Comprehensive Management of Tibial Shaft Fractures: Operative Techniques and Evidence-Based Protocols
Key Takeaway
Tibial shaft fractures are the most common long bone fractures, often complicated by precarious vascularity and limited soft-tissue coverage. Management requires a nuanced approach, balancing soft-tissue preservation with mechanical stability. While closed, low-energy fractures may be managed with functional bracing, high-energy, unstable, or open fractures necessitate operative intervention. Intramedullary nailing remains the gold standard, though circular external fixation is invaluable for complex periarticular or highly comminuted patterns.
Introduction and Biomechanics
Fractures of the tibial shaft represent the most common long bone fractures encountered in orthopedic trauma. Due to its unique anatomical location and biomechanical environment, the tibia cannot be treated by following a simple, rigid set of rules. Approximately one-third of the tibial surface is subcutaneous throughout its length, making it highly vulnerable to direct trauma and resulting in a higher incidence of open fractures than any other major long bone.
The blood supply to the tibia is notoriously precarious compared to bones enveloped by heavy musculature. The primary endosteal supply is derived from the nutrient artery (a branch of the posterior tibial artery), which enters the posterolateral cortex at the proximal third of the diaphysis. High-energy trauma, particularly transverse or short oblique fractures, often completely disrupts this endosteal circulation. In such cases, the bone must rely on the secondary periosteal blood supply, which itself is frequently compromised by the initial soft-tissue stripping.
Furthermore, the presence of hinge joints at both the knee and the ankle allows for virtually no compensatory adjustment for rotary deformity after a fracture. Special care is absolutely necessary during reduction to correct any such deformity, as axial or rotational malalignment alters the loading characteristics in adjacent joints, inevitably hastening the development of posttraumatic osteoarthritis.
Clinical Evaluation and Initial Management
Evaluation of tibial fractures must begin with a detailed history and physical examination, adhering strictly to ATLS protocols for high-energy trauma. The limb is inspected for open wounds, soft-tissue crushing, degloving, or contusions.
A thorough neurovascular examination is paramount. The ipsilateral femur, knee, ankle, and foot must also be examined to rule out floating knee injuries or syndesmotic disruptions.
🚨 SURGICAL WARNING: Compartment Syndrome
High-energy tibial fractures carry a significant risk of acute compartment syndrome. A pulse deficit or neurological deficit (such as decreased sensation in the first web space or weakness in toe extension) is a late and unreliable sign. Pain out of proportion to the injury and severe pain with passive stretch of the involved compartment's muscles are the hallmark clinical indicators. Immediate fasciotomy is required if compartment pressures are elevated or clinical suspicion is high.
When the initial examination is completed, the limb should be gently realigned and splinted. Open wounds must be irrigated gently, dressed under sterile conditions, and appropriate tetanus and intravenous antibiotic prophylaxis administered immediately.
Radiographic Evaluation
Plain anteroposterior (AP) and lateral radiographs that include the knee and ankle are mandatory. Oblique radiographic views at 45 degrees are sometimes required to detect nondisplaced spiral fractures or subtle articular extensions.

Radiographs of the contralateral intact tibia are frequently necessary to evaluate native length and mechanical axis in fractures with severe comminution or segmental bone loss.
Prognostic Factors and Acceptable Alignment
The goals of treatment are to obtain a healed, well-aligned fracture; pain-free weight bearing; and a functional range of motion of the knee and ankle joints.
According to Nicoll, the most critical factors in the prognosis of tibial shaft fractures are:
1. The amount of initial displacement.
2. The degree of comminution.
3. The presence of infection.
4. The severity of the soft-tissue injury (excluding infection).
Hoaglund and States classified fractures as resulting from either high-energy (e.g., motor vehicle collisions, crush injuries) or low-energy trauma (e.g., skiing falls). High-energy fractures, which include 90% of open fractures, take an average of 6 months to heal, whereas low-energy fractures heal in approximately 4 months. Suman and Böstman noted that initial displacement of more than 50% of the tibial width significantly increases the risk of delayed union, nonunion, and loss of reduction.
Parameters for Acceptable Alignment
Maintaining fracture alignment is difficult in certain fracture types. While recommendations in the literature vary, Trafton’s criteria remain the gold standard for acceptable reduction:
* Varus-valgus angulation: Less than 5 degrees.
* Anteroposterior (procurvatum/recurvatum) angulation: Less than 10 degrees.
* Rotation: Less than 10 degrees.
* Shortening: Less than 15 mm.
Tarr et al. and Puno et al. demonstrated that distal tibial malalignment is more poorly tolerated than proximal malalignment due to its profound effect on ankle joint contact stresses.
Nonoperative Management: Indications and Limitations
Although commonly advocated in the past, nonoperative treatment is now generally reserved for closed, stable, isolated, minimally displaced fractures caused by low-energy trauma, as well as some stable low-velocity gunshot fractures.
Sarmiento, Nicoll, Dehne, and Weissman demonstrated that closed treatment with casting or functional bracing (patellar tendon-bearing braces) can be highly effective. Sarmiento reported union rates of up to 97.5% in selected fractures treated with early weight-bearing functional braces.
However, for closed treatment to succeed, the cast or brace must maintain acceptable fracture alignment, and the fracture pattern must allow early weight bearing. Repeated attempts at closed manipulation should be avoided to prevent further soft-tissue trauma. Nonoperative treatment is contraindicated in noncompliant patients, obese patients, or those with massive limb edema where alignment cannot be maintained.
Operative Management: Evidence and Indications
Operative treatment is indicated for most tibial fractures caused by high-energy trauma. These fractures are usually unstable, comminuted, and associated with varying degrees of soft-tissue trauma. Operative fixation allows early motion, provides vital soft-tissue access for wound care, and avoids the systemic complications associated with prolonged immobilization.
Specific indications for internal fixation include:
* Open fractures requiring complex soft-tissue reconstruction.
