Surgical Treatment of Cubital Tunnel Syndrome

Introduction and Epidemiology
Cubital tunnel syndrome represents a pervasive compression neuropathy of the ulnar nerve occurring at or adjacent to the elbow joint. The nomenclature "cubital" is derived from the Latin cubitus, denoting the elbow. Epidemiologically, cubital tunnel syndrome is the second most common compression neuropathy of the upper extremity requiring surgical intervention, superseded only by carpal tunnel syndrome. It predominantly affects individuals in their fourth to sixth decades of life, demonstrating a higher prevalence in males. This demographic skew is hypothesized to be secondary to anatomical dimorphism, specifically differences in the carrying angle, a narrower retrocondylar groove, and decreased subcutaneous adiposity at the medial elbow in men compared to women.
The pathogenesis of ulnar nerve compression at the elbow is inherently multifactorial, involving a complex interplay of traction, friction, and direct mechanical compression. Chronic compression precipitates localized nerve ischemia, leading to the disruption of the blood-nerve barrier. This cascade induces intraneural edema and subsequent perineural and epineural fibrosis. Prolonged mechanical and ischemic insult ultimately results in focal demyelination, which slows conduction velocity, and in severe, protracted cases, irreversible Wallerian degeneration of the axonal architecture. Furthermore, the "double crush" hypothesis must be considered, wherein proximal compression (e.g., cervical radiculopathy at C8-T1) renders the distal nerve more susceptible to compression at the cubital tunnel.
Without operative intervention, approximately half of mild, early-stage cases may resolve with strict activity modification, avoidance of prolonged elbow flexion, and nocturnal extension splinting. However, robust longitudinal studies have failed to establish a favorable natural history for severe disease characterized by persistent sensory deficits, intrinsic muscle wasting, or profound electrodiagnostic abnormalities. As the neuropathy progresses, subjective complaints typically manifest as paresthesias in the small finger and the ulnar half of the ring finger. This is frequently accompanied by an insidious, aching, or burning pain radiating proximally from the medial epicondyle into the medial brachium or distally into the ulnar forearm. Exacerbation of symptoms during sleep or prolonged elbow flexion (e.g., talking on a telephone, driving) remains a hallmark clinical feature of the disease.
Surgical Anatomy and Biomechanics
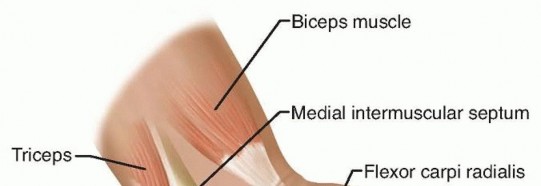
A profound comprehension of the regional anatomy and local biomechanics is paramount for safe, comprehensive, and effective surgical decompression. The ulnar nerve originates as the terminal continuation of the medial cord of the brachial plexus, carrying fibers predominantly from the C8 and T1 nerve roots. It courses distally through the anterior compartment of the arm, medial to the brachial artery, before piercing the medial intermuscular septum at the level of the arcade of Struthers to enter the posterior compartment.

Sites of Ulnar Nerve Compression
Surgical exploration must account for five primary anatomical zones where the ulnar nerve is distinctively susceptible to compression or tethering around the elbow:
- The Arcade of Struthers: A fascial band or thickening extending from the medial head of the triceps to the medial intermuscular septum, located approximately 8 to 10 cm proximal to the medial epicondyle. While its existence as a universally present, distinct anatomical structure is debated in the literature, fascial thickening in this region is a well-documented site of compression. It is particularly critical to release this area during anterior transposition of the ulnar nerve to prevent proximal kinking.
- The Medial Intermuscular Septum: As the nerve transitions from the anterior to the posterior compartment, it can be tethered by the rigid edge of the septum, particularly if the nerve is transposed anteriorly without concurrent septal excision.
- The Medial Epicondyle: The nerve passes through the retrocondylar groove, a fibro-osseous channel bordered anteriorly by the medial epicondyle, laterally by the olecranon, and floored by the medial collateral ligament (MCL).
- The Cubital Tunnel: The true cubital tunnel begins at the arcuate ligament of Osborne, a transverse fibrous band spanning from the medial epicondyle to the olecranon, connecting the two heads of the flexor carpi ulnaris (FCU). This ligament forms the primary roof of the tunnel, while the floor is formed by the posterior band of the MCL and the elbow joint capsule.
- The Deep Flexor Pronator Aponeurosis: Distally, the nerve passes between the humeral and ulnar heads of the FCU. The deep aponeurosis of the FCU can cause significant stenosis and must be released until the nerve is observed entering the normal, unconstricted muscle belly.
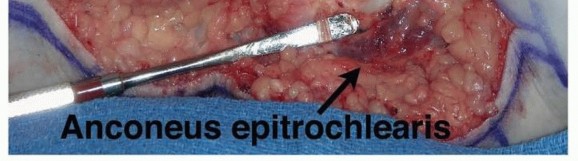
Anomalous structures may also contribute to dynamic or static compression. The anconeus epitrochlearis, an accessory muscle present in up to 11% to 30% of cadaveric specimens, extends from the medial olecranon to the medial epicondyle. When present, it replaces Osborne's ligament and acts as a dynamic compressor during elbow flexion, necessitating surgical excision.

