacement | Articular incongruity >1-2mm. Cortical displacement >2mm. | Anatomically reduced or minimally displaced fractures (<1-2mm). |
| Soft Tissue Status | Generally good soft tissue envelope or controllable swelling (if amenable to delayed fixation after swelling subsides). | Severe blistering, significant skin loss, active cellulitis precluding immediate surgery (may consider temporary external fixation with delayed ORIF). Uncontrolled edema. |
| Patient Factors | Young, active individuals, patients with high functional demands, patients requiring early mobilization (e.g., polytrauma). | Severe medical comorbidities (e.g., uncontrolled diabetes, severe PVD, advanced cardiac/pulmonary disease) where surgical risks outweigh benefits. Frail, non-ambulatory patients with limited functional demands. Patients refusing surgery after informed discussion. |
| Concomitant Injuries | Ligamentous instability (syndesmosis, deltoid), compartment syndrome. | No significant concomitant ligamentous instability requiring repair. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is critical for optimizing outcomes and minimizing complications.
Diagnostic Imaging
- Standard Radiographs: Anteroposterior (AP), Lateral, and Mortise views are essential. The mortise view (AP with 15-20 degrees internal rotation) best evaluates the tibiotalar joint space, medial clear space, and syndesmosis. Stress radiographs (gravity stress, external rotation stress) may be necessary to assess syndesmotic and deltoid ligament integrity in equivocal cases.
- Computed Tomography (CT): Increasingly utilized, especially for complex fractures (trimalleolar, pilon, comminuted), assessing posterior malleolus size and displacement, identifying articular impaction, and guiding hardware placement. CT with 3D reconstructions can be invaluable for understanding fracture morphology and planning reduction strategies.
- Magnetic Resonance Imaging (MRI): Less common in acute trauma, but can be useful for assessing soft tissue injuries (e.g., deltoid ligament avulsion, osteochondral lesions, syndesmotic sprain without frank rupture) if clinically indicated and not fully appreciated on other imaging.
Pre-Operative Assessment & Optimization
- Medical Optimization: Comprehensive medical evaluation to assess patient comorbidities (diabetes, cardiovascular disease, pulmonary compromise, nutritional status) and optimize their condition for surgery. Glycemic control in diabetics, cessation of anticoagulants (with bridging if necessary), and smoking cessation counseling are paramount.
- Neurovascular Status: Thorough assessment of neurovascular status distal to the injury, documented pre- and post-reduction.
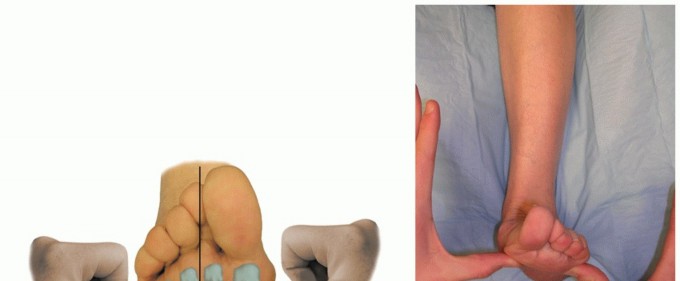
- Soft Tissue Assessment: Critical evaluation of skin integrity, presence of blisters, swelling, and open wounds. Delaying surgery for several days to allow swelling to subside and skin wrinkles to reappear (the "wrinkle sign") is often prudent to minimize wound complications. External fixation may be used as a temporizing measure for severe swelling or open fractures.
- Antibiotic Prophylaxis: Administer pre-operative intravenous antibiotics, typically a first or second-generation cephalosporin, 30-60 minutes before incision. For open fractures, broader spectrum antibiotics are indicated.
- Fluoroscopy Availability: Confirm the availability and functionality of a C-arm in the operating room.
Patient Positioning
The most common positioning for ankle fracture open reduction and internal fixation (ORIF) is
supine
on a radiolucent operating table.
* A bump or blanket roll under the ipsilateral hip can internally rotate the leg, facilitating access to the lateral malleolus.
* The entire leg, from mid-thigh to toes, should be prepped and draped to allow manipulation of the ankle and foot for reduction and assessment of motion.
* The C-arm can be positioned to obtain AP, lateral, and mortise views without repositioning the patient.
