Operative Management of Pelvic, Clavicular, Proximal Humeral, and Femoral Nonunions
Key Takeaway
The operative management of orthopaedic nonunions requires a profound understanding of fracture biomechanics, vascularity, and precise surgical techniques. This guide details evidence-based protocols for addressing complex nonunions of the pelvis, clavicle, and femoral neck. By employing rigid internal fixation, strategic bone grafting, and biomechanical realignment, orthopaedic surgeons can restore anatomical stability, alleviate pain, and optimize functional recovery in patients with delayed unions and recalcitrant nonunions.
Comprehensive Introduction and Patho-Epidemiology
The development of a nonunion represents a profound failure of the physiological bone-healing cascade, often precipitated by a confluence of mechanical instability, compromised vascularity, inadequate initial reduction, or profound biological host compromise. The United States Food and Drug Administration (FDA) formally defines a nonunion as a fracture that is a minimum of nine months post-occurrence and has shown no visible progressive signs of healing for three consecutive months. However, in the clinical arena of orthopedic traumatology, waiting nine months to intervene on a clearly failing osteosynthesis construct in critical anatomical regions is often deleterious to the patient's ultimate functional outcome. The operative management of these complex scenarios demands a rigorous, evidence-based approach tailored to the specific anatomical region, adhering strictly to the "Diamond Concept" of fracture healing championed by Giannoudis et al., which necessitates the optimization of osteogenic cells, an osteoconductive scaffold, osteoinductive growth factors, and a stable mechanical environment, all underpinned by robust vascularity.
Nonunions are broadly categorized into hypertrophic, oligotrophic, and atrophic variants, each dictating a distinct surgical philosophy. Hypertrophic nonunions are characterized by abundant, "elephant shoe" callus formation, indicating excellent biological vitality but a profound lack of mechanical stability; these are classically treated with rigid stabilization alone. Conversely, atrophic nonunions exhibit no callus formation and sclerotic, tapered bone ends, representing a biological desert that requires aggressive debridement, decortication, and the introduction of autologous bone graft or orthobiologics alongside mechanical stabilization. Oligotrophic nonunions fall on the spectrum between the two, typically requiring both biological augmentation and mechanical revision.
The epidemiology of nonunions varies drastically by anatomical site, largely driven by the local vascular anatomy and the magnitude of deforming forces. Pelvic ring nonunions are relatively rare but catastrophic, typically resulting from the under-treatment of highly unstable Vertical Shear (VS) or severe Anteroposterior Compression (APC) injuries. Clavicular nonunions, while historically considered rare when treated non-operatively, have seen a shifting epidemiological profile; midshaft fractures carry an overall nonunion rate of approximately 5-15% depending on displacement, whereas lateral third fractures (Neer Type II) carry a notoriously high nonunion rate approaching 30% due to the suspensory forces of the coracoclavicular ligaments. Proximal humeral nonunions are increasingly prevalent in the geriatric population, often secondary to the failure of locking plate constructs in severely osteopenic bone subjected to the massive multidirectional forces of the rotator cuff. Finally, femoral neck nonunions remain a devastating complication, occurring in 10-30% of displaced intracapsular fractures, threatening the viability of the femoral head and the biomechanical integrity of the entire hip joint.
The Biological and Mechanical Interplay
Understanding the precise etiology of a nonunion is the cornerstone of successful revision surgery. The surgeon must systematically evaluate the host's physiological status, including nutritional markers (albumin, prealbumin), endocrinopathies (diabetes mellitus, thyroid dysfunction), pharmacological impediments (chronic NSAID use, corticosteroids), and social habits (tobacco use, which drastically reduces microvascular perfusion). Furthermore, occult infection must always be ruled out; a "septic nonunion until proven otherwise" mentality is mandatory. Preoperative serological markers, including Erythrocyte Sedimentation Rate (ESR) and C-Reactive Protein (CRP), should be routinely obtained, and any elevation warrants intraoperative tissue cultures and potentially a staged reconstructive approach utilizing the Masquelet technique.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of regional anatomy and the specific biomechanical forces acting upon the fracture fragments is non-negotiable for the reconstructive orthopedic surgeon. Each anatomical region presents a unique set of challenges that must be neutralized to achieve solid osseous union.