* Associated ipsilateral femur fractures (floating knee).
* Polytrauma patients.
* Fractures associated with compartment syndrome or vascular injury.
* Segmental fractures or those with significant bone loss.
* Failure to maintain acceptable alignment with closed methods.
Intramedullary Nailing vs. Casting
Locked intramedullary (IM) nailing is currently the preferred treatment for most diaphyseal tibial shaft fractures requiring operative fixation.
Bone et al. retrospectively compared IM nailing and cast treatment for isolated displaced tibial shaft fractures. Nonunions occurred in only 2% of nailed fractures compared to 10% of casted fractures. Furthermore, 10% of casted fractures healed with unacceptable malalignment, whereas none of the nailed fractures did. Puno et al. and Hooper et al. corroborated these findings in prospective trials, demonstrating superior union rates, lower malunion rates, and faster return to work with IM nailing.
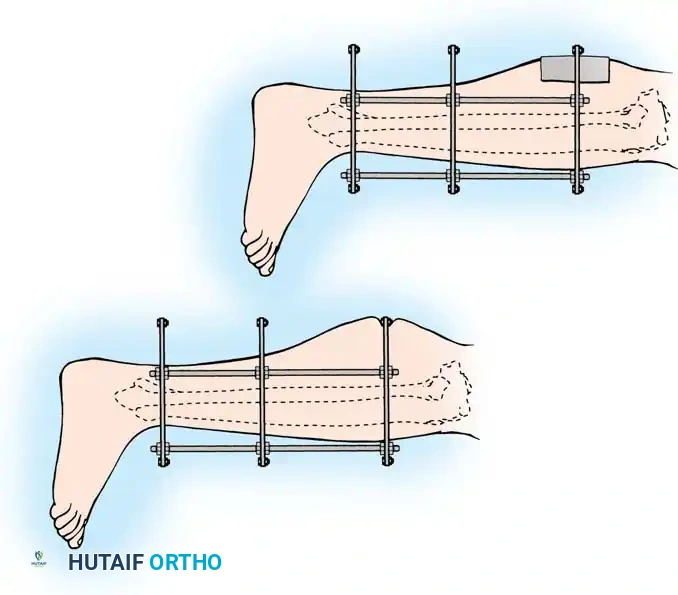
Advanced Surgical Technique: Circular External Fixation
While IM nailing is ideal for diaphyseal fractures, external fixation—particularly circular ring fixators (Ilizarov or Taylor Spatial Frame principles)—is invaluable for severe open fractures, highly comminuted metaphyseal-diaphyseal fractures (AO Type C), and fractures with extensive periarticular involvement.
The following represents a masterclass, step-by-step approach to the application of a circular frame for complex tibial shaft fractures with articular extension.
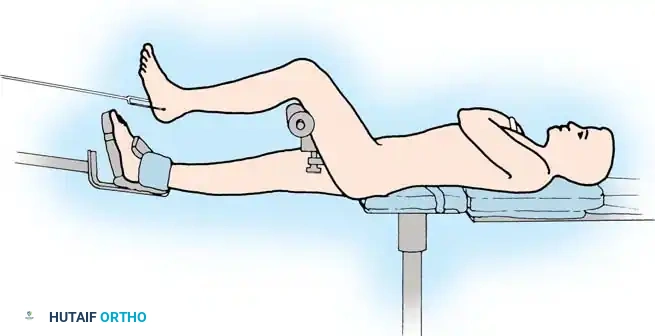
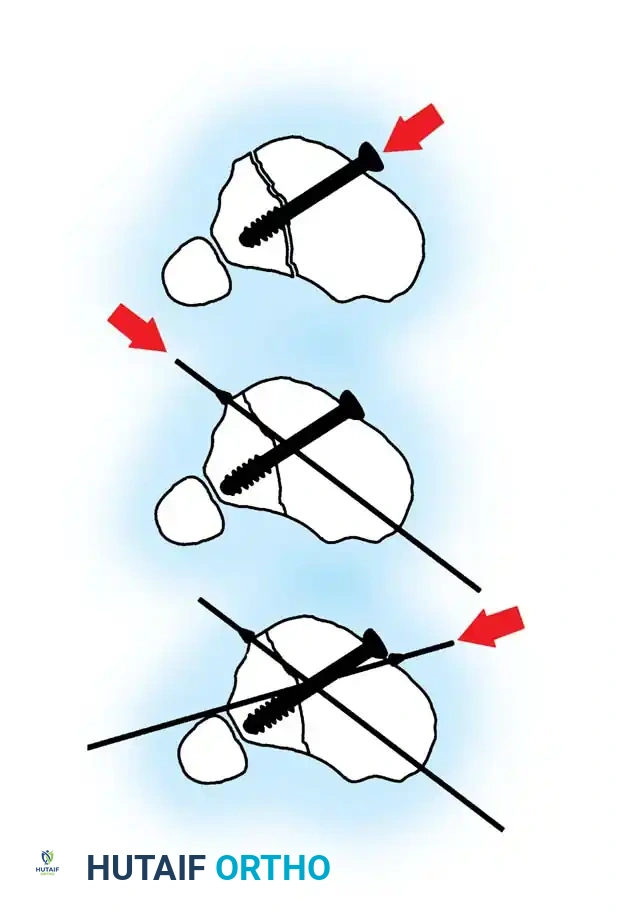
Step 1: Articular Reduction and Provisional Fixation
For fractures extending into the tibial plateau or plafond, anatomic reduction of the articular surface is the absolute first priority.
- Use a small elevator to disimpact the depressed articular surface and reduce it under direct vision or fluoroscopy.
- Use Kirschner wires (K-wires) to hold the fragments temporarily.
- Apply any autologous bone graft or orthobiologics necessary to maintain the segment in position and fill any metaphyseal cancellous defects created by the disimpaction.

- Reduce the metaphyseal fragments and hold them with temporary K-wire fixation.
