Cavovarus Foot Deformity: Etiology, Biomechanics, and Surgical Reconstruction
Key Takeaway
Pes cavus, or cavovarus foot deformity, is a complex structural pathology characterized by an abnormally elevated medial longitudinal arch, hindfoot varus, and claw toes. Historically deemed idiopathic, up to 90% of cases are now traced to neuromuscular or traumatic etiologies, most notably Charcot-Marie-Tooth disease. Successful surgical correction requires a deep understanding of extrinsic-intrinsic muscle imbalances and meticulous stepwise reconstruction to restore a plantigrade, stable foot.
INTRODUCTION TO CAVOVARUS DEFORMITY
The cavovarus foot presents one of the most challenging reconstructive paradigms in orthopedic surgery. What begins as a mildly elevated medial longitudinal arch can relentlessly progress into a rigid equinovarus deformity with fixed claw toes. Understanding the exact etiology and the underlying biomechanical cascade is paramount. In most patients, this progression does not occur spontaneously; rather, the evolution of the deformity is strictly dictated by its underlying cause.
Historically, the orthopedic consensus held that in 80% of patients, the cause of a cavus deformity was unknown (idiopathic). Today, the diagnostic landscape has shifted dramatically. With the advent of detailed physical examinations supplemented by electromyography (EMG), nerve conduction velocities (NCV), advanced magnetic resonance imaging (MRI), myelography, arteriography, and sophisticated genetic sequencing, a definitive etiology can be identified in 80% to 90% of patients.
ETIOLOGY AND PATHOGENESIS
In skeletally mature patients, the etiology of pes cavus is most frequently rooted in neuromuscular disease or severe trauma. Recognizing the specific driver of the deformity dictates not only the surgical timing but the choice of soft tissue and bony procedures required for durable correction.
Neuromuscular Etiologies
The most common neuromuscular diseases causing pes cavus in skeletally mature feet are Charcot-Marie-Tooth (CMT) disease and residual poliomyelitis.

Marked forefoot equinus and resulting dorsal prominence of the tarsus in a patient with residual poliomyelitis deformity.
Patients with spinal dysraphism, cerebral palsy, primary cerebellar disease, Friedreich’s ataxia, arthrogryposis, or severe clubfeet may also develop cavus deformities. However, these conditions are usually recognized and treated well before skeletal maturity. In progressive neuromuscular diseases like CMT, the deformity is driven by a highly specific pattern of muscle denervation and preservation.
Traumatic Etiologies
Traumatic cavus deformity is frequently the sequela of a deep posterior compartment syndrome following a fracture of the tibia or fibula, or it may result from the malunion of midfoot fractures or fracture-dislocations (e.g., talar neck fractures).
The clinical presentation of post-traumatic cavus may be delayed. It often does not appear for several months following the initial local ischemia and muscle fibrosis of the deep posterior compartment. Alternatively, it may present initially as a mild, barely perceptible abnormality that progresses relentlessly to a rigid cavovarus–claw toe deformity.
Surgical Warning: Whether the fibrosis and contracture of the tibialis posterior, flexor digitorum longus (FDL), and flexor hallucis longus (FHL) are caused by ischemia from arterial disruption, elevated compartment pressures with myonecrosis, or direct laceration of muscle-tendon units, the end result is a devastating combination of deformities. This ranges from mild clawing of the toes (a checkrein deformity caused by adherence of tendons around a fibrotic area of fracture healing) to a rigid, unyielding cavovarus foot.
Idiopathic Etiologies
Despite advanced diagnostics, in a small subset of patients with symptomatic cavus deformities, no definite cause is discovered. These are classified as true idiopathic pes cavus.


