Operative Management of Pes Planus: A Comprehensive Surgical Guide
Key Takeaway
Pes planus is a complex multiplanar deformity characterized by the loss of the medial longitudinal arch, hindfoot valgus, and forefoot supination. While asymptomatic flexible flatfeet rarely require intervention, symptomatic cases failing conservative management necessitate precise surgical correction. This guide details evidence-based operative strategies, including medial column stabilization, lateral column lengthening, and calcaneal displacement osteotomies, to restore foot biomechanics and alleviate disabling pain.
Introduction to Pes Planus
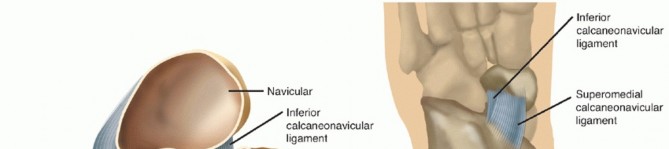
Pes planus (flatfoot) by convention refers to the loss of the normal medial longitudinal arch. However, it is fundamentally a complex, multiplanar deformity. The anatomical abnormalities present include a valgus posture of the heel; mild subluxation of the subtalar joint, in which the head of the talus tilts medially and plantarward (appearing foreshortened on the standing dorsoplantar radiograph); eversion of the calcaneus at the subtalar joint; lateral angulation (abduction) at the midtarsal joint (talonavicular and calcaneocuboid joints); and supination of the forefoot relative to the hindfoot, which places the first ray plantigrade.
The Achilles tendon is frequently shortened, accentuating the valgus of the hindfoot and acting as a deforming force that must be addressed during surgical reconstruction. Pes planus in children and adults is usually flexible; upon non–weight-bearing examination, a normal-appearing arch is restored. If an acceptable medial longitudinal arch does not appear with non–weight-bearing, the pes planus is termed fixed, or rigid. In fixed or semirigid pes planus, bony and soft-tissue structural changes exist that do not lend themselves to treatment by simply altering footwear.
Clinical and Radiographic Evaluation
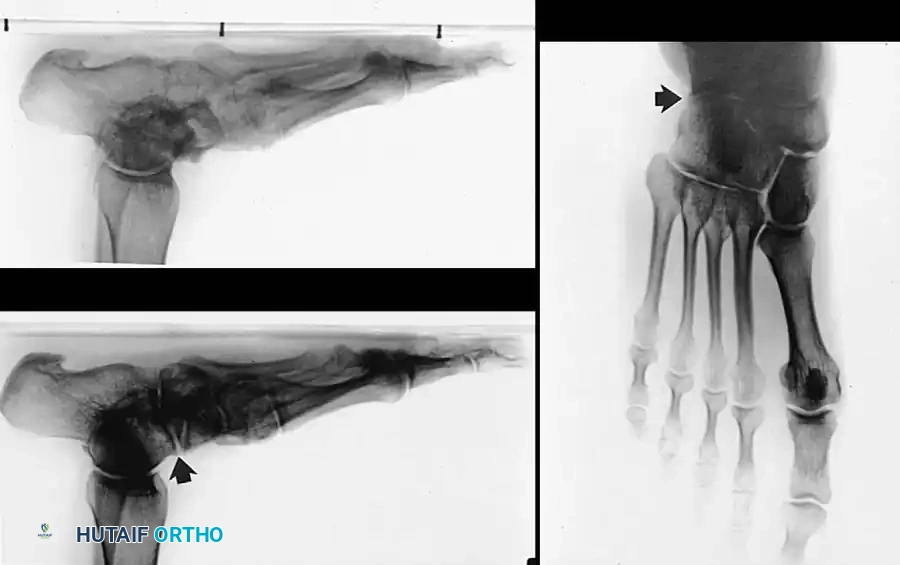
Standing radiographs in the anteroposterior (AP) and lateral planes, alongside nonstanding lateral oblique views, are mandatory to evaluate the severity of the deformity.
