Pelvis Chiari Medial Osteotomy: Salvaging Dysplastic Hips
Key Takeaway
We review everything you need to understand about Pelvis Chiari Medial Osteotomy: Salvaging Dysplastic Hips. The Chiari medial displacement osteotomy of the pelvis is a salvage procedure for acetabular dysplasia in painful, unstable hips, especially when congruent reduction is not possible. This pericapsular osteotomy through the iliac bone medializes the acetabulum, forming a shelf to improve posterior and lateral femoral head coverage, aiming for a stable, pain-free hip.
Comprehensive Introduction and Patho-Epidemiology
The Chiari medial displacement osteotomy of the pelvis remains a highly specialized, single pericapsular osteotomy designed primarily as a salvage procedure for the management of severe acetabular dysplasia in the painful, unstable hip. Originally described by Karl Chiari in 1955, this technique fundamentally differs from reorientation osteotomies, such as the Bernese periacetabular osteotomy (PAO) or the triple innominate osteotomy of Steel or Tönnis. While reorientation osteotomies aim to reposition native hyaline cartilage over the femoral head to achieve a congruous reduction, the Chiari osteotomy is reserved for clinical scenarios where congruous reduction is anatomically and biologically impossible. This structural impossibility typically arises from advanced arthrosis, severe femoral head asphericity (such as coxa magna or coxa plana), or profound subluxation that precludes the use of standard rotational osteotomies.


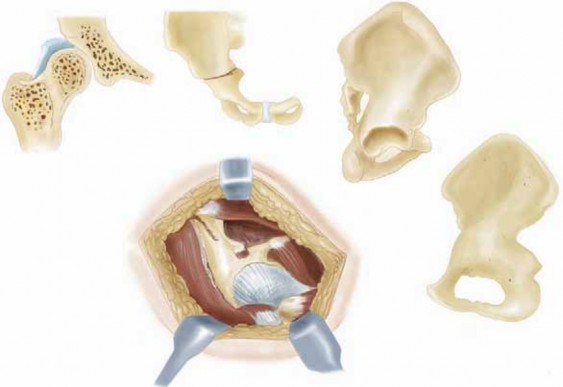
By executing an osteotomy through the iliac (innominate) bone just superior to the acetabular rim, the acetabulum and the hip joint are displaced medially. The proximal ilium remains in situ, effectively forming a robust, lateral bony roof over the subluxated femoral head. This procedure relies on the interposition of the superior joint capsule between the newly created iliac roof and the femoral head. Over time, under the influence of compressive and shear forces, this interposed capsule undergoes a remarkable biological transformation known as fibrocartilaginous metaplasia. This newly formed fibrocartilage acts as a functional, albeit non-hyaline, articular surface, providing a biological interpositional arthroplasty that significantly reduces pain and mechanically stabilizes the hip joint.


The patho-epidemiology of conditions necessitating a Chiari osteotomy is rooted in the natural history of untreated or recalcitrant pediatric hip disorders. Patients typically present in their second to fourth decades of life with secondary osteoarthritis superimposed on severe developmental dysplasia of the hip (DDH), sequelae of Legg-Calvé-Perthes disease, or post-infectious hip deformities. In these cohorts, the femoral head becomes severely deformed (coxa magna), rendering the native acetabulum entirely insufficient for containment. The epidemiological burden of these complex deformities, while decreasing due to widespread neonatal ultrasound screening for DDH, remains significant in tertiary orthopedic referral centers. Furthermore, the procedure serves as a critical bridge, delaying the need for total hip arthroplasty (THA) in young, active patients who would otherwise rapidly wear out conventional arthroplasty bearing surfaces.