Cutaneous Nerve Anatomy
The medial antebrachial cutaneous (MABC) nerve and the medial brachial cutaneous (MBC) nerve emanate directly from the medial cord of the brachial plexus. They are not branches of the ulnar nerve but are critical, high-risk structures within the surgical field. The MABC typically divides into anterior and posterior branches in the distal third of the arm. The posterior branch of the MABC reliably crosses the operative field transversally, approximately 2 to 3 cm distal to the medial epicondyle. Iatrogenic transection or traction injury to these branches can result in exquisitely painful neuromas, which frequently overshadow the functional benefits of the ulnar nerve decompression.

Biomechanical Considerations
Elbow kinematics play a critical role in the pathogenesis of cubital tunnel syndrome. The cubital tunnel is a dynamic space. During elbow flexion, the arcuate ligament of Osborne becomes taut, and the medial head of the triceps pushes medially. Consequently, the cubital tunnel volume decreases by up to 55%, while the intraneural pressure increases significantly, often exceeding capillary perfusion pressure. Furthermore, the ulnar nerve undergoes significant longitudinal excursion, stretching up to 4.7 mm or more to accommodate joint flexion.

In a subset of patients, the ulnar nerve lacks stable anatomical restraint within the retrocondylar groove due to a lax or absent Osborne's ligament or a hypoplastic medial epicondyle. This leads to subluxation or frank dislocation of the nerve over the apex of the medial epicondyle during flexion. This "perched" or subluxating nerve is subjected to severe friction, repetitive microtrauma, and sheer stress, accelerating the neuropathic process.

Indications and Contraindications
Surgical intervention is indicated when non-operative modalities (activity modification, NSAIDs, nocturnal splinting) fail to provide relief after 3 to 6 months, or when patients present initially with advanced disease. Comprehensive clinical evaluation should include a detailed motor and sensory examination. Advanced motor involvement is heralded by wasting of the first dorsal interosseous (FDI) and hypothenar muscles. Clinical signs of advanced motor weakness include a positive Froment sign (compensatory thumb interphalangeal joint flexion via the median-innervated flexor pollicis longus during key pinch), a positive Jeanne sign (compensatory thumb metacarpophalangeal joint hyperextension), and a positive Wartenberg sign (persistent abduction of the small finger due to unopposed action of the radial-innervated extensor digiti minimi combined with third palmar interosseous weakness).
Electrodiagnostic testing (EMG/NCS) is highly recommended to confirm the diagnosis, localize the precise site of compression, assess the severity of axonal loss, and rule out concurrent pathologies such as cervical radiculopathy (C8-T1), thoracic outlet syndrome, or polyneuropathy. A motor nerve conduction velocity of less than 50 m/s across the elbow segment, or a drop in amplitude of the compound muscle action potential (CMAP) of more than 20% across the elbow, is generally considered diagnostic. The presence of fibrillations or sharp waves on EMG indicates active denervation and mandates prompt surgical release.
| Clinical Scenario | Operative Management | Non Operative Management |
|---|---|---|
| Symptom Duration | > 3 to 6 months of persistent symptoms | < 3 months, intermittent symptoms |
| Sensory Findings | Constant numbness, two-point discrimination > 6mm | Intermittent paresthesias, normal two-point discrimination |
| Motor Findings | Intrinsic weakness, FDI atrophy, clawing | Normal grip and pinch strength, no atrophy |
| Electrodiagnostics | Conduction velocity < 50 m/s, denervation potentials | Normal or mildly delayed sensory latencies |
| Anatomy | Symptomatic subluxating nerve, space-occupying lesion | Stable nerve in retrocondylar groove |
Contraindications to surgical intervention include active local soft tissue or joint infection, severe medical comorbidities precluding anesthesia, and advanced, irreversible end-stage neuropathy where the primary goal of surgery (e.g., pain relief) does not align with patient expectations of motor recovery. In end-stage cases with complete intrinsic atrophy and no recordable CMAPs, surgery may halt progression and relieve pain but is unlikely to restore fine motor function.
Pre Operative Planning and Patient Positioning
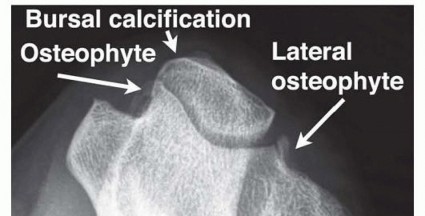
Preoperative planning requires a careful review of electrodiagnostic studies and any advanced imaging. While routine radiographs are sufficient to rule out gross bony deformities (e.g., cubitus valgus, osteoarthritis, heterotopic ossification), ultrasound or MRI is indicated if a space-occupying lesion (e.g., ganglion cyst, lipoma, anomalous muscle) is clinically suspected.
The patient is positioned supine on the operating table with the operative extremity extended on a radiolucent hand table. A non-sterile tourniquet is placed high on the brachium to ensure a bloodless field, though it should be deflated prior to closure to ensure meticulous hemostasis. The arm is externally rotated and abducted to expose the medial aspect of the elbow. Bony landmarks, including the medial epicondyle and olecranon, along with the anticipated course of the ulnar nerve, are carefully marked.