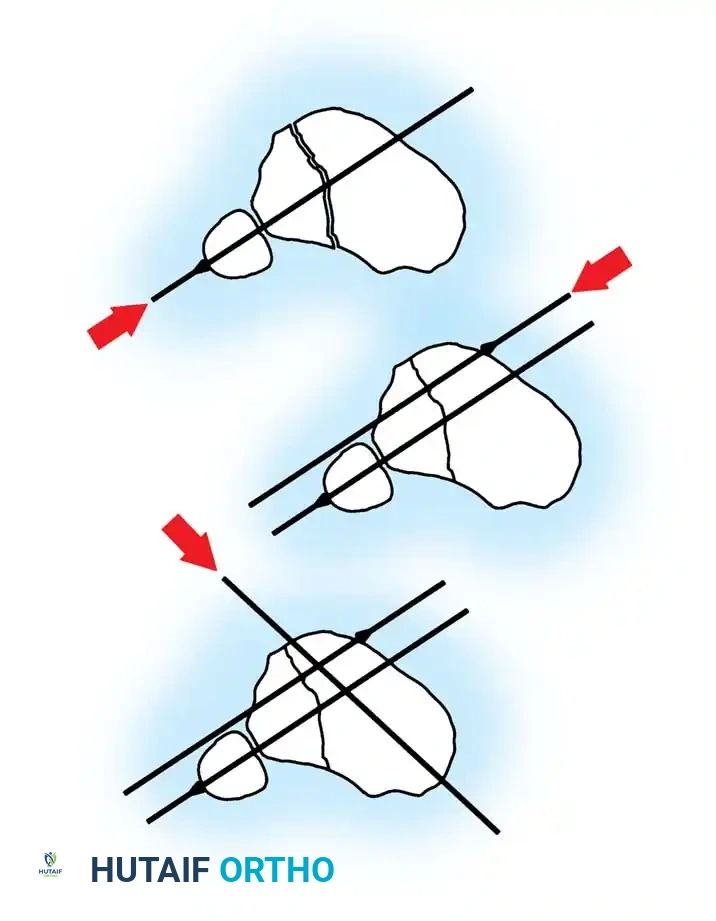
- Use a cannulated screw for definitive articular fixation of any coronal fracture lines. Alternatively, for most fracture lines, place olive wires percutaneously or directly through the incision to fix the fragments dynamically.
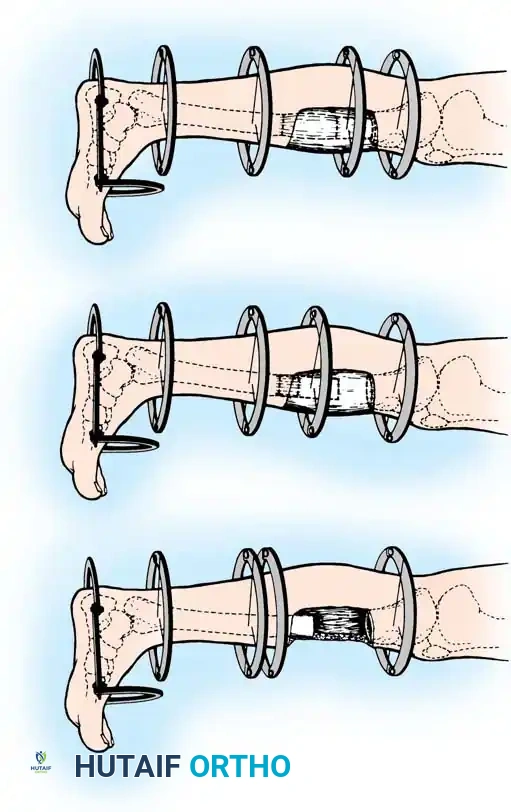
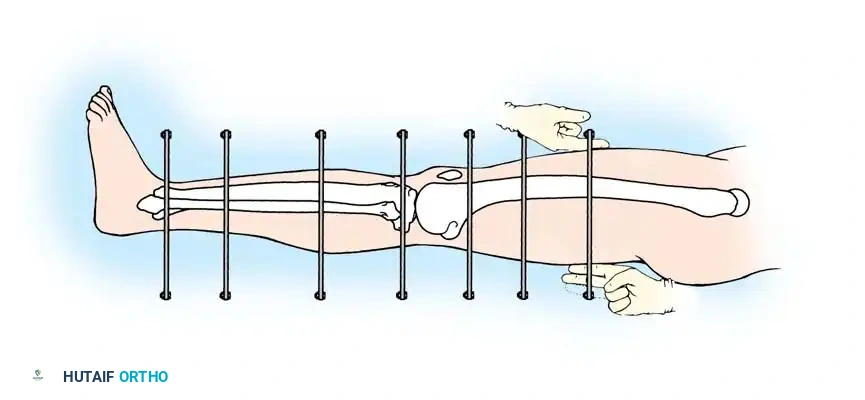
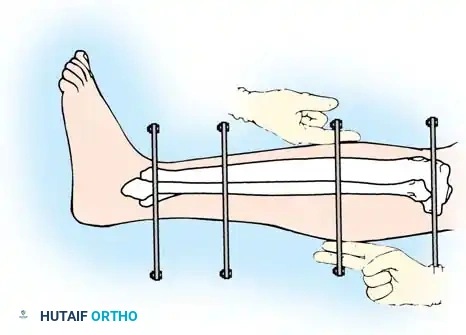
Step 2: Wire Placement and Diastasis Reduction
At least three or four olive wires are necessary to obtain adequate fixation of the articular surfaces.
- If the distal tibiofibular joint (syndesmosis) has been disrupted, use an olive wire to reduce the diastasis by passing the wire from the fibula across the tibia.
- If the fibula has not been plated, ensure that it is pulled out to its full length and that appropriate rotation is maintained before placing the tibia-fibula transfixation wire.