Understanding the progression of articular degeneration in these patients is paramount. The incongruous joint experiences astronomically high peak contact stresses, particularly at the lateral acetabular rim, leading to rapid chondral delamination, subchondral cyst formation, and eventual collapse. The Chiari osteotomy directly addresses this by increasing the weight-bearing surface area and medializing the mechanical axis of the hip. This medialization fundamentally alters the biomechanical environment, shifting the center of rotation closer to the pubic symphysis and dramatically reducing the joint reactive forces. Consequently, the procedure not only provides structural coverage but actively alters the pathological force vectors driving the degenerative cascade.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of pelvic osteology and pericapsular anatomy is an absolute prerequisite for the safe and effective execution of the Chiari osteotomy. The innominate bone, at the level of the supra-acetabular corridor, presents a complex three-dimensional geometry. The osteotomy must be performed immediately superior to the capsular insertion on the acetabular rim, traversing from the anterior inferior iliac spine (AIIS) anteriorly to the greater sciatic notch posteriorly. The trajectory of this cut is fraught with danger; if the osteotomy is placed too proximally, the resulting lateral coverage will be inadequate, and the interposed capsule will not be supported. Conversely, an osteotomy placed too distally risks catastrophic intra-articular penetration, violating the remaining articular cartilage and accelerating joint destruction.


The neurovascular anatomy surrounding the greater sciatic notch dictates the posterior limits of the dissection and osteotomy. The sciatic nerve, exiting the pelvis inferior to the piriformis muscle, lies in close proximity to the posterior exit point of the osteotomy. Subperiosteal dissection must be meticulous, utilizing blunt, curved retractors (such as sciatic nerve retractors) placed subperiosteally into the notch to protect the nerve and the superior gluteal vessels during the bone cut. The superior gluteal nerve and artery, which exit the pelvis through the greater sciatic notch superior to the piriformis, are at risk during lateral dissection and retraction of the abductor musculature. Excessive tension on the gluteus medius and minimus must be avoided to prevent iatrogenic denervation and subsequent severe Trendelenburg gait.


Biomechanically, the Chiari osteotomy is a masterclass in the application of Pauwels' principles of hip biomechanics. The joint reactive force across the hip is a function of body weight and the ratio between the body weight moment arm and the abductor moment arm. By displacing the acetabulum and the femoral head medially, the Chiari osteotomy significantly shortens the body weight moment arm (the distance from the center of gravity to the center of the femoral head). Simultaneously, the lateralization of the greater trochanter relative to the new center of rotation increases the effective lever arm of the abductor musculature. This dual biomechanical advantage exponentially decreases the total joint reactive forces, offloading the compromised articular cartilage and facilitating the survival of the joint.


Furthermore, the biological biomechanics of the interposed capsule cannot be overstated. The capsule, normally a fibrous structure rich in type I collagen, is subjected to compressive loading between the raw cancellous bone of the proximal iliac fragment and the femoral head. This mechanical stimulus induces cellular differentiation, leading to the synthesis of type II collagen and proteoglycans, characteristic of fibrocartilage. For this metaplasia to occur successfully, the hip must maintain a functional range of motion post-operatively. A stiff hip will not provide the necessary dynamic mechanical environment, leading to capsular necrosis or ossification rather than the desired fibrocartilaginous transformation.
Exhaustive Indications and Contraindications
The decision to perform a Chiari osteotomy requires meticulous patient selection, as the procedure is fundamentally a salvage operation. The primary indication is the presence of a painful, dysplastic hip in an adolescent or young adult where the femoral head cannot be congruously reduced into the true acetabulum. This is most frequently encountered in severe, neglected DDH, advanced Legg-Calvé-Perthes disease with severe coxa magna and extrusion, and complex post-traumatic or post-infectious hip deformities. In these scenarios, spherical reorientation osteotomies (like the PAO) are contraindicated because rotating the acetabulum over an aspherical head will result in a hinge-abduction phenomenon, exacerbating joint incongruity and accelerating arthrosis.


Another critical indication is the presence of inadequate acetabular bone stock that precludes the use of a shelf arthroplasty or a rotational osteotomy. The Chiari osteotomy utilizes the entire width of the ilium to provide coverage, making it highly effective even when the lateral acetabular rim is severely deficient. Additionally, it is often indicated in patients with paralytic hip instability, such as those with cerebral palsy or myelomeningocele, where achieving deep, stable coverage is paramount to preventing recurrent dislocation, provided the patient has adequate ambulatory potential.