Pelvis and Acetabulum Biomechanics
The pelvic ring functions as a complex biomechanical arch, transferring the axial load of the torso from the sacrum across the sacroiliac (SI) joints to the acetabula and lower extremities. Pennal and Massiah classified pelvic nonunions into three primary groups based on the original deforming force vectors, which dictate the specific pattern of instability. Anteroposterior Compression (APC) injuries are characterized by symphyseal diastasis and external rotation of the hemipelvis, often leading to anterior instability and posterior sacroiliac joint disruption. Lateral Compression (LC) injuries are driven by internal rotation forces, frequently resulting in impacted sacral fractures and overriding pubic rami fractures. Vertical Shear (VS) injuries represent the most unstable pattern, involving complete osteoligamentous disruption with cephalad displacement of the hemipelvis.
In pelvic nonunions, the anatomical location dictates the biological character of the nonunion. The sacroiliac region and posterior pelvic ring typically exhibit an avascular, atrophic nonunion pattern due to the massive soft tissue stripping sustained during the initial trauma and the precarious intraosseous vascularity of the sacrum. This necessitates aggressive decortication and robust autogenous bone grafting. Conversely, the anterior ring and pubic rami often present with hypervascular (hypertrophic) nonunions, where the abundant muscular envelope of the rectus abdominis and adductor complex maintains blood supply; here, rigid stabilization alone may suffice to achieve union. Acetabular nonunions are exceedingly rare, typically occurring only in the context of widely displaced, unreduced articular fragments or unrecognized transverse fracture patterns that undergo cyclic loading during weight-bearing.
Clavicular Suspensory Mechanics
The biomechanical environment of the clavicle is highly complex, acting as the sole osseous strut connecting the axial skeleton to the upper extremity. The clavicle is subjected to constant, multidirectional forces. The medial fragment is invariably drawn superiorly and posteriorly by the relentless pull of the sternocleidomastoid and trapezius muscles. Concurrently, the lateral fragment is driven inferiorly by the weight of the arm and pulled medially by the powerful pectoralis major and latissimus dorsi muscles.
This dynamic muscular antagonism creates a highly unfavorable environment for secondary fracture healing if displacement is significant. In midshaft nonunions, the fracture ends often become encased in dense, avascular fibrous tissue, with the medullary canals becoming heavily sclerotic and plugged. Lateral third clavicular nonunions present an even greater challenge; if the fracture occurs medial to the coracoclavicular (CC) ligaments (conoid and trapezoid), the medial fragment is completely unconstrained, leading to massive superior displacement and a high rate of atrophic nonunion.
Proximal Humerus and the Rotator Cuff
Nonunions of the proximal humerus present a unique biomechanical challenge dominated by the multidirectional deforming forces exerted by the rotator cuff musculature. The proximal humerus is essentially a dynamic fulcrum. The supraspinatus and infraspinatus exert a powerful superior and posterior pull on the greater tuberosity fragment. The subscapularis forcefully internally rotates and displaces the lesser tuberosity medially. Meanwhile, the pectoralis major exerts a strong medializing force on the humeral shaft.
When a fracture fails to unite, these forces lead to profound displacement, often resulting in severe varus collapse of the articular segment. Furthermore, the proximal fragment is highly cancellous and frequently osteopenic, particularly in the elderly female demographic. This makes standard screw purchase precarious, leading to a high risk of hardware pullout ("cut-out") and subsequent mechanical failure. The surgeon must not only achieve rigid fixation but must also actively neutralize these muscular forces to prevent catastrophic failure of the revision construct.
Femoral Neck and Pauwels' Principles
The femoral neck is subjected to massive biomechanical forces, routinely supporting loads equivalent to multiple times the patient's body weight during the normal gait cycle. The forces acting across a femoral neck fracture or nonunion are dictated by the fracture angle, famously described by Friedrich Pauwels. Pauwels Type I fractures (less than 30 degrees from the horizontal) experience primarily compressive forces, which are highly conducive to osteogenesis. However, Pauwels Type III fractures (greater than 50 degrees from the horizontal) are subjected to massive vertical shear forces.