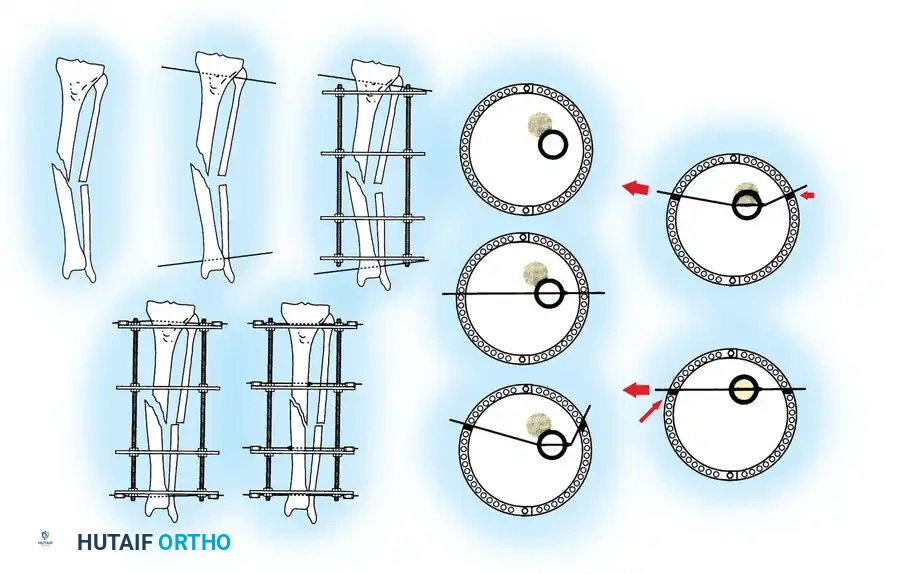
- Place the final wire—a transverse reference wire—just anterior to the fibula. Pass this wire only through the tibia to ensure that it is perfectly parallel to the joint line, approximately 1 cm proximal to the ankle joint.
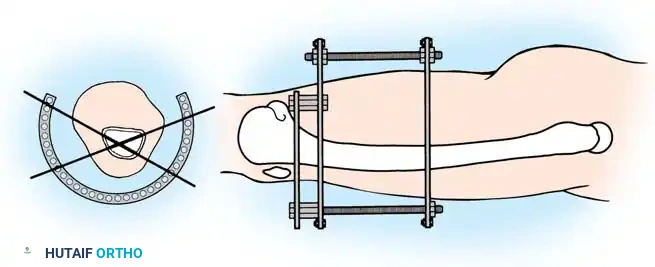
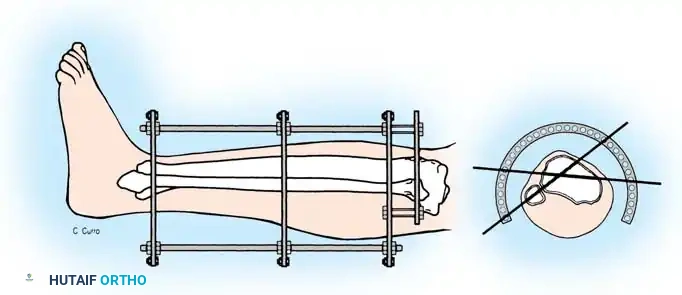
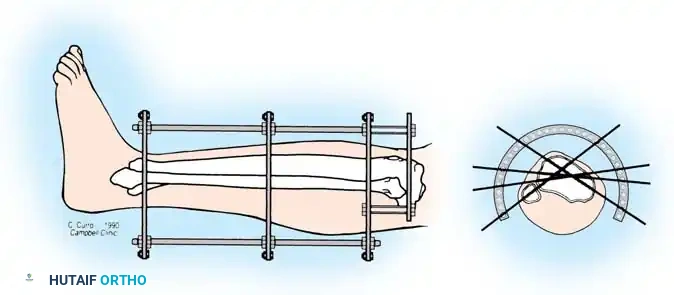
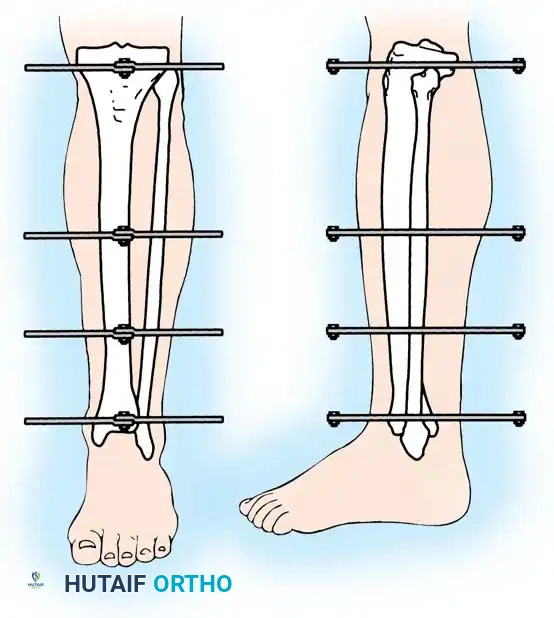
Step 3: Frame Assembly and "Clamshelling"
Once the reference wires are in place, the frame is assembled around the limb.
- "Clamshell" the distal ring (open the ring, place it around the leg, and close it), positioning the ring directly on the transverse reference wire. This critical step ensures that the knee and ankle joints will remain parallel when the distal and proximal rings are eventually connected.
- Attach the remainder of the wires to the free ring. Because the wires may not lie directly in apposition to the ring due to the contour of the leg, build up to the ring by using various posts and washers of different heights to avoid bending the wires and displacing the fracture.