* For posterior malleolus fractures requiring a direct posterior approach, a
prone
or
lateral decubitus
position may be considered, but this often necessitates repositioning the patient if other malleoli also require fixation, which can be cumbersome. Often, a supine approach with an extended posterolateral incision and careful retraction is preferred to address posterior malleolar fractures without repositioning.
Detailed Surgical Approach / Technique
The surgical approach to ankle fractures is determined by the specific fracture pattern, the location of the fragments, and the need for access to various malleoli and the syndesmosis. The general principles include anatomical reduction, stable internal fixation, and restoration of ankle mortise congruity.
1. Lateral Malleolus Fracture Fixation
Typically, the lateral malleolus is addressed first in multi-malleolar fractures as its anatomical reduction helps restore fibular length and rotational alignment, which is critical for guiding the reduction of other fragments and the talus.
Approach
- Incision: A curvilinear or straight incision centered over the distal fibula, extending from approximately 5 cm proximal to the tip of the lateral malleolus to the level of the calcaneocuboid joint distally.
- Dissection: Dissect through the subcutaneous tissue. Identify and protect the superficial peroneal nerve branches, particularly those that cross the incision, and the lesser saphenous vein, if encountered. The deep fascia is incised longitudinally, revealing the peroneus brevis and longus tendons posteriorly and the fibula anteriorly.
- Internervous Plane: The approach to the lateral malleolus is generally extensile, utilizing the interval between the peroneus longus/brevis posteriorly and the anterior compartment muscles anteriorly.
Reduction and Fixation
- Exposure: Subperiosteal dissection exposes the fracture fragments. Hematoma evacuation is performed.
- Reduction: Restore fibular length and rotation. This often requires axial traction and gentle manipulation. For oblique or spiral fractures, reduction clamps (e.g., pointed reduction clamp, Verbrugge clamp) are applied across the fracture site.
-
Fixation:
- Lag Screws: For long oblique or spiral fractures, one or two lag screws can be inserted across the fracture plane to achieve interfragmentary compression.
- Plate Fixation: A contoured one-third tubular plate, a locking compression plate (LCP), or a pre-contoured ankle fracture plate is applied to the lateral surface of the fibula. The plate should span the fracture, with at least two or three screws proximal and distal to the fracture site. Screws can be bicortical or unicortical, locking or non-locking, depending on bone quality and desired stability. A "neutralization plate" technique involves using a plate to buttress and neutralize rotational and bending forces after lag screw compression. An "anti-glide plate" is placed posteriorly to resist posterior displacement of the distal fragment, particularly for oblique fractures extending from anteroproximal to posterodistal.
2. Medial Malleolus Fracture Fixation
Medial malleolus fractures are typically approached anteromedially.
Approach
- Incision: A curvilinear incision over the medial malleolus, parallel to the posterior tibial tendon, extending from 2-3 cm proximal to the tip of the malleolus to the sustentaculum tali.
- Dissection: Careful dissection through the subcutaneous tissue. Identify and protect the saphenous vein and nerve, which course anterior to the medial malleolus. Incise the retinaculum or periosteum.
- Internervous Plane: The approach is direct, through subcutaneous tissue and then splitting the superficial and deep deltoid ligaments for intra-articular fractures.
Reduction and Fixation
- Exposure: Subperiosteal dissection and hematoma evacuation.
- Reduction: Direct reduction of the fragment. A pointed reduction clamp may be used. Ensure restoration of the articular surface.
-
Fixation:
- Lag Screws: The most common method. One or two 3.5mm or 4.0mm cannulated or non-cannulated screws are inserted from the tip of the medial malleolus, obliquely across the fracture line, into the tibial shaft. Ensuring proper screw length and trajectory to engage sufficient cortex is critical.
- Tension Band Wiring: For small, avulsed fragments, particularly in osteoporotic bone. Two K-wires are placed across the fracture, and a figure-of-eight wire loop is passed around the K-wires and a screw in the distal tibia, compressing the fragment.
- Anti-glide Plate: For vertical medial malleolus fractures (e.g., supination-adduction type II), an anti-glide plate can be effective in resisting shear forces.
3. Posterior Malleolus Fracture Fixation
Fixation of the posterior malleolus is indicated if the fragment is significantly displaced (>2mm), involves >25-30% of the articular surface, causes talar subluxation, or creates significant posterior instability of the talus.