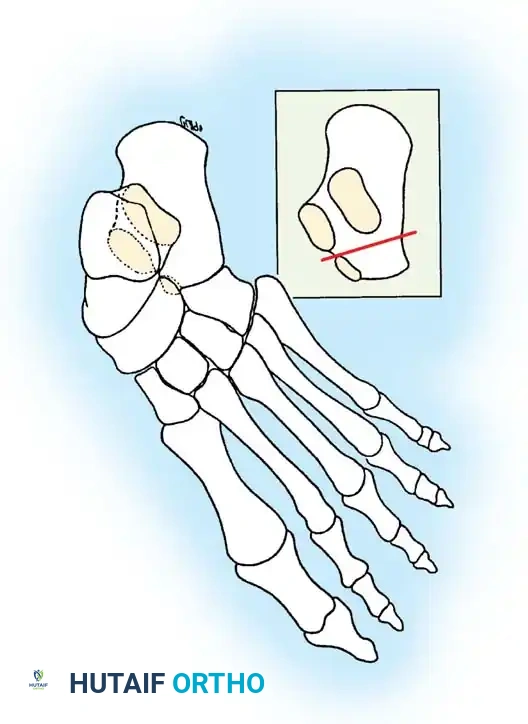
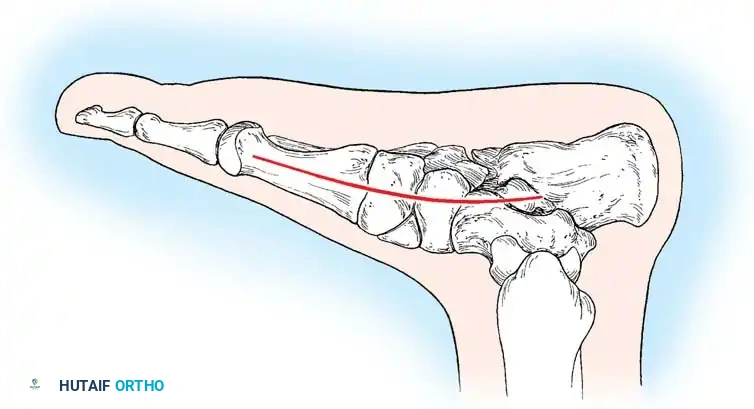
On the dorsoplantar (AP) view, talocalcaneal divergence (Kite's angle) is increased, and talonavicular uncoverage is evident. On the lateral view, plantar flexion of the talus disrupts Meary’s line (the talar-first metatarsal axis). Lateur et al. (1994) described the “C” sign on lateral radiographs of the ankle as suggestive of a talocalcaneal subtalar coalition. While highly useful, Brown et al. later found the “C” sign to be more specific for severe pes planus than for subtalar coalition alone.
Additionally, a structural “sag” at the talonavicular, naviculocuneiform, or tarsometatarsal joints can be assessed. The oblique view in a 9- to 14-year-old child is critical, as it may reveal a calcaneonavicular bony bar or suggest a synchondrosis.
Evidence-Based Nonoperative Management
Nowhere in the care of the foot is the literature more confusing, contradictory, and anecdotal than in the treatment of flexible pes planus. Recommendations historically ranged from aggressive surgical correction in toddlers to absolute therapeutic nihilism.
For a child from walking age to 3 years with flexible pes planus, encumbering the parents and patient with expensive shoe modifications is not warranted unless there is a strong family history of flatfeet persisting into adulthood. The arch may not develop fully until the child is 7 to 10 years old. Approximately 15% to 20% of adults have some degree of flexible pes planus, and the vast majority remain asymptomatic.
Clinical Pearl: There are no convincing data that shoe modifications and inserts appreciably alter the final structural development of the foot arch. Wenger et al. concluded that corrective shoes and inserts worn for 3 years did not influence the course of flexible pes planus in children.
Hogan and Staheli evaluated physically active adults and found no relationship between arch configuration and pain scores, suggesting that in a civilian population, flexible pes planus is not a source of disability. Michelson et al. (2002) evaluated athletes (42% in contact sports) and found pes planus did not predispose them to lower extremity injury, advising against routine prophylactic orthoses. Based on these robust findings, asymptomatic flexible pes planus in children should not be treated.
When a child is symptomatic, an arch support is placed in a leather shoe with a firm heel counter, an extended medial counter, a steel shank, a Thomas heel, and a medial heel wedge. Custom orthoses (leather, cork, or polypropylene) are reserved for severe, symptomatic flexible pes planus (3 to 9 years old) with marked heel valgus, forefoot abduction, and a prominent medial talar head, primarily for comfort.
Surgical Indications and Principles
What is the origin of pain in symptomatic pes planus? Malicky et al. studied simulated weight-bearing CT scans in adult patients with symptomatic pes planus. They found that sinus tarsi impingement—evidenced by cystic changes, sclerosis, and abutment of the lateral process of the talus on the floor of the sinus tarsi—was present in 92% of symptomatic patients. Calcaneofibular impingement was present in 66%.
Surgical intervention is reserved for patients with disabling pain who have exhausted conservative management. We agree philosophically with Crego and Ford:
1. Surgery should never be performed for cosmetic reasons alone.
2. The surgeon, patient, and parents must be willing to exchange a loss of hindfoot inversion/eversion for the relief of pain and disability.
3. Arthrodeses for relieving painful pes planus are most successful when the subtalar joint is included, though joint-sparing osteotomies have revolutionized modern treatment.
Modern Surgical Paradigm
In recent years, the paradigm has shifted away from isolated medial column arthrodesis toward peritalar osteotomies. We have been highly impressed with the ability to correct deformity using lateral column lengthening (anterior calcaneal osteotomy) and posterior calcaneal displacement osteotomies, combined with posterior tibial tendon advancement or transfer (FDL/FHL).