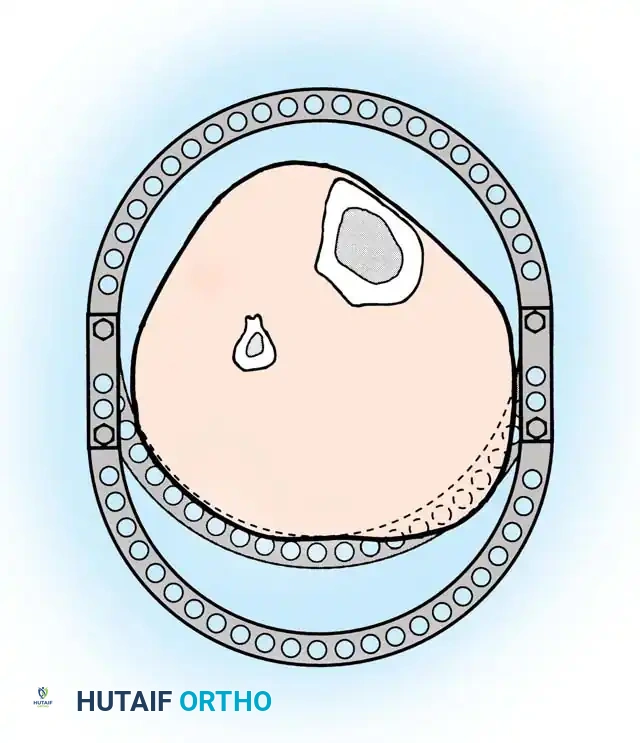
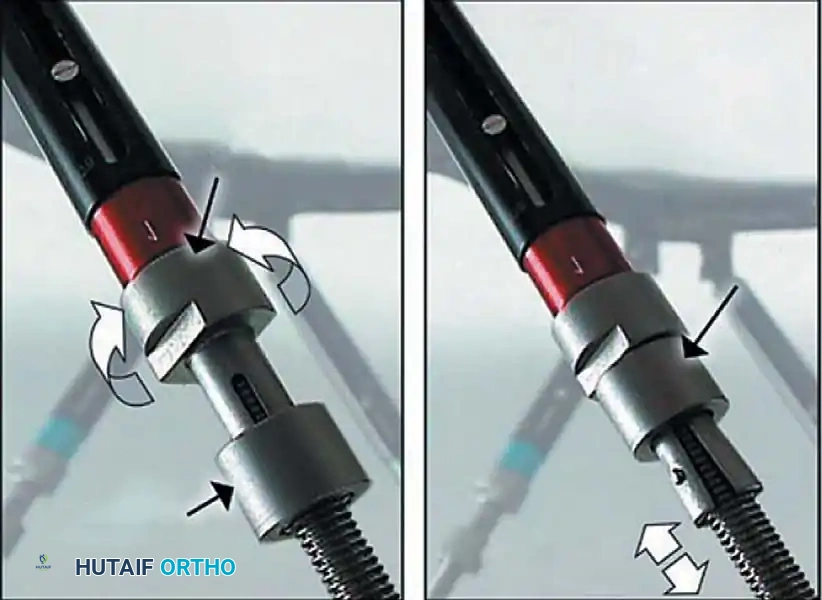
Step 4: Symmetrical Tensioning
Proper tensioning of the wires is what provides the circular frame with its unique biomechanical stability (beam loading).
- Tension the opposing olive wires symmetrically using two-wire tensioners.
- Crucial Step: Perform this tensioning strictly under fluoroscopic control. Asymmetrical tensioning can cause unequal compression across fracture lines, leading to iatrogenic displacement or varus/valgus malalignment.
Step 5: Proximal Extension and Shaft Alignment
Once the periarticular block is secured, attention turns to the diaphyseal comminution.
- Attach the distal ring block to the proximal rings using threaded rods equipped with conical washers. These washers allow for multi-planar variability in reducing and maintaining the overall mechanical axis.

- Use the ring at the level of the proximal shaft extension to reduce proximal shaft comminution.
- Use additional olive or smooth wires to manipulate and maintain shaft alignment, effectively "pulling" large butterfly fragments into the construct. Attach these wires to the mid-distal ring and tension them under fluoroscopy so the reduction can be observed in real-time.

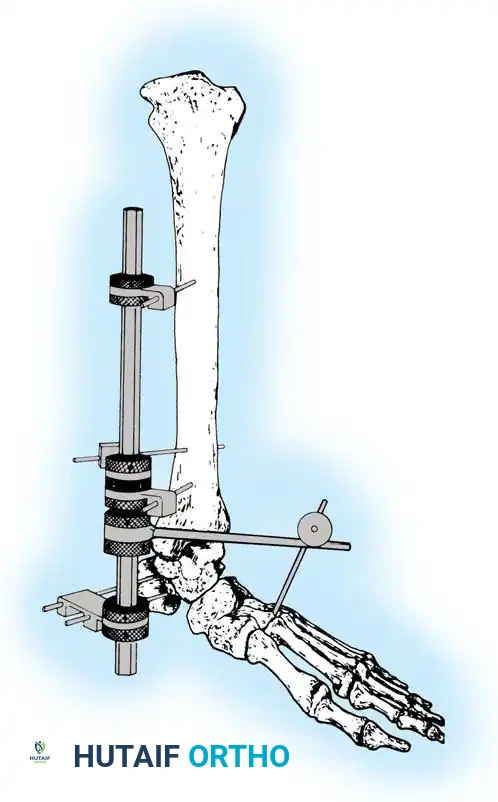
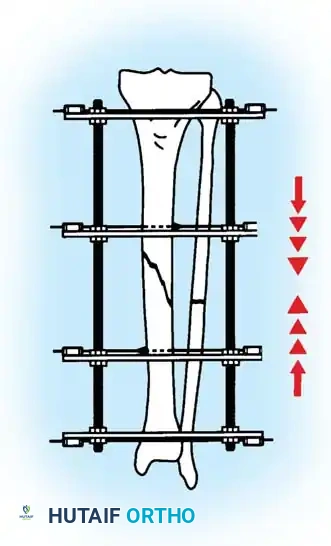
Step 6: Distraction Ligamentotaxis for AO Type C Injuries
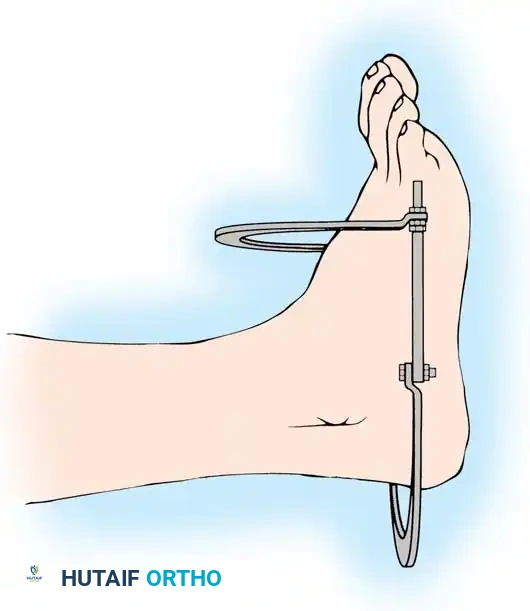
For severe AO Type C injuries with extensive joint involvement, massive metaphyseal comminution, or bone loss, standard reduction techniques may fail. In these scenarios, distraction ligamentotaxis is employed.