Approach
- Posterolateral Approach: This is the most common for larger posterior malleolus fragments. An incision is made between the Achilles tendon and the peroneal tendons. Dissection involves identifying and retracting the sural nerve and lesser saphenous vein. The interval between the flexor hallucis longus (FHL) and the peroneal tendons is developed. The posterior aspect of the fibula and tibia are exposed.
- Posteromedial Approach: Less common, but can be used for smaller, medially displaced fragments. The interval between the tibialis posterior and FHL tendons is utilized.
- Anterolateral Approach (Indirect): Small posterior malleolus fractures may sometimes be reduced and fixed with anterior-to-posterior screws after lateral malleolus fixation, but this is less common and relies on indirect reduction.
Reduction and Fixation
- Exposure: Careful retraction of neurovascular structures (tibial nerve, posterior tibial artery/vein).
- Reduction: Direct reduction under fluoroscopic guidance. Reduction clamps or K-wires can aid in temporary stabilization.
-
Fixation:
- Anterior-to-posterior Screws: If the fragment is large enough and amenable, screws are placed from anterior-to-posterior through the anterior tibial cortex into the posterior malleolus. This requires precise trajectory.
- Posterior Plate Fixation: A small fragment plate (e.g., one-third tubular plate, specialty posterior malleolus plate) can be applied to the posterior aspect of the tibia, typically with screws extending into the main tibial shaft. This is often preferred for larger, comminuted, or unstable posterior fragments.
- Posteroanterior Lag Screws: Screws inserted from the posterior aspect of the fragment into the tibial metaphysis.
4. Syndesmotic Fixation
Syndesmotic instability must be assessed intraoperatively after fixation of the malleoli.
*
Assessment:
*
Hook Test:
A hook placed under the fibula is used to apply lateral traction. Excessive movement suggests instability.
*
External Rotation Stress Test:
With the lateral malleolus reduced and fixed, an external rotation stress is applied to the foot. C-arm views are obtained to check for medial clear space widening.
*
Cotton Test:
A blunt instrument used to pry the fibula laterally.
*
Fixation:
If unstable, syndesmotic fixation is performed.
*
Screws:
Typically, one or two 3.5mm or 4.5mm cortical screws are placed 2-4 cm above the ankle joint line, traversing three (tricortical) or four (quadricortical) cortices. The screw should be placed parallel to the ankle joint and angled 20-30 degrees anteriorly from the true lateral plane. The ankle is positioned in neutral dorsiflexion or slight dorsiflexion (to prevent "syndesmotic overcompression" or malreduction in plantarflexion).
*
Suture Button Devices:
Newer devices (e.g., TightRope™) allow for dynamic stabilization of the syndesmosis, avoiding potential issues with screw breakage or the need for routine hardware removal. These devices use a suture loop between two buttons to maintain tibiofibular reduction.
Key Intraoperative Steps:
- Soft Tissue Handling: Meticulous soft tissue handling, avoiding excessive retraction, and ensuring adequate irrigation are crucial to prevent wound complications.
- Fluoroscopy: Frequent use of fluoroscopy (AP, lateral, mortise views) to confirm reduction, hardware placement, and ankle joint congruity.
- Final Assessment: After all fixation, reassess ankle stability, range of motion, and confirm anatomical alignment on fluoroscopy. Ensure adequate irrigation and hemostasis before closure.

Surgical Fixation Example: A typical construct for internal fixation of an ankle fracture, demonstrating plate and screw application.
Complications & Management
Despite meticulous surgical technique, complications can occur following ankle fracture ORIF. These can be categorized into acute and chronic.
Acute Complications
-
Wound Complications (Infection, Dehiscence):
- Incidence: Varies, 2-15% for superficial infections, 0.5-5% for deep infections. Higher in open fractures, diabetics, and those with poor soft tissue quality.
- Management: Superficial infections may respond to oral antibiotics and local wound care. Deep infections or dehiscence require surgical debridement, intravenous antibiotics, and potentially hardware removal (if fixation is stable) or reconstructive soft tissue procedures.
-
Neurovascular Injury:
- Incidence: Rare (<1%). Damage to superficial peroneal nerve, saphenous nerve/vein, or sural nerve during exposure. Tibial artery/nerve can be injured in high-energy trauma or during posterior approaches.