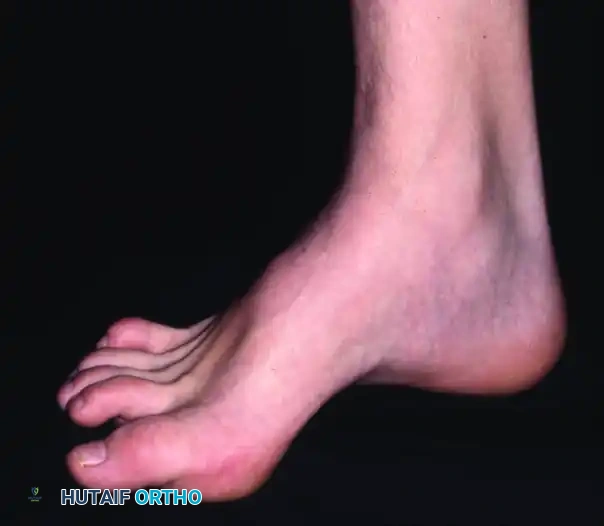
Fifteen-year-old boy with “idiopathic” pes cavus after extensive neurological evaluation. Note the prominent medial arch and hindfoot varus.
BIOMECHANICS AND PATHOANATOMY
The exact role of the intrinsic muscles in the production of the cavus deformity has been historically debated, especially in traumatic pes cavus. However, in patients with neuromuscular diseases and idiopathic deformities, the underlying pathological mechanism is universally accepted as an imbalance between the extrinsic and intrinsic musculature.
The Extrinsic-Intrinsic Imbalance
The intrinsic muscles in the plantar aspect of the foot generally flex the metatarsophalangeal (MTP) joints and extend the interphalangeal (IP) joints. Any weakness of these muscles—whether absolute or relative to their antagonists—disrupts the intrinsic-extrinsic muscle balance, functioning much like an intrinsic-minus (claw) hand.
Mild cavus deformity and clawing of toes in a patient in whom no cause could be found.
The Charcot-Marie-Tooth (CMT) Model
In progressive neuromuscular diseases such as CMT, the pathoanatomy follows a predictable sequence:
1. First Ray Plantarflexion: The forefoot assumes an equinus position with a rigidly plantarflexed and pronated first metatarsal. This is primarily caused by the relative sparing of the peroneus longus muscle, which overpowers the weakened tibialis anterior.
2. Forefoot Pronation: The plantarflexed first ray causes fixed pronation of the forefoot (forefoot valgus).
3. Hindfoot Varus: With peroneus brevis weakness, the strong tibialis posterior exacerbates the forefoot equinus and inverts the foot at the midtarsal joints.
4. Plantar Fascia Contracture: As the arch elevates, the plantar fascia undergoes adaptive shortening and contracture.

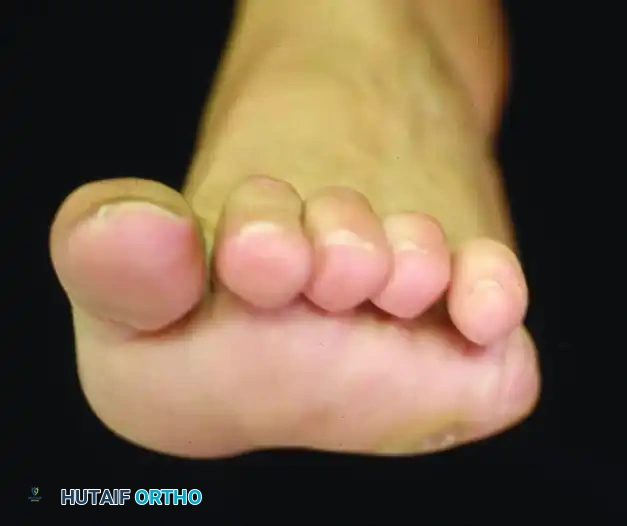
Forefoot is pronated in relation to the hindfoot during weight bearing; note the severe clawing of the toes.
Shortening of the medial column of the foot, a hallmark of chronic cavovarus deformity.
Forefoot-Driven Hindfoot Deformity
That the hindfoot deformity follows forefoot equinus is supported by the landmark observations of Paulos et al. The rigid, plantarflexed first ray acts as a kickstand. When the patient bears weight, the first metatarsal strikes the ground prematurely, forcing the heel into a compensatory varus position to allow the lateral border of the foot to contact the floor. Over time, this flexible compensatory varus becomes a rigid, fixed structural deformity.