- It is highly helpful to preconstruct a four-ring frame with an attached foot frame to maintain distraction at the ankle joint.
- The distraction construct can be as simple as a single calcaneal transfixation pin/wire attached to a distal calcaneal half-ring, or as extensive as a full foot frame attached to the distal tibial ring.
- Attach the proximal tibial rings first, ensuring appropriate soft-tissue clearance (minimum two fingerbreadths) to accommodate postoperative edema.
- Attach the foot frame or calcaneal pin, and perform distraction ligamentotaxis across the ankle joint by adjusting the threaded rods. The tension of the intact joint capsule and ligaments will pull the comminuted articular fragments into alignment.
Clinical Pearl: Open Reduction in Ligamentotaxis
If ligamentotaxis reduction is inadequate (often due to impacted osteochondral fragments or interposed soft tissue), do not over-distract. Perform a limited open procedure to disimpact the fragments directly.
- When reduction is satisfactory, position the distal tibial ring at the level of the fracture. Pass the fixation wires across the fracture fragments, attach them to the ring, and tension them.
- Note: The only difference in this specific technique is that the distal tibial ring is already attached to the preconstructed frame, so it is not necessary to "clamshell" the ring to place it around the wires.
Postoperative Protocol and Complications
Postoperative management is dictated by the fracture pattern, soft-tissue envelope, and the stability of the chosen fixation.
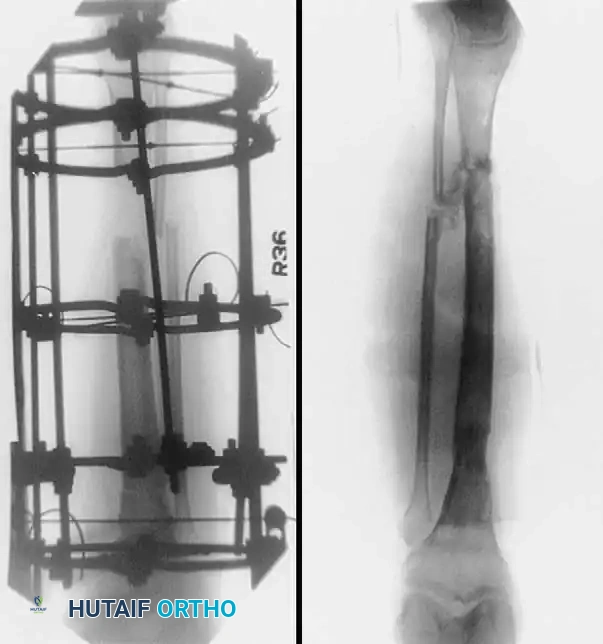
For intramedullary nails in stable patterns, immediate weight-bearing as tolerated is often permitted. For circular frames, weight-bearing is encouraged to promote micromotion at the fracture site, which stimulates secondary bone healing (callus formation). Meticulous pin site care is mandatory to prevent superficial infections
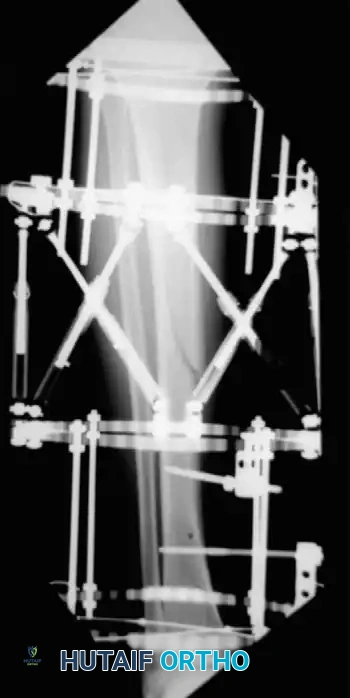
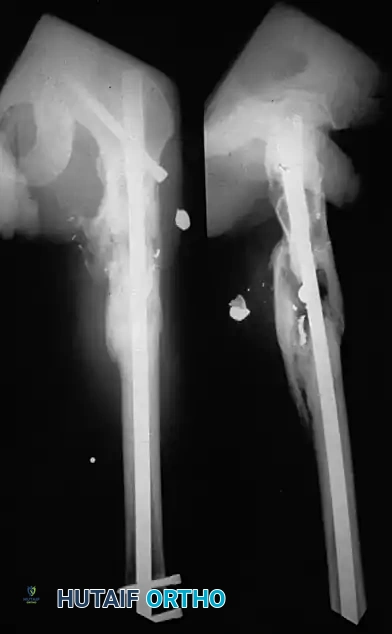
Associated Surgical & Radiographic Imaging

📚 Medical References
- Bahnson DH, Lovell WW: Genu valgum following fractures of the proximal tibial metaphysis in children, Orthop Trans 4:306, 1980.