- Management: Careful surgical technique, meticulous dissection, and clear identification of anatomical structures are preventative. Acute arterial injury requires vascular surgical consultation for repair. Nerve injuries may be managed expectantly for neuropraxia, or with surgical exploration and repair for transection.
-
Compartment Syndrome:
- Incidence: Rare but limb-threatening, particularly in high-energy trauma.
- Management: Prompt diagnosis based on clinical signs (pain out of proportion, pallor, paresthesia, pulselessness, paralysis) and compartment pressure measurements. Requires urgent fasciotomy.
-
Hardware Prominence/Irritation:
- Incidence: Common (10-30%), especially with plates and screws near superficial tendons or subcutaneous bone.
- Management: Often managed with symptomatic treatment. If persistent or severe, elective hardware removal after fracture healing (typically 6-12 months post-op) may be indicated.
Chronic Complications
-
Nonunion/Malunion:
- Incidence: Nonunion is rare (<5% with adequate fixation), malunion is more common, particularly rotational or length malalignment of the fibula.
- Management: Nonunion may require revision surgery with bone grafting and more rigid fixation. Malunion, especially if symptomatic or leading to altered biomechanics, may require corrective osteotomy.
-
Post-Traumatic Arthritis (PTA):
- Incidence: The most significant long-term complication, occurring in 10-50% of patients, even with anatomical reduction. Risk factors include initial articular cartilage damage, poor reduction, and high-energy mechanism.
- Management: Initially managed conservatively (NSAIDs, activity modification, bracing, injections). If debilitating, surgical options include arthroscopic debridement, osteotomies, ankle arthrodesis, or total ankle arthroplasty.
-
Syndesmotic Malreduction/Heterotopic Ossification:
- Incidence: Malreduction occurs in 10-30% of cases fixed with screws, leading to altered ankle kinematics. Heterotopic ossification can cause stiffness.
- Management: Symptomatic malreduction may require revision syndesmotic fixation. Routine hardware removal of syndesmotic screws is controversial but often performed to prevent breakage and allow physiological motion. Suture button devices have a lower incidence of malreduction.
-
Complex Regional Pain Syndrome (CRPS):
- Incidence: Rare but debilitating (1-5%).
- Management: Early recognition and multidisciplinary approach involving pain management specialists, physical therapy, and medication (e.g., gabapentin, tricyclic antidepressants, regional nerve blocks).
-
Ankle Stiffness and Weakness:
- Incidence: Common, especially after prolonged immobilization or significant soft tissue injury.
- Management: Aggressive physical therapy, including range-of-motion exercises, strengthening, and proprioceptive training.
Complications & Management: Summary
| Complication | Incidence (Approx.) | Salvage Strategies / Management |
|---|---|---|
| Wound Infection (Superficial) | 2-15% | Oral antibiotics, local wound care, close monitoring. |
| Wound Infection (Deep) | 0.5-5% | Urgent surgical debridement, IV antibiotics, hardware retention vs. removal (if stable union), soft tissue coverage if needed. |
| Wound Dehiscence | 1-10% | Local wound care, delayed primary closure, skin grafting, flap reconstruction. |
| Neurovascular Injury | <1% | Meticulous dissection to prevent. For injury: observation (neuropraxia), surgical exploration/repair (transection), vascular repair. |
| Compartment Syndrome | Rare | Immediate fasciotomy. |
| Hardware Prominence/Irritation | 10-30% | Conservative management (padding, shoe modifications). Elective hardware removal after fracture union (typically 6-12 months). |
| Nonunion | <5% | Revision ORIF with bone grafting (autograft/allograft), more rigid fixation, biological adjuncts (e.g., BMP). |
| Malunion | Variable | Corrective osteotomy (if symptomatic and significant angular/rotational deformity) after fracture union. |
| Post-Traumatic Arthritis | 10-50% | Conservative (NSAIDs, injections, bracing). Surgical: arthroscopic debridement, osteotomy, ankle arthrodesis, total ankle arthroplasty (for end-stage disease). |
| Syndesmotic Malreduction | 10-30% | Revision syndesmotic fixation (if symptomatic). Routine removal of syndesmotic screws often performed to prevent breakage and improve motion. |
| Complex Regional Pain Syndrome | 1-5% | Multidisciplinary pain management, physical therapy, pharmacological agents (gabapentin, TCAs), regional nerve blocks. |
| Ankle Stiffness/Weakness | Common | Intensive physical therapy (ROM, strengthening, proprioception). Possible arthroscopic lysis of adhesions (if recalcitrant). |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for optimizing functional recovery, preventing stiffness, and minimizing long-term disability. Protocols vary based on fracture stability, extent of soft tissue injury, and specific fixation construct.