Femoral neck nonunions almost universally occur in the setting of these high-shear environments. The shear forces actively prevent the formation of a stable fibrin clot and disrupt the delicate microvascular angiogenesis required for endochondral ossification. Furthermore, the vascular supply to the femoral head—primarily the deep branch of the medial femoral circumflex artery (MFCA) and the lateral epiphyseal artery system—is highly vulnerable to disruption at the time of injury. Nonunion threatens the viability of the femoral head, and the surgeon must meticulously assess head viability before attempting any joint-preserving osteosynthesis.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for a nonunion is highly nuanced, requiring a comprehensive assessment of the patient's physiological age, functional demands, bone stock, and local soft tissue envelope. Operative intervention is generally indicated for patients exhibiting chronic, debilitating pain, progressive clinical deformity, mechanical instability, and a profound inability to perform activities of daily living (ADLs).
Conservative management of established, symptomatic nonunions in these four critical anatomical regions universally fails to relieve pain or restore mechanics. However, surgical intervention is not without significant risk, and strict adherence to established contraindications is paramount to avoid catastrophic complications such as deep space infection, catastrophic hardware failure, or amputation.
| Anatomical Region | Primary Surgical Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Pelvis / Acetabulum | Intractable pelvic ring pain; progressive leg length discrepancy; severe gait dysfunction; neurological impingement from hypertrophic callus. | Active pelvic osteomyelitis (requires staged approach); medically unstable patient; non-ambulatory baseline status. | Severe osteoporosis precluding fixation; massive soft tissue compromise (e.g., Morel-Lavallée lesion sequelae); active smoking. |
| Clavicle | Painful midshaft nonunion > 6 months; symptomatic lateral third nonunion; impending skin breakdown; severe shoulder girdle weakness/fatigue. | Asymptomatic nonunion in an elderly/low-demand patient; active local soft tissue infection. | Poor soft tissue envelope overlying the clavicle; heavy tobacco use; active intravenous drug use. |
| Proximal Humerus | Painful pseudarthrosis; severe varus collapse limiting forward elevation; rotator cuff dysfunction secondary to tuberosity displacement. | Active glenohumeral joint infection; completely paralyzed upper extremity (e.g., severe brachial plexus avulsion). | Profound osteopenia (may favor arthroplasty over osteosynthesis); advanced physiological age with low functional demand. |
| Femoral Neck | Viable femoral head in a physiologically young patient (< 60 yrs) with a shear-pattern nonunion; painful nonunion in the elderly (indication for arthroplasty). | Active hip joint sepsis; medically unfit for major anesthesia. | Pre-existing advanced acetabular osteoarthritis (contraindicates joint-preserving osteotomy or hemiarthroplasty; dictates THA); active smoking. |
In the context of the femoral neck, the distinction between joint-preserving surgery and arthroplasty is critical. An angulation osteotomy is strictly contraindicated if there is radiographic evidence of advanced avascular necrosis (AVN) with subchondral collapse, or if there is pre-existing traumatic or primary osteoarthritis of the acetabulum. In such scenarios, prosthetic replacement (Total Hip Arthroplasty) becomes the mandatory procedure.
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the distinguishing hallmark of the master orthopedic surgeon. The complexity of nonunion surgery dictates that the operation must be entirely conceptualized, templated, and mentally executed long before the scalpel touches the skin. Inadequate imaging or failure to anticipate bone defects will inevitably lead to intraoperative compromises and subsequent construct failure.
Advanced Imaging Modalities
Standard orthogonal radiographs are merely the starting point. For pelvic nonunions, Pennal views are critical. Cephalad (Outlet) and caudal (Inlet) tangential views taken at 45 degrees relative to the standard AP projection provide a three-dimensional understanding of the deformity. The Inlet view assesses anterior-posterior translation and internal/external rotation, while the Outlet view evaluates vertical displacement and leg length discrepancy. High-resolution Computed Tomography (CT) with 3D reconstructions is the absolute gold standard for defining the exact osseous anatomy, identifying avascular fragments, quantifying bone loss, and planning the trajectory of internal fixation.