Contraindications to the Chiari osteotomy are rigid and must be strictly respected to avoid disastrous outcomes. The most absolute contraindication is a stiff hip. Because the procedure relies on capsular metaplasia driven by joint motion, a hip with less than 90 degrees of flexion or less than 15 degrees of abduction will fail to form a functional fibrocartilaginous articulation, resulting in severe stiffness and persistent pain. Advanced osteoarthritis with complete loss of joint space and bone-on-bone articulation across the entire weight-bearing dome is also a contraindication; in such cases, total hip arthroplasty or arthrodesis is the appropriate definitive management. Active intra-articular infection and severe osteopenia, which would compromise the fixation and stability of the displaced fragment, represent further absolute contraindications.
| Category | Specific Clinical Scenarios | Rationale / Notes |
|---|---|---|
| Primary Indications | Severe DDH with incongruity, Coxa Magna (LCPD), Coxa Plana | Salvage procedure when PAO/Triple osteotomy will cause hinge abduction. |
| Secondary Indications | Paralytic hip instability (CP, Spina Bifida), failed previous osteotomies | Provides massive structural coverage utilizing the full iliac width. |
| Absolute Contraindications | Stiff hip (<90° flexion, <15° abduction), Active Infection | Motion is strictly required for capsular fibrocartilaginous metaplasia. |
| Relative Contraindications | Advanced OA (Tonnis Grade 3), Severe Osteopenia, Age > 45 | Poor biological healing capacity; THA is generally preferred in older demographics. |

Surgeons must also carefully evaluate the patient's soft tissue envelope and muscular function. Severe abductor deficiency is a relative contraindication. While the Chiari medializes the hip center and theoretically improves abductor mechanics, a completely non-functional abductor mechanism will not be salvaged by the osteotomy, and the patient will continue to suffer from a severe Trendelenburg gait and instability. Comprehensive pre-operative counseling is mandatory, ensuring the patient understands that the Chiari is a joint-preserving salvage procedure designed to buy time—often decades—before a definitive total hip arthroplasty becomes necessary.
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning for a Chiari osteotomy demands an exhaustive radiographic evaluation to precisely map the patient's pathoanatomy. Standard imaging must include an anteroposterior (AP) radiograph of the pelvis, a false-profile view of Lequesne and de Sèze, and functional views such as abduction/adduction and flexion/extension films. The AP pelvis is utilized to measure the center-edge (CE) angle of Wiberg, the extrusion index, and the degree of subluxation. Crucially, the abduction view helps determine if the femoral head can be centralized and if a hinge-abduction phenomenon exists. If the joint congruency improves in abduction, a varus derotational femoral osteotomy (VDRO) may be required concomitantly with the Chiari.


Advanced cross-sectional imaging, specifically a fine-cut computed tomography (CT) scan with 3D reconstructions, is now considered the gold standard for pre-operative templating. The CT scan allows the surgeon to assess the exact bone stock of the ilium just superior to the acetabulum, measuring the thickness and depth of the bone where the osteotomy will be performed. 3D templating software is utilized to simulate the osteotomy cut. The trajectory of the cut is critical; it must be angled 10 to 15 degrees proximally (up-slope) from lateral to medial. This proximal angulation is mathematically designed to prevent the distal fragment from sliding laterally under the sheer force of body weight once the patient begins weight-bearing.

Patient positioning is a critical step that directly influences the intra-operative fluoroscopic evaluation and the ease of the surgical approach. The patient is typically positioned supine on a fully radiolucent Jackson table or a specialized orthopedic traction table. The supine position allows for easy comparison of leg lengths and facilitates bilateral fluoroscopic imaging. A bump is placed under the ipsilateral hemipelvis to slightly elevate the operative side, aiding in the lateral dissection. Some surgeons prefer the lateral decubitus position, arguing it provides superior access to the sciatic notch; however, this orientation complicates true AP fluoroscopic imaging, which is essential for assessing the osteotomy level and the degree of medial displacement.