Calcaneal osteotomies are biomechanically sound:
* Transverse plane: Raises the floor of the sinus tarsi (Chambers; Miller).
* Oblique plane (Tuberosity): Shifts the posterior fragment medially to improve the weight-bearing axis (Koutsogiannis).
* Coronal plane (Anterior): Lengthens the lateral column, pushing the navicular and forefoot medially to correct abduction (Evans; Mosca).
Surgical Warning: Calcaneal osteotomy rarely corrects the entire deformity in older patients with long-standing posterior tibial tendon insufficiency. Fixed supination (forefoot varus) at the midtarsal joint will not be corrected by calcaneal lengthening and must be addressed simultaneously (e.g., with a Cotton osteotomy).
Operative Techniques
1. Durham Plasty for Pes Planus (Medial Column Stabilization)
The Durham plasty combines the advancement of the posterior tibial tendon and an osteoperiosteal flap with arthrodesis of the navicular–first cuneiform joint. Caldwell and Coleman reported excellent or good results in over 90% of patients, defined by a restored weight-bearing longitudinal arch and an asymptomatic foot.
Surgical Technique 79-1:
- Incision and Exposure: Begin the incision 2 cm inferior to the medial malleolus, extend it in a gentle curve distally 1 cm dorsal to the navicular tuberosity, and slope plantarward to end 2 cm distal to the first metatarsal–first cuneiform joint.
- Gently undermine the skin and superficial fascia 7 to 10 mm dorsally and plantarward to expose the medial aspect of the midfoot from the sustentaculum tali to the anterior tibial tendon insertion.
- Hemostasis and Nerve Protection: Carefully coagulate or tie the superficial plantar communicating veins from the saphenous system. Protect the terminal branches of the saphenous nerve.
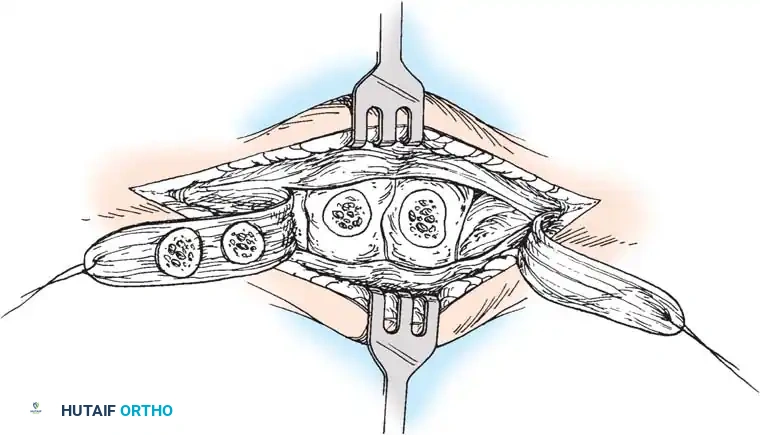
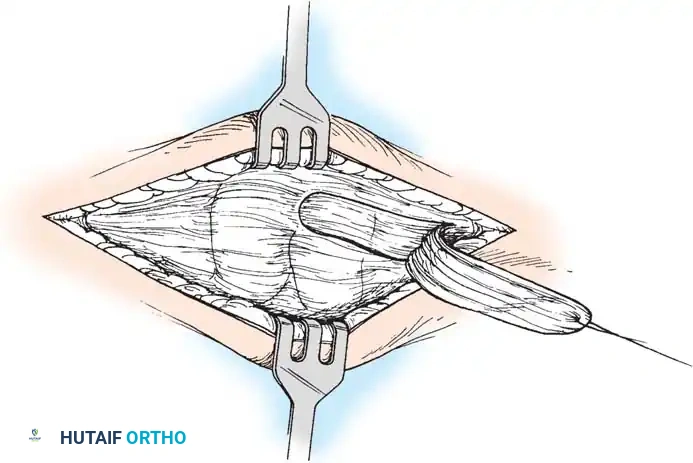
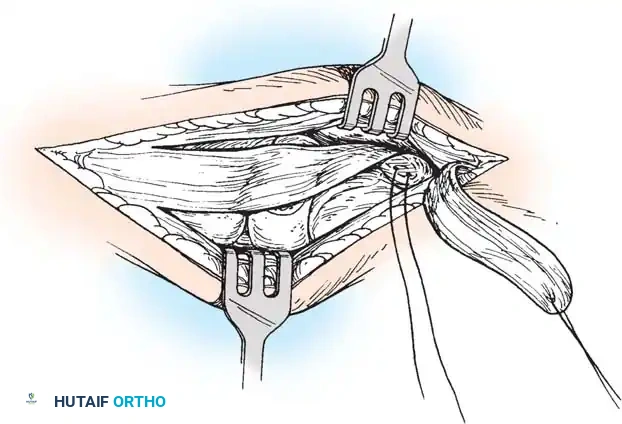
- Flap Creation: Incise the master knot of Henry and identify the posterior tibial tendon. Create a robust osteoperiosteal flap based distally, reflecting the tendon and periosteum to expose the naviculocuneiform joint.