For clavicular and proximal humeral nonunions, CT imaging is invaluable for assessing the degree of medullary sclerosis and the exact volume of the bone defect, which dictates the volume of autologous bone graft required. In the femoral neck, assessing the viability of the femoral head is paramount. While plain radiographs may show sclerosis or subchondral cysts suggestive of AVN, Magnetic Resonance Imaging (MRI) without contrast is highly sensitive and specific for evaluating the vascular status of the proximal segment. If MRI is contraindicated, intraoperative assessment of punctate bleeding from the femoral head upon drilling is a reliable, albeit late, indicator of viability.
Digital Templating and Positioning
Digital templating is utilized to determine the appropriate implant size, length, and specific screw trajectories. For a Pauwels angulation osteotomy of the femoral neck, the surgeon must calculate the exact wedge of bone to be resected from the intertrochanteric region to convert the vertical shear angle (e.g., 70 degrees) to a compressive angle (e.g., 20 degrees). This requires precise measurement of the neck-shaft angle and the planned osteotomy angle on preoperative AP pelvic radiographs.
Patient positioning is dictated by the surgical approach and must allow for unhindered intraoperative fluoroscopy.
* Pelvis: Depending on the nonunion site, the patient is placed supine (for anterior ring and ilioinguinal approaches) or prone (for posterior ring and sacral approaches) on a completely radiolucent Jackson table.
* Clavicle: The patient is placed in a modified beach-chair position with a bump between the scapulae to allow the shoulder girdle to fall posteriorly, aiding in the reduction of the medial fragment.
* Proximal Humerus: The beach-chair position is universally preferred, allowing gravity to assist with the inferior traction of the arm and providing excellent access to the anterior and lateral shoulder.
* Femoral Neck: For an angulation osteotomy, the patient is placed supine on a radiolucent flat table with a bump under the ipsilateral hemipelvis, allowing for free draping of the leg to assess clinical alignment and range of motion following fixation.
Step-by-Step Surgical Approach and Fixation Technique
The execution of nonunion surgery requires aggressive biological preparation combined with uncompromising mechanical stabilization. The surgical steps must be followed with rigid discipline.
Pelvic Ring Reconstruction
Historically, nonoperative treatment of pelvic nonunions yielded abysmal functional outcomes. Pennal and Massiah noted that of 24 patients treated nonoperatively, only five returned to their pre-injury employment. Operative stabilization and bone grafting result in high rates of solid bony union and functional restoration. Mears and Velyvis reported 79% excellent and 21% satisfactory results following bone grafting and realignment procedures.
- Surgical Approach: The ilioinguinal or modified Stoppa approach is utilized for anterior pathology, allowing access to the symphysis pubis, superior pubic ramus, and quadrilateral plate. A posterior approach (e.g., longitudinal incision lateral to the PSIS) is used for the sacroiliac complex and sacrum.
- Debridement and Decortication: The nonunion site is radically debrided. All interposed fibrous tissue, necrotic cartilage, and sclerotic bone are excised down to bleeding, punctate bone—the classic "paprika sign." Failure to achieve bleeding bone guarantees failure of the procedure.
- Reduction: Specialized pelvic reduction forceps (e.g., Jungbluth clamps, Farabeuf clamps) are applied to correct multiplanar deformities. Schanz pins placed into the iliac crests can be used as "joysticks" to manipulate the hemipelvis.
- Bone Grafting: Copious autologous cancellous bone graft, typically harvested from the posterior iliac crest, is densely packed into the defect to provide an osteoconductive and osteogenic environment.
- Rigid Internal Fixation: Multi-hole reconstruction plates (3.5 mm or 4.5 mm) are meticulously contoured to the pelvic brim or posterior pelvis. Absolute stability is required; hence, dual plating or the use of heavy locking constructs is often necessary.
Clavicular Midshaft Osteosynthesis
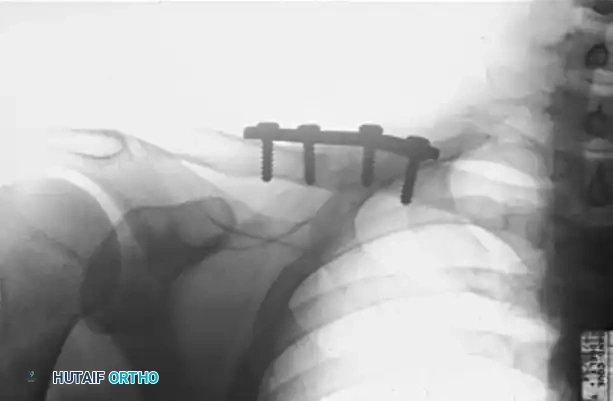
Operative intervention is indicated for patients exhibiting pain, weakness, and cosmetic deformity. The gold standard for midshaft nonunions is compression plating combined with autologous iliac crest bone grafting. Davids et al. emphasize the absolute necessity of opening and reaming the sclerotic medullary canal to restore endosteal blood flow.