Phase 1: Immobilization and Early Protection (0-6 Weeks Post-Op)
- Goals: Protect surgical repair, minimize pain and swelling, maintain soft tissue integrity.
- Weight-Bearing: Strictly non-weight bearing (NWB) in a splint or controlled ankle motion (CAM) boot/cast. For stable fixation constructs and patient compliance, NWB with a posterior splint for 2 weeks, followed by a CAM boot or walking cast, is common.
- Elevation: Consistent elevation above heart level to reduce edema.
- Cryotherapy: Application of ice packs to control swelling and pain.
-
Range of Motion (ROM):
- Initial (0-2 weeks): Gentle active toe and foot pump exercises to promote circulation and prevent DVT. Hip and knee ROM.
- Later (2-6 weeks): Once wound healing permits, gentle active and passive ankle dorsiflexion/plantarflexion within the limits of pain, often initiated out of the boot/cast. Avoid inversion/eversion to protect repair.
- Wound Care: Meticulous wound care, dressing changes, and monitoring for signs of infection. Suture removal typically at 2-3 weeks.
Phase 2: Progressive Weight-Bearing and ROM (6-12 Weeks Post-Op)
- Goals: Restore full ankle ROM, gradually introduce weight-bearing, improve muscle strength.
- Weight-Bearing: Progression from NWB to partial weight-bearing (PWB) in a CAM boot or walking cast, typically commencing around 6 weeks post-op, assuming radiographic evidence of healing. PWB progresses to full weight-bearing (FWB) as tolerated, usually by 8-12 weeks, based on clinical and radiographic assessment. Crutches or a walker are used for support during this transition.
- Range of Motion: Aggressive but controlled ankle ROM exercises (dorsiflexion, plantarflexion, inversion, eversion). Manual therapy for joint mobilization may be initiated by a physical therapist.
-
Strengthening:
- Isometrics: Gentle isometric exercises for ankle musculature (dorsiflexors, plantarflexors, invertors, evertors) while in the boot/cast.
- Resistive Exercises: Once out of the boot/cast and FWB, initiate resistance band exercises, calf raises, and balance board exercises.
- Gait Training: Focus on restoring a normal gait pattern, initially with assistive devices, then progressing to unassisted ambulation.
Phase 3: Advanced Strengthening and Proprioception (12+ Weeks Post-Op)
- Goals: Regain full strength, endurance, proprioception, and prepare for return to activity.
- Weight-Bearing: Full weight-bearing without assistive devices.
- Strengthening: Progressive resistive exercises, eccentric exercises, plyometrics (if appropriate for patient's goals). Focus on all muscle groups surrounding the ankle and foot.
- Proprioception and Balance: Single-leg stance, wobble board, balance beam exercises. This is critical for preventing re-injury.
- Functional Training: Agility drills, sport-specific exercises (if applicable).
- Return to Activity: Gradual return to light activities (e.g., swimming, cycling) once adequate strength and ROM are achieved. Return to high-impact activities or sports is typically delayed until 4-6 months post-op, with full clearance based on functional testing and physician assessment.
Considerations
- Syndesmotic Repair: If syndesmotic screws were placed, some protocols recommend non-weight bearing for longer (e.g., 8-10 weeks) or delaying specific ROM to protect the repair. If a suture button device was used, earlier weight-bearing may be permitted. Removal of syndesmotic screws is often performed between 12-16 weeks post-op, or later if the device is a TightRope, which may not require removal.
- Osteoporosis: Patients with poor bone quality may require extended periods of NWB or PWB.
- Patient Compliance: Adherence to rehabilitation protocols is essential. Non-compliance can lead to stiffness, poor healing, or re-injury.