- Joint Preparation: Denude the articular cartilage of the navicular and medial cuneiform down to bleeding subchondral bone using a curette and osteotome. Ensure the surfaces are flat and congruent when the arch is manually reduced.
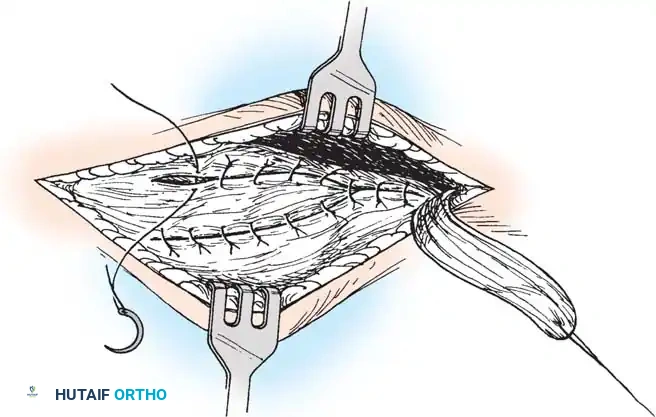
- Arthrodesis and Advancement: Plantarflex the first ray and invert the midfoot to close the arthrodesis site. Fix the joint using crossed partially threaded cancellous screws or a medial column plate. Advance the posterior tibial tendon flap under tension and suture it securely to the periosteum of the medial cuneiform and first metatarsal base.

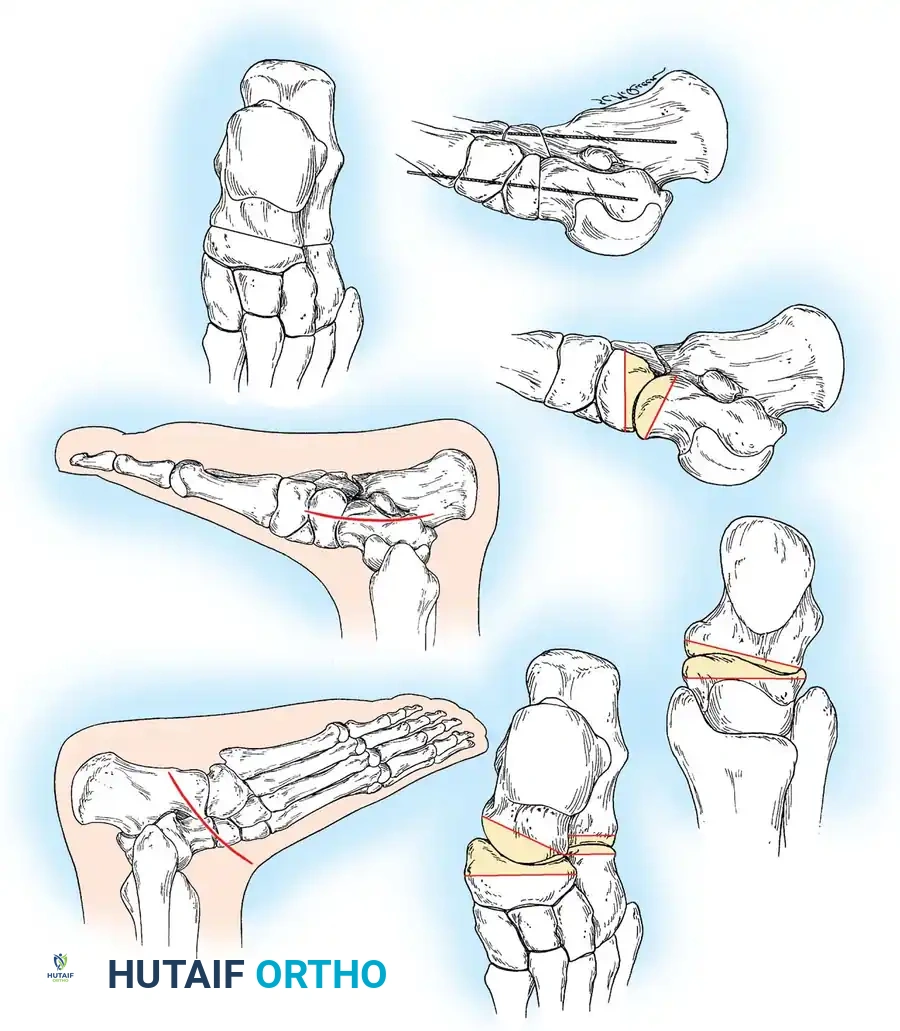
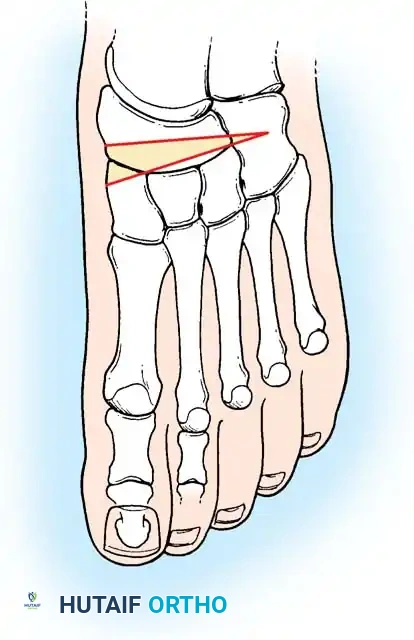
2. Lateral Column Lengthening (Anterior Calcaneal Osteotomy)
Described by Dillwyn Evans and modified by Mosca, this procedure corrects midfoot abduction and restores the talonavicular joint congruency by lengthening the lateral column.