Figure A: Preoperative radiograph demonstrating a hypervascular nonunion of the clavicle. The patient presented with severe pain and instability 1.5 years following the initial fracture, exacerbated by a recent fall.
- Approach: A superior or anteroinferior incision is made along the clavicular axis. The anteroinferior approach is increasingly favored as it avoids placing the incision directly over the hardware, reducing the risk of wound dehiscence, and allows for longer screw purchase in the AP plane. The supraclavicular nerves must be meticulously identified and preserved to prevent painful neuromas.
- Preparation: The fibrous nonunion is sharply excised. The sclerotic medullary canals of both the medial and lateral fragments are aggressively drilled with a 2.5mm or 3.2mm drill bit to open the intramedullary space and restore marrow continuity.
- Grafting: Corticocancellous autograft from the anterior iliac crest is harvested and contoured to fit the defect perfectly.
- Plating: A specially contoured, low-profile locking clavicle plate is applied. Compression is achieved across the nonunion site using eccentric drilling techniques in the dynamic compression holes prior to inserting locking screws.
Figure B: Postoperative radiograph at 2.5 months demonstrating solid osseous union following aggressive decortication, application of a superior compression plate, and autologous bone grafting.
For highly recalcitrant cases, such as radiation-induced pathological fractures or post-infectious nonunions with massive bone loss, Fuchs et al. demonstrated success utilizing a free vascularized graft harvested from the medial femoral condyle, anastomosed to the transverse cervical vessels, combined with robust plate fixation.
Proximal Humerus Tension Band and Buttress Plate Technique
To counteract the massive deforming forces of the rotator cuff in osteopenic bone, Healy, Jupiter, Kristiansen, and White described a highly effective, biomechanically superior combination technique utilizing a buttress plate augmented with heavy tension band wiring.
By weaving a heavy nonabsorbable suture through the rotator cuff tendon insertions and anchoring it directly to the plate, the surgeon actively neutralizes the muscular pull. This brilliant biomechanical maneuver converts the distracting forces of the supraspinatus into compressive forces across the fracture site and protects the proximal metaphyseal screws from catastrophic pullout.
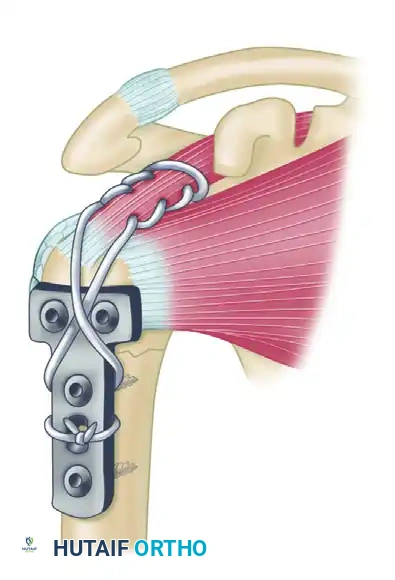
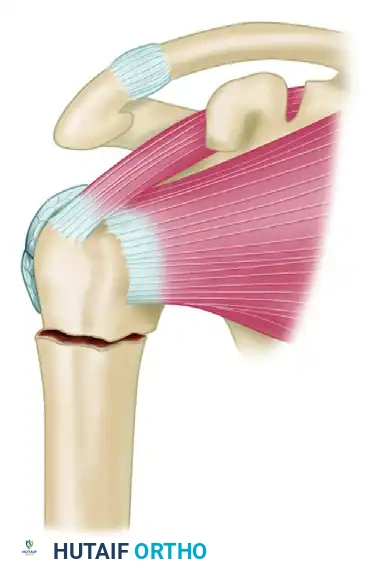
Step 1: Identification of the nonunion site. The proximal fragment is subjected to superior displacement by the supraspinatus, while the humeral shaft is pulled medially by the pectoralis major.