It is critical to mark the anticipated course of the MABC nerve branches. The posterior branch of the MABC typically crosses the operative field approximately 2 to 3 cm distal to the medial epicondyle. The incision should be planned slightly posterior to the medial epicondyle—rather than directly over it—to minimize the risk of intersecting these cutaneous branches perpendicularly and to prevent the surgical scar from resting directly over the bony prominence.
Detailed Surgical Approach and Technique
The optimal surgical management of cubital tunnel syndrome remains a topic of vigorous academic debate. Options include in situ decompression, anterior subcutaneous transposition, anterior intramuscular transposition, anterior submuscular transposition, and medial epicondylectomy. The choice of procedure relies heavily on preoperative nerve stability, primary versus revision surgical setting, patient anatomy (e.g., valgus deformity, obesity), and surgeon preference.

In Situ Ulnar Nerve Decompression
In situ decompression is the standard of care for primary cubital tunnel syndrome without baseline nerve subluxation or significant osseous deformity.
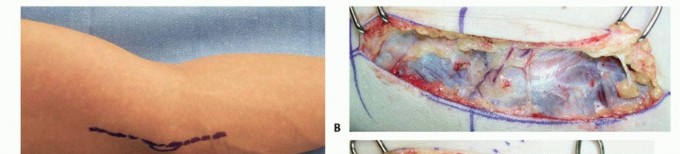
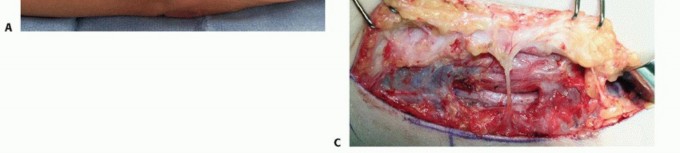
- Incision: An 8 to 10 cm longitudinal incision is made centered just posterior to the medial epicondyle.
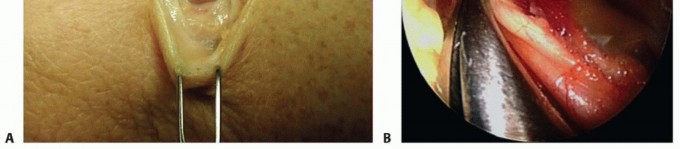
- Dissection: Subcutaneous tissues are carefully dissected using blunt and sharp techniques. Loupe magnification is highly recommended to identify and protect the branches of the MABC nerve.
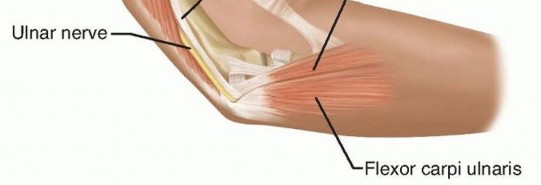
- Fascial Release: The fascia over the FCU is identified. The arcuate ligament of Osborne is incised sharply, releasing the primary roof of the cubital tunnel.
- Proximal and Distal Exploration: The decompression is carried proximally along the medial head of the triceps to the arcade of Struthers, ensuring complete release of the medial intermuscular septum. Distally, the nerve is followed between the two heads of the FCU, dividing the deep flexor-pronator aponeurosis until the nerve dives into the normal, unscarred muscle belly.
- Dynamic Assessment: The elbow is taken through a full, uninhibited range of motion to assess for iatrogenic nerve subluxation. If the nerve subluxates anterior to the medial epicondyle upon flexion, a transposition procedure must be performed to prevent postoperative friction neuritis.