- Balthazar DA, Pappas AM: Acquired valgus deformity of the tibia in children, J Pediatr Orthop 4:538, 1984.
- Bartlett CS III, Weiner LS, Yang EC: Treatment of type II and type II tibia fractures in children, J Orthop Trauma 11:357, 1997.
- Blasier RD, Barnes CL: Age as a prognostic factor in open tibial fractures in children, Clin Orthop Relat Res 331:261, 1996.
- Briggs TWR, Orr MM, Lightowler CDR: Isolated tibial fractures in children, Injury 23:308, 1992.
- Buckley SL, Smith GR, Sponseller PD, et al: Severe (type III) open fractures of the tibia in children, J Pediatr Orthop 16:627, 1996.
- Court-Brown CM, Byrnes T, McLaughlin G: Intramedullary nailing of tibial diaphyseal fractures in adolescents with open physes, Injury 34:781, 2003.
- Cozen L: Knock knee deformity after fracture of the proximal tibia in children, Orthopedics 1:230, 1959.
- Cramer KE, Limbird TJ, Green NE: Open fractures of the diaphysis of the lower extremity in children: treatment, results, and complications, J Bone Joint Surg 74A:218, 1992.
- Cullen MC, Roy DR, Crawford AH, et al: Open fracture of the tibia in children, J Bone Joint Surg 78A:1039, 1996.
- Engh CA, Robinson RA, Milgram J: Stress fractures in children, J Trauma 10:532, 1970.
- Green NE: Tibial valga caused by asymmetrical overgrowth following a nondisplaced fracture of the proximal tibial metaphysis, J Pediatr Orthop 3:235, 1983.
- Grimard G, Naudie D, Laberge LC, et al: Open fractures of the tibia in children, Clin Orthop Relat Res 332:62, 1996.
- Hansen BA, Greiff J, Bergmann F: Fractures of the tibia in children, Acta Orthop Scand 47:448, 1976.
- Herring JA, Moseley C: Posttraumatic valgus deformity of the tibia, J Pediatr Orthop 1:435, 1981.
- Houghton GR, Rooker GD: The role of the periosteum in the growth of long bones: an experimental study in the rabbit, J Bone Joint Surg 61B:218, 1979.
- Ippolito E, Pentimalli G: Post-traumatic valgus deformity of the knee in proximal tibial metaphyseal fractures in children, Ital J Orthop Traumatol 10:103, 1984.
- Jackson DW, Cozen L: Genu valgum as a complication of proximal tibial metaphyseal fractures in children, J Bone Joint Surg 53A:1571, 1971.
- Jordan SE, Alonso JE, Cook FF: The etiology of valgus angulation after metaphyseal fractures of the tibia in children, J Pediatr Orthop 7:450, 1987.
- Levy AS, Wetzler M, Lewars M, et al: The orthopedic and social outcome of open tibia fractures in children, Orthopedics 20:593, 1997 Mubarak SJ, Hargens AR, Owen CA, et al: The wick catheter technique for measurement of intramuscular pressure, J Bone Joint Surg 58A:1016, 1976.
- Müller I, Muschol M, Mann M, et al: Results of proximal metaphyseal fractures in children, Arch Orthop Trauma Surg 122:331, 2002.
- Navascués JA, González-López JL, López-Valverde S, et al: Premature physeal closure after tibial diaphyseal fractures in adolescents, J Pediatr Orthop 20:193, 2000.
- O’Brien T, Weisman DS, Ronchetti P, et al: Flexible titanium nailing for the treatment of the unstable pediatric tibial fracture, J Pediatr Orthop 24:601, 2004.
- Ogden JA, Ogden DA, Pugh L, et al: Tibia valga after proximal metaphyseal fractures in childhood: a normal biologic response, J Pediatr Orthop 15:489, 1995.
- Pappas AM, Anas P, Toczylowski HM Jr: Asymmetrical arrest of the proximal tibial physis and genu recurvatum deformity, J Bone Joint Surg 66A:575, 1984.
- Pollen AG: Fractures and dislocations in children , Baltimore, 1973, Williams & Wilkins. Rang M: Children’s fractures, 2nd ed, Philadelphia, 1983, Lippincott. Robert M, Khouri N, Carlioz H, et al: Fractures of the proximal tibial metaphysis in children: review of a series of 25 cases, J Pediatr Orthop 7:444, 1987.
- Salter RB, Best T: The pathogenesis and prevention of valgus deformity following fractures of the proximal metaphyseal region of the tibia in children, J Bone Joint Surg 55A:1324, 1973.
- Skak SV, Jensen TT, Poulsen TD: Fracture of the proximal metaphysis of the tibia in children, Injury 18:149, 1987.
- Song KM, Sangeorzan B, Benirschke S, Browne R: Open fractures of the tibia in children, J Pediatr Orthop 16:635, 1996.
- Steel HH, Sandrow RE, Sullivan PD: Complications of tibial osteotomy in children for genu varum or valgum, J Bone Joint Surg 53A:1629, 1971.
- Taylor SL: Tibial overgrowth: a cause of genu valgum, J Bone Joint Surg 45A:659, 1963.
- Weber BG: Fibrous interposition causing valgus deformity after fracture of the upper tibial metaphysis in children, J Bone Joint Surg 59B:290, 1977.
- Weber BG, Brunner C, Freuler F, eds: Treatment of fractures in children and adolescents, New York, 1980, SpringerVerlag. Whitesides TE Jr, Haney TC, Morimoto K, et al: Tissue pressure measurements as a determinant for the need of fasciotomy, Clin Orthop Relat Res 113:43, 1975.
- Yang JP, Letts RM: Isolated fractures of the tibia with intact fi bula in children: a review of 95 patients, J Pediatr Orthop 17:347, 1997.