CLINICAL EVALUATION
A meticulous clinical evaluation is required to formulate a surgical plan. The most common symptom prompting orthopedic consultation is not the deformity itself, but the painful calluses that develop beneath the metatarsal heads due to forefoot equinus and clawing.

Calluses beneath the metatarsal heads are the most common symptom prompting orthopedic consultation.
Neurological Assessment
Electromyography and nerve conduction velocity studies are critical. They help diagnose neurological abnormalities in the intrinsic muscles, especially if a sensory deficit to touch and pinprick over the pulps of one or more toes is present, or if tenderness is noted beneath the flexor retinaculum along the course of the tibial nerve.
The Coleman Block Test
The Coleman and Chestnut block test is the gold standard for determining the hindfoot-forefoot relationship in pes cavus.
* Technique: The patient stands with the heel and lateral border of the foot on a 1-inch wooden block, allowing the plantarflexed first metatarsal to hang freely off the medial edge.
* Interpretation: If the hindfoot varus corrects to neutral or valgus, the hindfoot is flexible, and the deformity is entirely forefoot-driven. If the hindfoot remains in varus, the deformity is fixed, necessitating a calcaneal osteotomy or hindfoot arthrodesis.
Clinical Pearl: Other than the underlying cause and the age of the patient, the flexibility of the anatomical components of a cavus foot is the single most important factor for determining appropriate surgical treatment.
SURGICAL INDICATIONS AND DECISION MAKING
Surgical intervention is indicated for patients with progressive deformity, intractable plantar keratoses, recurrent lateral ankle instability, or failure of conservative management (e.g., custom orthotics, AFOs).
The surgical algorithm is dictated by the flexibility of the deformity:
* Flexible Hindfoot: Soft tissue releases (plantar fasciotomy), first metatarsal dorsiflexion osteotomy, and tendon transfers.
* Rigid Hindfoot: Addition of a lateralizing calcaneal osteotomy.
* Rigid Degenerative Foot: Triple arthrodesis (salvage procedure).
PREOPERATIVE PLANNING AND POSITIONING
- Anesthesia: General anesthesia combined with a regional popliteal block for postoperative pain control.
- Positioning: The patient is placed in the lateral decubitus position or supine with a large ipsilateral hip bump to allow internal rotation of the leg, granting access to both the medial and lateral aspects of the foot.
- Tourniquet: A thigh or calf tourniquet is applied and inflated to 250-300 mm Hg after exsanguination.
SURGICAL APPROACHES AND TECHNIQUES: STEP-BY-STEP
Reconstruction of the cavovarus foot is an à la carte procedure. The surgeon must systematically address the plantar fascia, the bony architecture of the forefoot and hindfoot, and the dynamic muscle imbalances.
Step 1: Plantar Fascia Release (Steindler Stripping)
The first step in correcting a cavus foot is releasing the contracted plantar fascia to unlock the medial column.
1. Make a 3-cm longitudinal incision on the medial aspect of the heel, just superior to the plantar fat pad.
2. Identify the medial calcaneal nerve and retract it superiorly.
3. Expose the origin of the plantar fascia on the medial calcaneal tuberosity.
4. Release the plantar fascia and the origins of the abductor hallucis, flexor digitorum brevis, and abductor digiti minimi directly off the bone.
5. Dorsiflex the foot to ensure complete release of the medial column.
Step 2: First Metatarsal Dorsiflexion Osteotomy
If the Coleman block test demonstrates a forefoot-driven deformity, the plantarflexed first ray must be elevated.
1. Make a dorsal longitudinal incision over the proximal first metatarsal.
2. Protect the extensor hallucis longus (EHL) tendon and the medial branch of the deep peroneal nerve.
3. Perform a dorsal closing-wedge osteotomy approximately 1.5 cm distal to the first tarsometatarsal (TMT) joint.
4. Remove a 2- to 4-mm wedge of bone based dorsally.
5. Close the osteotomy by dorsiflexing the distal fragment and secure it with a low-profile titanium plate or crossed K-wires.
Step 3: Calcaneal Osteotomy (Dwyer or Lateralizing Shift)
If the hindfoot varus is rigid, a calcaneal osteotomy is mandatory to restore the mechanical axis.