Surgical Steps:
* Approach: Make an oblique incision over the sinus tarsi, extending toward the calcaneocuboid (CC) joint. Identify and protect the sural nerve and peroneal tendons.
* Exposure: Reflect the extensor digitorum brevis (EDB) muscle belly distally to expose the anterior calcaneus and the CC joint.
* Osteotomy: Perform a transverse osteotomy of the anterior calcaneus approximately 1.5 cm proximal to the CC joint line. Use an oscillating saw, taking care not to breach the medial calcaneal cortex entirely, leaving a periosteal hinge.
- Distraction: Insert a lamina spreader into the osteotomy. Gently distract the site while observing the medial longitudinal arch. The forefoot will adduct, and the talonavicular joint will reduce.
- Grafting: Harvest a tricortical iliac crest bone graft (or use structural allograft) tailored to the exact dimensions of the distracted gap (typically 8 to 12 mm). Tamp the graft into place.
- Fixation: While the graft is often stable under compression, supplemental fixation with a cervical plate or a single compression screw is highly recommended to prevent graft extrusion or nonunion.
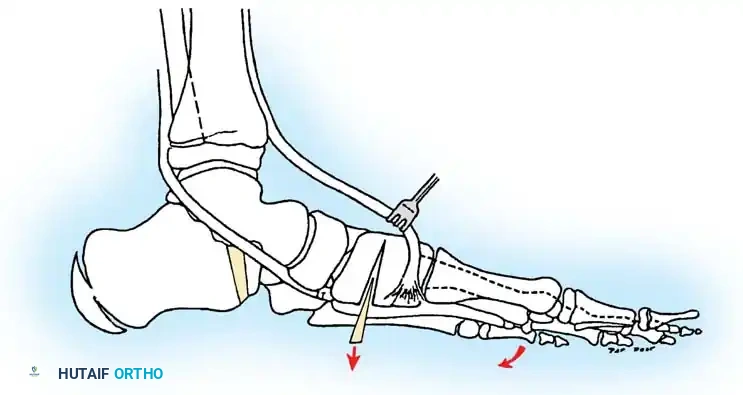
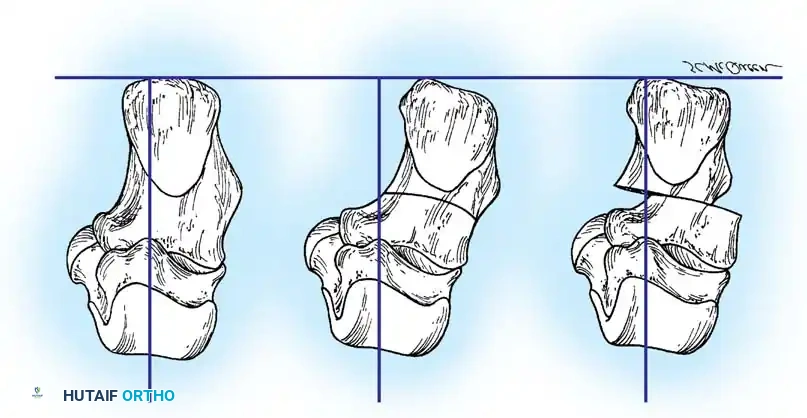
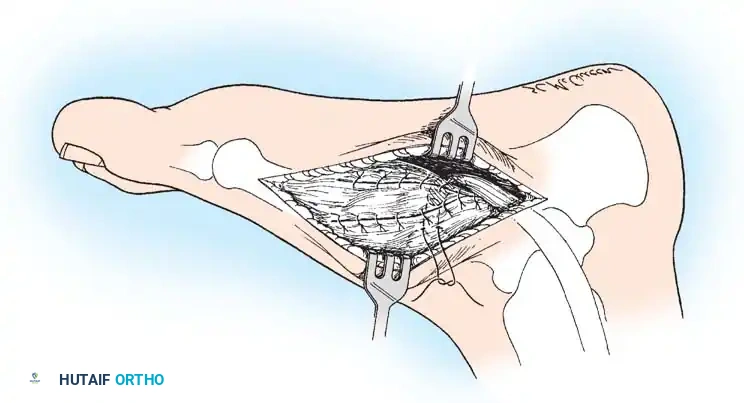
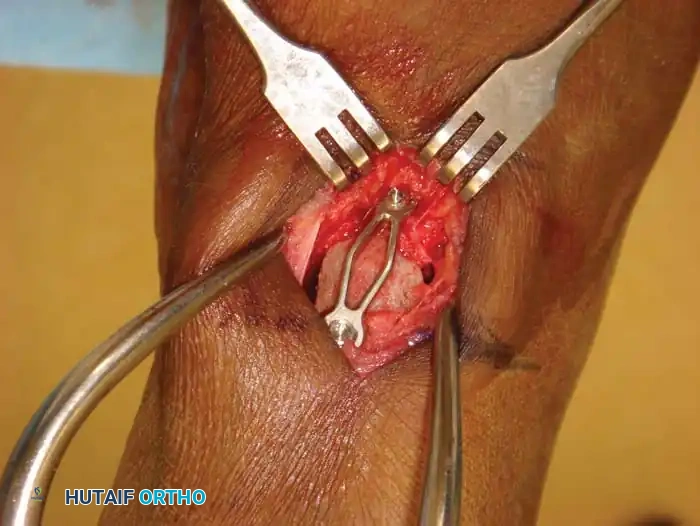
3. Posterior Calcaneal Displacement Osteotomy (Koutsogiannis)