- Zionts LE, Harcke T, Brooks KM, et al: Posttraumatic tibia valga: a case demonstrating asymmetric activity at the proximal growth plate on technetium bone scan, J Pediatr Orthop 7:458, 1987.
- Distal Tibial and Fibular Epiphyseal Fractures Barmada A, Gaynor T, Mubarak SJ: Premature physeal closure following distal tibia physeal fractures: a new radiographic predictor, J Pediatr Orthop 23:733, 2003.
- Beaty JH, Linton RC: Medial malleolar fracture in a child: a case report, J Bone Joint Surg 70A:1254, 1988.
- Bright RW: Operative correction of partial epiphyseal plate closure by osseous-bridge resection and silicone-rubber implant, J Bone Joint Surg 56A:655, 1974.
- Buckley SL, Smith G, Sponseller PD, et al: Open fractures of the tibia in children, J Bone Joint Surg 72A:1462, 1990.
- Busconi BD, Pappas AM: Chronic, painful ankle instability in skeletally immature athletes: ununited osteochondral fractures of the distal fi bula, Am J Sports Med 24:647, 1996.
- Carothers CO, Crenshaw AH: Clinical signifi cance of a classifi cation of epiphyseal injuries at the ankle, Am J Surg 89:879, 1955.
- Cass JR, Peterson HA: Salter-Harris type IV injuries of the distal tibial epiphyseal growth plate, with emphasis on those involving the medial malleolus, J Bone Joint Surg 65A:1059, 1983.
- Chuinard EG, Peterson RE: Distraction-compression bone-graft arthrodesis of the ankle: a method especially applicable in children, J Bone Joint Surg 45A:1040, 1978.
- Cooperman DR, Spiegel PG, Laros GS: Tibial fractures involving the ankle in children: the so-called triplane epiphyseal fracture, J Bone Joint Surg 60A:1040, 1978.
- Crenshaw AH: Injuries of the distal tibial epiphysis, Clin Orthop Relat Res 41:98, 1965.
- Cutler L, Molloy A, Dhukuram V, et al: Do CT scans aid assessment of distal tibial physeal fractures? J Bone Joint Surg 86B:239, 2004.
- Denton JR, Fischer SJ: The medial triplane fracture: report of an unusual injury, J Trauma 21:991, 1981.
- Dias LS, Giegerich CR: Fractures of the distal tibial epiphysis in adolescence, J Bone Joint Surg 65A:438, 1983.
- Feldman DS, Otsuka NY, Hedden DM: Extra-articular triplane fracture of the distal tibial epiphysis, J Pediatr Orthop 15:479, 1995.
- Hope PG, Cole WG: Open fractures of the tibia in children, J Bone Joint Surg 74B:546, 1992.
- Horn DB, Crisci K, Krug M, et al: Radiologic evaluation of juvenile Tillaux fractures of the distal tibia. J Pediatr Orthop 21:162, 2001.
- Hynes D, O’Brien T: Growth disturbance lines after injury of the distal tibial physis: their signifi cance in prognosis, J Bone Joint Surg 70B:231, 1988.
- Kling TF, Bright RW, Hensinger RM: Distal tibial physeal fractures in children that may require open reduction, J Bone Joint Surg 66A:647, 1984.
- Langenskiöld A: An operation for partial closure of an epiphysial plate in children, and its experimental basis, J Bone Joint Surg 57B:325, 1975.
- Leibner ED, Simanovsky N, Abu-Sneinah K, et al: Fractures of the lateral process of the talus in children. J Pediatr Orthop 10B:68, 2001.
- Letts M, Davidson D, McCaffrey M: The adolescent pilon fracture: management and outcome, J Pediatr Orthop 21:20, 2001.
- Letts RM: Hidden adolescent ankle fracture, J Pediatr Orthop 2:161, 1982.
- Lintecum N, Blasier RD: Direct reduction and indirect fi xation of distal tibial physeal fractures: a report of a technique, J Pediatr Orthop 16:107, 1996.
- Marmor L: An unusual fracture of the tibial epiphysis, Clin Orthop Relat Res 73:132, 1970.
- Ogden JA, Lee J: Accessory ossifi cation patterns and injuries of the malleoli, J Pediatr Orthop 10:306, 1990.
- Peterson HA: Operative correction of post-fracture arrest of the epiphyseal plate: case report with a ten-year follow-up, J Bone Joint Surg 62A:1018, 1980.
- Rapariz JM, Ocete G, Gonzalez-Herranz P, et al: Distal tibial triplane fractures: long-term follow-up, J Pediatr Orthop 16:113, 1996.
- Ruedi TP, Allgower M: The operative treatment of intra-articular fractures of the lower end of the tibia, Clin Orthop 138:105, 1979.
- Schlesinger I, Wedge JH: Percutaneous reduction and fi xation of displaced juvenile Tillaux fractures: a new surgical technique, J Pediatr Orthop 13:389, 1993.
- Seifert J, Matthes G, Hinz P, et al: Role of magnetic resonance imaging in the diagnosis of distal tibia fractures in adolescents, J Pediatr Orthop 23:727, 2003.
- Shannak AO: Tibial fractures in children: follow-up study, J Pediatr Orthop 8:306, 1988.
- Shin AY, Moran ME, Wenger DR: Intramalleolar triplane fractures of the distal tibial epiphysis, J Pediatr Orthop 17:352, 1997.
- Spiegel PG, Cooperman DR, Laros GS: Epiphyseal fractures of the distal ends of the tibia and fi bula: a retrospective study of 237 cases in children, J Bone Joint Surg 60A:1046, 1978.
- Stanitski CL, Micheli LJ: Observations on symptomatic medial malleolar ossifi cation centers, J Pediatr Orthop 13:164, 1993.
- Weber BG, Sussenbach F:
You Might Also Like