1. Make an oblique incision over the lateral calcaneus, posterior to the sural nerve and peroneal tendons.
2. Incise the periosteum and expose the lateral wall of the calcaneus.
3. For a Lateralizing Shift: Perform an oblique osteotomy from posterior-dorsal to anterior-plantar. Translate the posterior tuberosity laterally by 10 mm.
4. For a Dwyer (Closing Wedge): Remove a laterally based wedge of bone to correct the varus angulation.
5. Fix the osteotomy with one or two large-fragment (6.5 mm or 7.3 mm) cannulated headless compression screws directed from the heel pad into the anterior calcaneus.
Step 4: Tendon Transfers
To prevent recurrence, the dynamic muscle imbalance must be neutralized.
* Peroneus Longus to Peroneus Brevis Transfer: The overpowering peroneus longus is transected at the level of the cuboid and tenodesed to the peroneus brevis. This removes the plantarflexing force on the first ray and augments eversion.
* Jones Transfer: For severe clawing of the hallux, the EHL is transected at the IP joint, rerouted through the neck of the first metatarsal, and sutured to itself. The IP joint of the hallux is then fused to prevent a drop-toe deformity.
* Hibbs Transfer: The extensor digitorum longus (EDL) tendons are transferred to the lateral cuneiform to elevate the midfoot and reduce clawing of the lesser toes.
Pitfall: Failing to address the dynamic muscle imbalance (e.g., leaving a strong peroneus longus unopposed) will inevitably lead to recurrence of the cavovarus deformity, regardless of how perfect the bony correction appears intraoperatively.
Step 5: Triple Arthrodesis (Salvage)
In older patients with severe, rigid deformities and secondary osteoarthritis of the subtalar and transverse tarsal joints, joint-sparing osteotomies will fail. A triple arthrodesis (fusion of the subtalar, talonavicular, and calcaneocuboid joints) is required.
1. Utilize a standard lateral approach to access the subtalar and calcaneocuboid joints, and a medial approach for the talonavicular joint.
2. Aggressively resect the articular cartilage and subchondral bone to correct the varus and elevate the arch.
3. Fixate the joints using large cannulated screws or specialized midfoot fusion plates.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The postoperative management is as critical as the surgical execution to ensure bony union and tendon transfer integration.
- Weeks 0-2: The patient is placed in a bulky, non-weight-bearing (NWB) posterior splint. The limb must remain strictly elevated to mitigate edema and prevent wound complications.
- Weeks 2-6: Sutures are removed at 2 weeks. The patient is transitioned to a short-leg fiberglass cast. Strict NWB status is maintained.
- Weeks 6-10: Radiographs are obtained to assess bony healing of the osteotomies or fusions. If callus formation is evident, the patient is transitioned to a controlled ankle motion (CAM) boot and allowed to begin progressive partial weight-bearing.
- Weeks 10-16: Full weight-bearing in the CAM boot is permitted. Physical therapy is initiated, focusing on strengthening the tendon transfers, restoring ankle range of motion, and proprioceptive training.
- Months 4-6: Transition to regular footwear, often utilizing a custom orthotic with a lateral heel wedge and first ray cutout to support the reconstruction. Return to high-impact activities is generally restricted until 6 to 9 months postoperatively.
CONCLUSION
The management of cavovarus foot deformity demands a comprehensive understanding of its complex etiology and biomechanical underpinnings. By systematically evaluating the flexibility of the hindfoot and forefoot, and meticulously executing a combination of soft tissue releases, bony osteotomies, and dynamic tendon transfers, the orthopedic surgeon can successfully restore a plantigrade, stable, and pain-free foot.
📚 Medical References
- cavovarus foot deformity in Charcot-Marie-Tooth disease, J Pediatr Orthop 25:360, 2005.
- Bradley GW, Coleman SS: Treatment of the calcaneocavus foot deformity, J Bone Joint Surg 63A:1159, 1981.
- Charcot JM, Marie P: Sur une forme particuliere d’atrophie musculaire souvent familiale debutant par les pied et les jambes et atteignant plus tard les mains, Rev Med p 96, 1886.