This extra-articular osteotomy shifts the mechanical axis of the hindfoot medially, converting the Achilles tendon from an evertor to an invertor of the heel.
Surgical Steps:
* Approach: Make an oblique lateral incision posterior to the peroneal tendons, avoiding the sural nerve.
* Osteotomy: Use an oscillating saw to make an oblique cut through the calcaneal tuberosity, angled at 45 degrees to the plantar surface.
* Translation: Free the medial periosteal attachments slightly to allow mobility. Translate the posterior tuberosity fragment medially by 10 to 15 mm (approximately 50% of the calcaneal width).
- Fixation: Provisionally pin the fragment with a Kirschner wire. Confirm the medial shift and overall hindfoot alignment clinically and fluoroscopically. Fix the osteotomy rigidly with one or two large-fragment (6.5 mm or 7.3 mm) cannulated headless or headed compression screws directed from the posterior heel into the anterior calcaneal body.
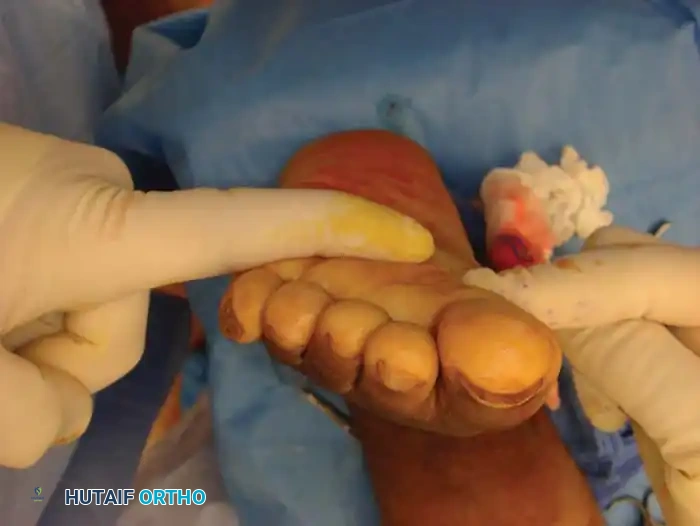
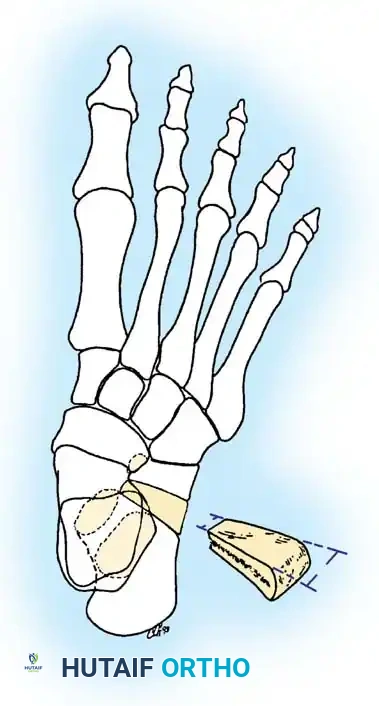
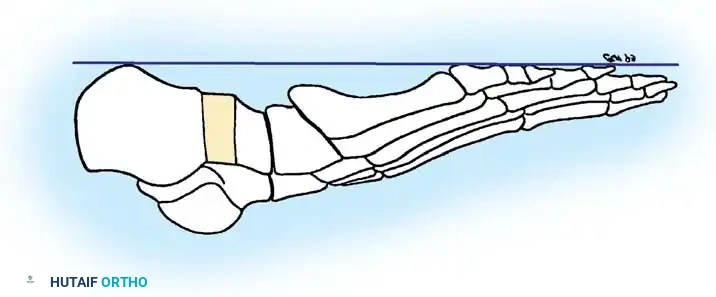
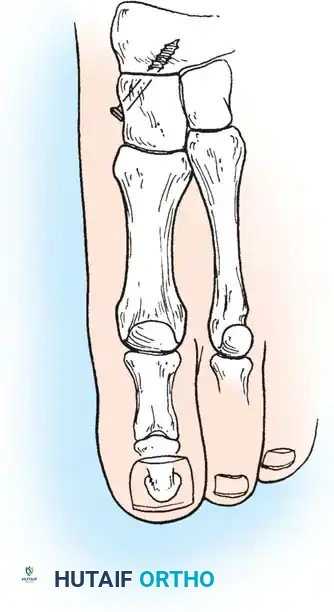
4. Plantar Flexion Osteotomy of the Medial Cuneiform (Cotton Procedure)
Following hindfoot correction (via calcaneal osteotomy), the forefoot may remain in fixed supination (forefoot varus). The Cotton osteotomy plantarflexes the first ray to restore a plantigrade tripod foot.