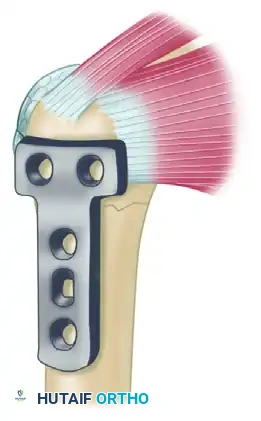
Step 2: Following radical debridement of the nonunion, opening of the medullary canal, and placement of autologous bone graft, a T-plate or anatomically contoured proximal humeral locking plate is applied to the lateral aspect of the humerus to provide a rigid buttress against varus collapse.
Step 3: A heavy, nonabsorbable suture (e.g., #5 FiberWire or equivalent ultra-high-molecular-weight polyethylene suture) is woven deeply through the rotator cuff tendons (supraspinatus and infraspinatus) utilizing a locking Krackow stitch configuration. The suture limbs are then passed through the designated proximal suture holes of the plate and tied securely in a figure-of-eight fashion while the arm is held in slight abduction. This effectively neutralizes the pull of the rotator cuff on the proximal fragment, offloading the screws.
Femoral Neck Angulation Osteotomy
The angulation (valgus-producing) osteotomy is a powerful joint-preserving procedure based on Pauwels' biomechanical principles. It is primarily indicated for younger patients (typically under 60 years of age) with a viable femoral head and a vertical shear nonunion. The goal is to change the inclination of the fracture surfaces, converting destructive shear forces into constructive compressive forces. Additionally, it shifts the mechanical axis and line of weight-bearing medially, reducing the bending moment on the hip joint.
- Approach: A standard lateral approach to the proximal femur is utilized.
- Guide Wire Placement: A guide wire is placed into the femoral head, parallel to the nonunion line. A second guide wire is placed at the pre-calculated angle (e.g., 130 degrees minus the desired wedge angle) to dictate the trajectory of the dynamic hip screw (DHS) lag screw.
- Osteotomy: A laterally based closing wedge osteotomy is performed at the level of the lesser trochanter. The size of the wedge corresponds exactly to the angle required to convert the nonunion to a Pauwels Type I configuration (typically 20-30 degrees).
- Fixation: The osteotomy is closed by abducting the distal fragment, and the construct is stabilized using a variable-angled DHS or a specialized locking side plate (e.g., 120-degree blade plate or locking proximal femur plate). Compression is applied across both the osteotomy site and the nonunion site.
Modern literature reports union rates ranging from 86% to 88% following this procedure when executed flawlessly. The functional outcome is directly proportional to the mechanical and physiological status of the nonunion prior to surgery. While function can approach normal if the head is viable, surgeons must counsel patients that excellent early results may degrade over 3 to 5 years due to progressive post-traumatic arthritic changes or late-onset AVN.
Complications, Incidence Rates, and Salvage Management
The surgical management of nonunions is fraught with potential complications. The host biology is often already compromised, and the local soft tissues have been subjected to previous trauma and surgery. The surgeon must be prepared to manage catastrophic failures and employ complex salvage strategies.