Draping must be extensive, allowing the operative leg to be freely draped into the sterile field to permit dynamic intra-operative manipulation. The entire hemipelvis, from the umbilicus to the gluteal cleft, and the entire lower extremity down to the foot, should be prepped and draped. Intra-operative fluoroscopy is positioned to allow seamless transition between AP, obturator oblique, and iliac oblique views. Before the skin incision is made, a "time-out" must confirm the operative side, and fluoroscopy should be used to mark the planned level of the osteotomy on the skin, correlating the external landmarks with the superior rim of the acetabulum.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach for the Chiari osteotomy is most commonly executed via a modified Smith-Petersen (iliofemoral) or an ilioinguinal approach, depending on surgeon preference and the need for concomitant procedures. The incision begins at the middle third of the iliac crest, extending anteriorly to the anterior superior iliac spine (ASIS), and then curving distally along the interval between the tensor fasciae latae (TFL) and the sartorius. The superficial fascia is incised, and the internervous plane between the femoral nerve (sartorius) and the superior gluteal nerve (TFL) is developed. The lateral femoral cutaneous nerve must be identified and carefully mobilized, usually retracting it medially to prevent traction neuropraxia.

Deep dissection involves releasing the abductor musculature (gluteus medius and minimus) subperiosteally from the outer table of the ilium, extending posteriorly toward the greater sciatic notch. Simultaneously, the iliacus is elevated from the inner table of the ilium. The reflected head of the rectus femoris is identified and detached from the joint capsule, while the straight head may be preserved or tenotomized depending on the required exposure. It is of absolute, paramount importance that the hip joint capsule remains completely intact. Any inadvertent capsulotomy will compromise the interposed tissue, leading to leakage of synovial fluid, failure of fibrocartilaginous metaplasia, and direct bone-to-bone contact between the femoral head and the iliac osteotomy site.

Once the inner and outer tables are exposed, blunt curved retractors (such as modified Taylor or sciatic nerve retractors) are carefully passed subperiosteally through the greater sciatic notch. These retractors protect the sciatic nerve posteriorly and the obturator neurovascular bundle medially. The osteotomy level is verified fluoroscopically; it must be 2 to 3 millimeters superior to the capsular reflection. The cut is typically initiated with an oscillating saw or a Gigli saw passed through the sciatic notch, and completed with sharp, broad osteotomes. The trajectory must be strictly maintained at a 10 to 15-degree proximal angle. An inadvertent distal trajectory will breach the acetabular vault, leading to catastrophic intra-articular damage.

Following the completion of the osteotomy, the displacement maneuver is performed. The operative leg is placed in abduction, and a strong medially directed force is applied to the greater trochanter, while a laterally directed force is applied to the proximal iliac fragment using a bone hook or a Schanz pin. The goal is to achieve approximately 50% to 60% medial displacement of the distal fragment relative to the proximal ilium, ensuring adequate coverage of the femoral head. Once optimal displacement is confirmed fluoroscopically, the osteotomy is provisionally stabilized with heavy Kirschner wires. Definitive fixation is achieved using two or three fully threaded cortical screws or cannulated screws directed from the proximal ilium down into the dense bone of the distal fragment (the acetabular roof).
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the Chiari osteotomy is associated with a distinct profile of intra-operative and post-operative complications, reflecting the complexity of pelvic osteotomies. Intra-operative complications primarily involve neurovascular injury and unintended intra-articular fractures. The sciatic nerve is at the highest risk during the posterior exit of the osteotomy. Sciatic nerve palsy occurs in approximately 1% to 3% of cases, usually secondary to vigorous retraction, direct thermal injury from the saw, or direct mechanical trauma. The lateral femoral cutaneous nerve is frequently stretched, leading to transient meralgia paresthetica in up to 15% of patients, though this is typically self-limiting.