Surgical Steps:
* Approach: Make a dorsal longitudinal incision over the medial cuneiform. Protect the medial branch of the superficial peroneal nerve and the extensor hallucis longus tendon.
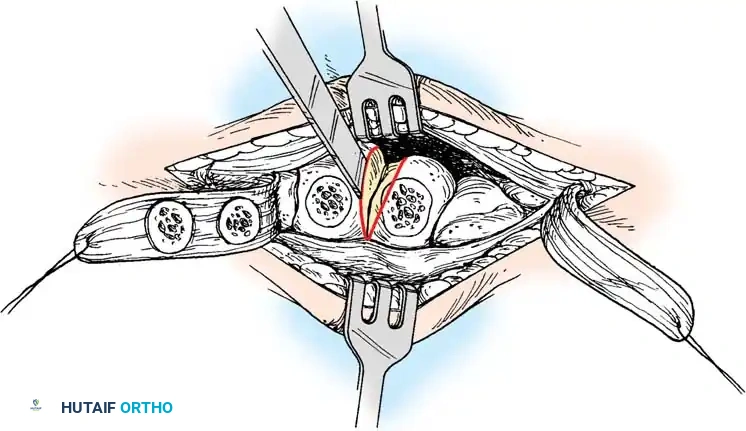
* Osteotomy: Perform a dorsal opening-wedge osteotomy of the medial cuneiform using a sagittal saw. Leave the plantar cortex intact to act as a hinge.
* Correction: Open the osteotomy dorsally with an osteotome until the first metatarsal head is brought down to the level of the lesser metatarsals (plantigrade).

- Grafting and Fixation: Insert a structural wedge graft (autograft or allograft) into the dorsal defect. Fixation is achieved with a dorsal spanning plate or staples.
5. Triple Arthrodesis
For rigid pes planus, severe arthritic changes, or failed previous reconstructions, a triple arthrodesis (fusion of the subtalar, talonavicular, and calcaneocuboid joints) remains the gold standard salvage procedure.

Surgical Steps:
* Exposure: Utilize a standard two-incision approach (lateral Ollier incision for the subtalar and CC joints; medial incision for the talonavicular joint).
* Joint Preparation: Meticulously denude all cartilage from the three joints. Use a high-speed burr and osteotomes to feather the subchondral bone, ensuring maximal bleeding surface area.

- Deformity Correction: The key to a successful triple arthrodesis in pes planus is the restoration of alignment. The talonavicular joint must be reduced (correcting abduction), and the subtalar joint must be brought out of valgus into 5 degrees of physiologic valgus.
- Fixation: Fix the subtalar joint first with a large cannulated screw from the calcaneal tuberosity into the talar dome. Fix the talonavicular joint with two crossed screws or a plate. Finally, fix the calcaneocuboid joint with staples or screws.
Postoperative Protocol
Regardless of the specific osteotomy or arthrodesis performed, strict adherence to postoperative immobilization is critical for success.
- Phase I (0-2 Weeks): The patient is placed in a bulky Jones splint and remains strictly non-weight-bearing. Elevation is paramount to control edema and prevent wound breakdown.
- Phase II (2-6 Weeks): Sutures are removed. The patient is transitioned to a short-leg cast or rigid CAM boot, remaining non-weight-bearing.
- Phase III (6-12 Weeks): Radiographs are obtained to confirm graft incorporation and osteotomy/arthrodesis healing.