- Coleman SS: Complex foot deformities in children, Philadelphia, 1983, Lea & Febiger. Coleman SS, Chestnut WJ: A simple test for hind foot fl exibility in the cavovarus foot, Clin Orthop Relat Res 123:60, 1977.
- Daher YH, Lonstein JE, Winter RB, et al: Spinal deformities in patients with Charcot-Marie-Tooth disease: a review of 21 patients, Clin Orthop Relat Res 202:219, 1986.
- Dejerine J, Sottas J: Sur la neurite interstitielle hypertrophique et progressive de l’enfance, CR Soc Biol 45:63, 1893.
- Dwyer FC: The treatment of relapsed club foot by the insertion of a wedge into the calcaneum, J Bone Joint Surg 45B:67, 1963.
- Fuller JE, DeLuca PA: Acetabular dysplasia and CharcotMarie-Tooth disease in a family, J Bone Joint Surg 77A:1087, 1995.
- Gould N: Surgery in advanced Charcot-Marie-Tooth disease, Foot Ankle 4:267, 1984.
- Guyton GP, Mann RA: The pathogenesis and surgical management of foot deformity in Charcot-Marie-Tooth disease, Foot Ankle Clin 5:317, 2000.
- Hayasaka K, Himoro M, Sato W, et al: Charcot-Marie-Tooth neuropathy type 1B is associated with mutations of the myelin P0 gene, Nat Genet 5:31, 1993.
- Hensinger RN, MacEwen GD: Spinal deformity associated with heritable neurologic conditions: spinal muscular atrophy, Friedreich’s ataxia, familial dysautonomia, and Charcot-MarieTooth disease, J Bone Joint Surg 58A:13, 1976.
- Hibbs RA: An operation for “claw-foot,” JAMA 73:1583, 1919.
- International Myotonic Dystrophy Consortium: New nomenclature and DNA testing guidelines for myotonic dystrophy type1 (DM-1), Neurology 54:1218, 2000.
- Jansen GA, Ferdinandusse S, Skjeldal OH, et al: Molecular basis of Refsum disease: identifi cation of new mutations in the phytanoyl-CoA hydroxylase cDNA, J Inherit Metab Dis 21:228, 1998.
- Jones R: The soldier’s foot and the treatment of common deformities of the foot, II: claw-foot, BMJ 1:749, 1916.
- Kaplan L, Margulies JY, Kadari A, et al: Aspects of spinal deformity in familial dysautonomia (Riley-Day syndrome), Eur Spine J 6:33, 1997.
- Kirkpatrick JS, Goldner JL, Goldner RD: Revision arthrodesis for tibiotalar pseudarthrosis with fi bular onlay-inlay graft and internal screw fi xation, Clin Orthop Relat Res 268:29, 1991.
- Kumar SJ, Marks HG, Bowen JR, et al: Hip dysplasia associated with Charcot-Marie-Tooth disease in the older child and adolescent, J Pediatr Orthop 5:511, 1985.
- Lorenzetti D, Pareyson D, Sghirlanzoni A, et al: A 1.5-Mb deletion in 17p11.2-p12 is frequently observed in Italian families with hereditary neuropathy with liability to pressure palsies, Am J Hum Genet 56:91, 1995.
- Lupski JR, Chance PF, Garcia CA: Inherited primary peripheral neuropathies: molecular genetics and clinical implications of CMT1A and HNPP, JAMA 270:2326, 1993.
- Lupski JR, de-Oca-Luna RM, Slaugenhaupt S, et al: DNA duplication associated with Charcot-Marie-Tooth disease type 1A, Cell 66:219, 1991.
- Mann RA, Missirian J: Pathophysiology of Charcot-Marie-Tooth disease, Clin Orthop Relat Res 234:221, 1988.
- McCluskey WP, Lovell WW, Cummings RJ: The cavovarus foot deformity: etiology and management, Clin Orthop Relat Res 247:27, 1989.
- Medhat MA, Krantz H: Neuropathic ankle joint in CharcotMarieTooth disease after
You Might Also Like