Anterior Subcutaneous Transposition
This technique is indicated when the nerve subluxates dynamically, in cases of significant cubitus valgus deformity, or when osteophytes within the retrocondylar groove preclude a smooth gliding surface.
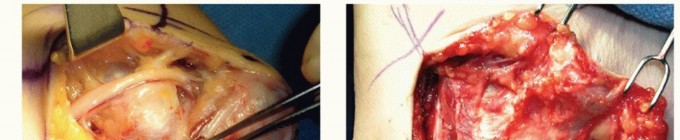
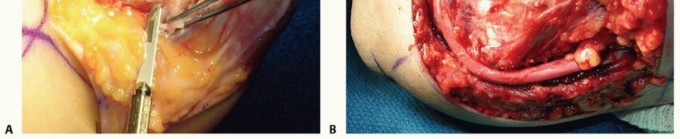
- Mobilization: Following a complete in situ release, the ulnar nerve is circumferentially mobilized from the arcade of Struthers down to its first motor branches to the FCU. Extreme care must be taken to preserve the extrinsic longitudinal blood supply (vasa nervorum) to the nerve, although some segmental vessels must inevitably be sacrificed to allow adequate mobilization.
- Septum Excision: The medial intermuscular septum must be aggressively excised to the level of the humerus to prevent proximal kinking of the nerve as it is transposed anteriorly.
- Transposition: The nerve is moved anterior to the medial epicondyle.
- Stabilization: A fasciodermal sling is created by suturing the subcutaneous tissue to the medial epicondyle or the residual fascia of the flexor-pronator mass. The surgeon must verify that the nerve is loosely retained in the anterior subcutaneous pocket without any points of compression, particularly at the proximal and distal fascial edges.
Anterior Submuscular Transposition
Submuscular transposition (often referred to as the Learmonth technique) places the nerve in a deep, well-vascularized bed. It is typically reserved for revision cases, severe primary cases with significant nerve scarring, or patients with minimal subcutaneous fat who would not tolerate a subcutaneous transposition.
- Preparation: The nerve is mobilized as described above. The medial intermuscular septum is excised completely.
- Flexor Pronator Mass Elevation: The flexor-pronator mass is sharply detached from the medial epicondyle, leaving a small fascial cuff for later repair. Alternatively, a step-cut Z-lengthening of the common flexor tendon can be performed. It is critical to identify and protect the median nerve, which lies deep to the pronator teres.
- Bed Preparation: The underlying brachialis muscle is exposed. The ulnar nerve is placed in a linear, tension-free bed adjacent to the median nerve.
- Reattachment: The flexor-pronator mass is repaired over the nerve using robust non-absorbable sutures. The surgeon must meticulously ensure that the fascial edges do not constrict the nerve at the proximal or distal exit points of the newly created submuscular tunnel.

Medial Epicondylectomy
Medial epicondylectomy achieves decompression by removing the bony prominence that causes tension and friction, allowing the nerve to naturally glide anteriorly during elbow flexion without the need for formal transposition and fascial sling creation.
- Exposure: The flexor-pronator origin is incised longitudinally over the medial epicondyle and reflected subperiosteally.
- Osteotomy: An osteotome or oscillating saw is used to resect the medial epicondyle. The trajectory of the osteotomy must be precise; removing less than 20% of the epicondyle width is insufficient for adequate decompression, while removing more than 50% critically risks destabilizing the anterior bundle of the medial collateral ligament (MCL), leading to valgus instability.
- Closure: The raw cancellous bone is smoothed with a rasp to prevent nerve abrasion, and bone wax may be applied to reduce postoperative hematoma. The flexor-pronator mass is securely repaired to the remaining periosteal sleeve.

Complications and Management
Surgical intervention for cubital tunnel syndrome is generally highly successful, yielding excellent outcomes in appropriately selected patients. However, complications can occur and are frequently related to technical errors during the procedure.

| Complication | Estimated Incidence | Etiology and Management Strategy |
|---|---|---|
| MABC Neuroma | 2% - 5% | Caused by transection or traction of MABC branches. Prevent via meticulous dissection. Salvage requires neuroma excision and proximal burying of the nerve end into deep muscle. |
| Incomplete Decompression | 1% - 3% | Failure to release the arcade of Struthers proximally or distal FCU fascia. Requires revision decompression and often submuscular transposition. |
| Iatrogenic Subluxation | 1% - 2% | Occurs after in situ decompression if the nerve becomes unstable. Managed by revision surgery with anterior transposition. |
| Elbow Instability | < 1% | Caused by over-resection during medial epicondylectomy (MCL |
Clinical & Radiographic Imaging

You Might Also Like