If radiographic healing is evident, the patient begins progressive weight-bearing in a CAM boot, advancing to a supportive shoe with a custom orthosis by 10 to 12 weeks. Physical therapy focuses on restoring ankle and forefoot range of motion, peroneal and posterior tibial tendon strengthening, and proprioceptive retraining. Full athletic activity is generally restricted until 6 to 9 months postoperatively.
📚 Medical References
- pes planus, Foot Ankle 4:274, 1984.
- Aronson J, Puskarich CL: Deformity and disability from treated clubfoot, J Pediatr Orthop 10:109, 1990.
- Atar D, Grant AD, Silver L, et al: The use of a tissue expander in clubfoot surgery: a case report and review, J Bone Joint Surg 72B:574, 1990.
- Bensahel H, Catterall A, Dimeglio A: Practical applications in idiopathic clubfoot: a retrospective multicentric study in EPOS, J Pediatr Orthop 10:186, 1990.
- Bényi P: A modifi ed Lambrinudi operation for drop foot, J Bone Joint Surg 42B:333, 1960.
- Bor N, Herzenberg JE, Frick SL: Ponseti management of clubfoot in older infants, Clin Orthop Relat Res 444:224, 2006.
- Bradish CF, Noor S: The Ilizarov method in the management of relapsed club feet, J Bone Joint Surg 82B:387, 2000.
- Bradish CF, Tan S: Residual bone cysts after Ilizarov treatment of relapsed clubfoot, J Pediatr Orthop 21:218, 2001.
- Brougham DI, Nicol RO: Use of the Cincinnati incision in congenital talipes equinovarus, J Pediatr Orthop 8:696, 1988.
- Carroll NC: Congenital clubfoot: pathoanatomy and treatment, Instr Course Lect 36:117, 1987.
- Carroll NC: Clubfoot, in Morrissy RT (ed): Pediatric Orthopaedics , 3rd ed, Philadelphia, JB Lippincott, 1990, vol. 2, pp. 927–956. Carroll NC: Controversies in the surgical management of clubfoot, Instr Course Lect 45:331, 1996.
- Catterall A: A method of assessment of the clubfoot deformity, Clin Orthop Relat Res 264:48, 1991.
- Chang CH, Huang SC: Clubfoot deformity in congenital constriction band syndrome: manifestations and treatment, J Formos Med Assoc 97:328, 1998.
- Changulani M, Garg N, Bruce CE: Neurovascular complications following percutaneous tendoachilles tenotomy for congenital idiopathic clubfoot, Arch Orthop Trauma Surg 10:2007.
- Cooper DM, Deitz FR: Treatment of idiopathic clubfoot: a thirty-year follow-up note, J Bone Joint Surg 77A:1477, 1995.
- Crawford AH, Gupta AK: Clubfoot controversies: complications and causes for failure, Instr Course Lect 45:339, 1996.
- Crawford AH, Marxen JL, Osterfeld DL: The Cincinnati incision: a comprehensive approach for surgical procedures of the foot and ankle in childhood, J Bone Joint Surg 64A:1355, 1982.
- Cummings J, Lovell WW: Current concepts: operative treatment of congenital idiopathic clubfoot, J Bone Joint Surg 70A:1108, 1988.
- Cummings RJ, Bashore CJ, Bookout CB, et al: Avascular necrosis of the talus after McKay clubfoot release for idiopathic congenital clubfoot, J Pediatr Orthop 21:221, 2001.
- DePuy J, Drennan JC: Correction of idiopathic clubfoot: a comparison of results of early versus delayed posteromedial release, J Pediatr Orthop 9:44, 1989.
- Dillwyn-Evans D: Relapsed clubfoot, J Bone Joint Surg 43B:722, 1961.
- Dimeglio A, Bensahel H, Souschet P, et al: Classifi cation of clubfoot, J Pediatr Orthop B 4:129, 1995.
- Dobbs MB, Gordon JE, Walton T, Schoenecker PL: Bleeding complications following percutaneous tendoachilles tenotomy in the treatment of deformity, J Pediatr Orthop 24:353, 2004.
- Dobbs MB, Rudzki JR, Purcell DB, et al: Factors predictive of outcome after use of the Ponseti method for the treatment of idiopathic clubfeet, J Bone Joint Surg 86A:22, 2004.
- Dunn HK, Samuelson KM: Flat-top talus: a long-term report of twenty clubfeet, J Bone Joint Surg 56A:57, 1974.
- Dwyer FC: Osteotomy of the calcaneum for pes cavus, J Bone Joint Surg 41B:80, 1959.
- Dwyer FC: The treatment of relapsed club foot by the insertion of a wedge into the calcaneum, J Bone Joint Surg 45B:67, 1963.
- Dwyer FC: The present status of the problem of pes cavus, Clin Orthop Relat Res 106:254, 1975.
- Ezra E, Hayek S, Gilai AN, et al: Tibialis anterior
You Might Also Like