The most devastating intra-operative complication is an intra-articular osteotomy cut. If the osteotomy trajectory is too distal, the saw or osteotome will penetrate the weight-bearing dome of the acetabulum. This destroys the remaining hyaline cartilage and severely compromises the structural integrity of the joint, almost guaranteeing rapid progression to severe osteoarthritis. If recognized intra-operatively, the surgeon must attempt to redirect the cut, but the prognosis for joint preservation drops precipitously. Salvage in this scenario often accelerates the timeline to a total hip arthroplasty (THA).
Post-operative complications include delayed union or non-union of the osteotomy site, loss of displacement, and heterotopic ossification. Non-union is rare given the massive cancellous bone contact area but can occur if fixation is inadequate or if the patient bears weight prematurely. Loss of medial displacement typically results from an osteotomy cut that was perfectly horizontal or sloped distally, allowing the sheer force of body weight to push the distal fragment laterally. Heterotopic ossification (HO) around the abductor musculature can severely limit post-operative range of motion, directly threatening the success of the capsular metaplasia. Prophylactic measures, such as indomethacin or localized radiation, are sometimes considered in high-risk patients.
| Complication | Estimated Incidence | Prevention & Salvage Management |
|---|---|---|
| Sciatic Nerve Palsy | 1% - 3% | Prevention: Subperiosteal retractor placement in sciatic notch. Salvage: AFO for drop foot, expectant management (usually neuropraxia). |
| Intra-articular Cut | < 2% | Prevention: Accurate fluoroscopy, 10-15° proximal trajectory. Salvage: Conversion to THA if joint rapidly degenerates. |
| Loss of Displacement | 2% - 5% | Prevention: Proximal slope of osteotomy, rigid screw fixation. Salvage: Revision fixation vs early THA if symptomatic. |
| Heterotopic Ossification | 5% - 10% | Prevention: Meticulous hemostasis, NSAID prophylaxis. Salvage: Surgical excision after maturation if ROM is severely restricted. |

When the Chiari osteotomy eventually fails—usually decades later due to the natural progression of arthrosis—the patient becomes a candidate for total hip arthroplasty. Interestingly, a previous Chiari osteotomy often facilitates a subsequent THA. The medial displacement of the pelvis increases the lateral bone stock, providing an excellent bony bed for acetabular cup placement. However, the surgeon must be prepared for altered anatomy, significant scar tissue in the abductor interval, and the potential need for retained hardware removal.
Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation following a Chiari osteotomy is a delicate balance between protecting the bone healing at the osteotomy site and encouraging the early motion necessary for capsular fibrocartilaginous metaplasia. Phase I (0 to 6 weeks post-operatively) is characterized by strict protection. Patients are restricted to toe-touch weight-bearing (TTWB) or non-weight-bearing (NWB) on the operative extremity using crutches or a walker. This restriction is absolute; premature weight-bearing risks catastrophic loss of the medial displacement and failure of the fixation hardware. During this phase, deep vein thrombosis (DVT) prophylaxis is mandatory, and patients are instructed in gentle, passive, and active-assisted range of motion exercises to prevent joint stiffness and promote capsular remodeling.


Phase II (6 to 12 weeks) begins once radiographic evidence of early bony consolidation is observed at the osteotomy site. If the AP and false-profile radiographs demonstrate bridging trabeculae, the patient is gradually transitioned from partial weight-bearing (PWB) to full weight-bearing (FWB) over a 4-to-6-week period. Physical therapy during this phase intensifies, focusing heavily on the restoration of the abductor mechanism. The gluteus medius and minimus, having been stripped during the approach and functionally lengthened by the medialization of the hip center, require rigorous, targeted strengthening to overcome the anticipated post-operative Trendelenburg gait. Aquatic therapy is highly beneficial during this transition, allowing for buoyant unloading of the joint while facilitating concentric and eccentric muscle work.

You Might Also Like