| Complication | Estimated Incidence | Anatomical Region Most Affected | Salvage Management Strategy |
|---|---|---|---|
| Deep Surgical Site Infection (SSI) | 3% - 8% | Pelvis, Proximal Humerus | Radical debridement, hardware removal (if unstable), placement of antibiotic-impregnated cement spacer (Masquelet technique), 6 weeks IV antibiotics, staged definitive reconstruction. |
| Avascular Necrosis (AVN) | 15% - 30% | Femoral Neck | Conversion to Total Hip Arthroplasty (THA). If patient is extremely young, consideration of free vascularized fibular graft (rarely successful post-collapse). |
| Hardware Failure / Pullout | 5% - 12% | Proximal Humerus, Clavicle | Revision open reduction internal fixation (ORIF) with longer/thicker plates, dual plating (clavicle), augmentation with intramedullary fibular strut allograft, and tension band wiring. |
| Neurovascular Injury | 1% - 4% | Pelvis (L5/S1 roots), Clavicle (Subclavian vessels) | Intraoperative vascular surgery consultation for vessel repair. Neurological injuries are typically managed expectantly with serial EMG/NCS; exploration if complete transection is suspected. |
| Persistent Recalcitrant Nonunion | 5% - 10% | All regions | Re-evaluation of biological vs. mechanical failure. Addition of rhBMP-2 (Bone Morphogenetic Protein), massive autogenous grafting, or free vascularized bone transfer (e.g., medial femoral condyle). |
Prosthetic Replacement and Arthrodesis as Salvage
When joint-preserving osteosynthesis fails, or when it is contraindicated from the outset, salvage procedures must be employed. Prosthetic replacement (hemiarthroplasty or total hip arthroplasty) offers an immediate, definitive solution to femoral neck nonunions, particularly in the elderly population. It is indicated in adults younger than 50 to 60 years old only if the femoral head is avascular and an arthrodesis is deemed undesirable. It is important to note that complication rates (such as dislocation, infection, and periprosthetic fracture) are significantly higher when performing arthroplasty for nonunions compared to acute fractures, necessitating meticulous surgical technique, utilization of dual-mobility bearing surfaces, and precise soft-tissue balancing.
Hip arthrodesis is an extreme salvage procedure that is rarely performed in the modern era of advanced arthroplasty, but it remains a viable option in highly specific scenarios—particularly in young, heavy laborers with unilateral hip pathology, a non-viable femoral head, and a history of deep infection precluding arthroplasty. According to Gill, the primary advantages of an arthrodesis are absolute freedom from pain and permanent mechanical stability. However, the profound alteration in gait kinematics and the subsequent accelerated degeneration of the lumbar spine and contralateral knee make this a procedure of absolute last resort.
Phased Post-Operative Rehabilitation Protocols
Regardless of the anatomical site, the postoperative management of surgically treated nonunions requires a delicate, highly supervised balance between protecting the fragile osteosynthesis construct and preventing debilitating soft-tissue contractures and joint stiffness. The rehabilitation protocol must be phased and dictated by radiographic evidence of healing.
- Pelvis and Acetabulum: Patients are typically restricted to toe-touch weight-bearing (TTWB) or strict non-weight-bearing (NWB) on the affected side for 8 to 12 weeks. Deep vein thrombosis (DVT) prophylaxis is absolutely mandatory given the high risk of venous stasis in pelvic surgery. Progression to partial weight-bearing is permitted only after radiographic evidence of bridging callus is confirmed on AP and Judet views.
- Clavicle: The arm is supported in a broad arm sling for 2 to 4 weeks to offload the weight of the extremity. Pendulum exercises and elbow/wrist/hand range of motion begin immediately to prevent distal stiffness. However, active elevation above 90 degrees, cross-body adduction, and any heavy lifting are strictly restricted until clinical and radiographic union is confirmed (usually 8 to 10 weeks).
- Proximal Humerus: The shoulder is highly prone to adhesive capsulitis. Passive range of motion (PROM) in forward elevation and external rotation is initiated early (within the first week) to prevent capsular contracture. Active range of motion (AROM) is strictly delayed until 6 weeks to protect the delicate tension band construct and allow the tuberosities to heal to the shaft. Resistance training is not initiated until 12 weeks.
- Femoral Neck (Osteotomy): Protected weight-bearing with crutches or a walker (typically 20 lbs flat-foot weight-bearing) is required for 8 to 12 weeks. Active hip abduction is limited to prevent excessive stress on the greater trochanter. Serial radiographs are scrutinized at 2, 6, 12, and 24 weeks for maintenance of the valgus correction, absence of hardware migration, and progressive obliteration of the nonunion line.
Summary of Landmark Literature and Clinical Guidelines
The operative management of these complex nonunions is heavily guided by historical and contemporary landmark literature. The foundational principles of pelvic nonunion management were established by Pennal and Massiah, who first articulated the disastrous outcomes of nonoperative management. Mears and Velyvis later codified the modern approach of aggressive debridement, rigid internal fixation, and autologous grafting, establishing the benchmark for functional recovery.
In the realm of acetabular surgery, the work of Letournel and Judet remains unparalleled; their massive series demonstrated that anatomical reduction of the articular surface acutely is the ultimate prophylaxis against nonunion