- Hardware Removal: Elective hardware removal may be considered for symptomatic hardware (e.g., pain, irritation, impingement) typically after 6-12 months, once fracture healing is complete.
Summary of Key Literature / Guidelines
The management of ankle fractures has evolved significantly, guided by both consensus and evidence-based medicine.
-
Importance of Anatomical Reduction: Numerous studies emphasize that anatomical reduction, particularly of the talus within the mortise, is the most crucial factor in preventing post-traumatic osteoarthritis and achieving good long-term outcomes. Even 1-2mm of talar shift or articular incongruity significantly increases joint contact pressures and predisposes to degenerative changes. This principle underpins the rationale for ORIF in unstable fractures.
- Reference: Ramsey and Hamilton (1976) classic cadaveric study demonstrating the severe impact of minimal talar displacement on tibiotalar contact area.
-
Syndesmotic Injury Management: The precise management of syndesmotic injuries remains an area of ongoing debate.
- Diagnostic Challenges: Intraoperative assessment for syndesmotic instability (stress tests, fluoroscopy) is paramount. The reliability of these tests can be variable.
- Fixation Options: Both tricortical and quadricortical syndesmotic screws have been used, with no clear superiority demonstrated in terms of outcomes, though quadricortical screws may offer slightly more rigidity. The number of screws (one vs. two) also lacks definitive consensus.
- Dynamic vs. Rigid Fixation: Suture button devices offer dynamic stabilization, potentially allowing for earlier weight-bearing and avoiding complications associated with rigid screw fixation (breakage, need for removal). Recent systematic reviews and randomized trials suggest comparable functional outcomes between suture button and screw fixation, with a lower rate of hardware removal for suture button devices.
- Syndesmotic Screw Removal: Routine removal of syndesmotic screws is common in practice, though its necessity is debated. Some studies suggest no functional benefit to routine removal, while others cite improved ankle motion and reduced pain. Suture button devices typically do not require removal unless symptomatic.
- References: Multiple meta-analyses and RCTs compare screw vs. suture button for syndesmotic fixation. The SYNSER trial is a prominent ongoing randomized controlled trial designed to provide robust evidence regarding syndesmotic fixation methods.
-
Posterior Malleolus Fractures:
- Size Threshold: The conventional threshold for operative fixation of posterior malleolus fractures is typically >25-30% of the articular surface involvement, or any fragment leading to talar subluxation. However, more recent literature emphasizes the importance of stability rather than simply fragment size. Even smaller fragments can contribute to instability.
- Approach and Fixation: Direct posterior approaches are increasingly favored for larger or displaced posterior malleolar fragments to achieve anatomical reduction and stable fixation, especially with improved surgical understanding of the posterior anatomy.
- References: Studies by Hertel et al. (2001) and others have refined the understanding of posterior malleolus fracture biomechanics and indications for fixation.
-
Osteoporotic Ankle Fractures: The increasing incidence in the elderly population with osteoporotic bone presents unique surgical challenges.
- Fixation Challenges: Poor bone quality makes traditional screw and plate fixation less reliable, increasing the risk of hardware pullout and nonunion.
- Strategies: Locking plates, augmented fixation (e.g., polymethylmethacrylate, calcium phosphate cement), and careful surgical technique are essential to enhance stability in osteoporotic bone. Non-operative management should be considered if surgical risks are prohibitive and stability can be maintained.
- References: Consensus guidelines and technical notes often address specific considerations for fragility fractures.
-
Timing of Surgery: The "wrinkle sign" and resolution of significant soft tissue swelling are critical for minimizing wound complications, especially in closed fractures. Delaying surgery for 7-14 days to allow soft tissue recovery is often beneficial. Open fractures, however, require urgent debridement and stabilization within 6-8 hours.
- References: Literature on soft tissue envelope management and timing of ORIF for closed fractures.
-
AAOS and AANA Guidelines: Professional organizations like the American Academy of Orthopaedic Surgeons (AAOS) and the American Orthopaedic Foot & Ankle Society (AOFAS) frequently publish clinical practice guidelines and position statements that summarize evidence-based recommendations for ankle fracture management, covering diagnostic imaging, surgical indications, and post-operative care. These are invaluable resources for practitioners.
Clinical & Radiographic Imaging


You Might Also Like