How to Accurately Determine the Severity of Neurological Impairment
Key Takeaway
For anyone wondering about How to Accurately Determine the Severity of Neurological Impairment, Determining the severity of neurological involvement is primarily assessed using the Frankel Scale, which classifies impairment from complete paralysis (A) to normal function (E). Further determination involves identifying specific cord syndromes: anterior column syndrome causes complete motor paralysis, central cord syndrome affects arms more than legs, and Brown-Séquard syndrome presents with unilateral paralysis and contralateral sensory loss.
Introduction and Epidemiology
Accurately determining the severity of neurological impairment following spinal trauma is the foundational step in guiding surgical decision-making, establishing a prognosis, and standardizing communication among spine surgeons and neurosurgeologists. Historically, the Frankel Scale provided a simple and direct method for categorizing the extent of neurological deficits. The Frankel classification stratifies patients into five distinct categories:
* Frankel A: Complete paralysis with absent motor and sensory function below the level of injury.
* Frankel B: Incomplete sensory preservation; only sensory function is intact below the injury level, with complete motor paralysis.
* Frankel C: Incomplete motor function; motor function is preserved below the injury level, but it is non-functional (muscle grade less than 3/5).
* Frankel D: Fair to good motor function; useful motor function is preserved below the injury level (muscle grade 3/5 or greater).
* Frankel E: Normal motor and sensory function, though abnormal reflexes may be present.

While the Frankel Scale laid the groundwork for standardized assessment, modern academic orthopedics relies heavily on the American Spinal Injury Association (ASIA) Impairment Scale (AIS), which offers a more granular, reproducible assessment of dermatomal and myotomal integrity.
Epidemiologically, traumatic spinal cord injury (SCI) exhibits a bimodal distribution, peaking in young adult males (high-energy trauma, motor vehicle collisions) and the elderly population (low-energy falls in the setting of cervical spondylosis). The incidence of specific incomplete cord syndromes varies, with Central Cord Syndrome being the most prevalent, particularly in the aging demographic. Understanding the precise neurological presentation—whether a complete transection, an incomplete syndrome, or transient spinal concussion—dictates the urgency and modality of operative intervention.
Surgical Anatomy and Biomechanics
A profound understanding of spinal cord cross-sectional anatomy, vascular supply, and injury biomechanics is requisite for interpreting incomplete cord syndromes and planning surgical decompression.
Spinal Cord Tracts and Somatotopic Organization
The spinal cord is organized into distinct white matter tracts and gray matter nuclei. The critical tracts for clinical evaluation include:
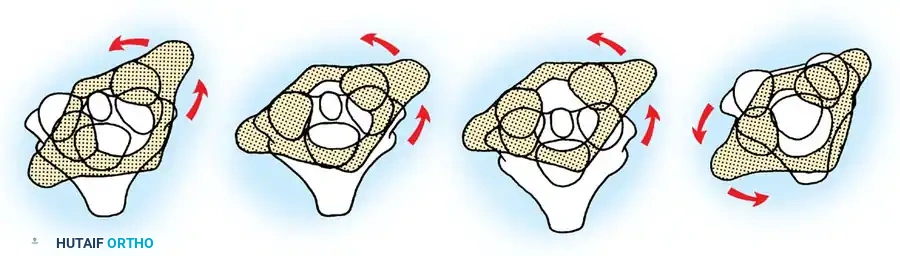
* Lateral Corticospinal Tract: Responsible for ipsilateral voluntary motor control. It exhibits a distinct somatotopic organization; the cervical motor fibers are located medially, while the thoracic, lumbar, and sacral fibers are layered progressively laterally. This anatomical arrangement explains the disproportionate upper extremity weakness seen in central cord injuries.
* Spinothalamic Tract: Located anterolaterally, this tract decussates within one to two levels of entry and carries contralateral pain and temperature sensation.
* Dorsal Columns (Fasciculus Gracilis and Cuneatus): Located posteriorly, these tracts carry ipsilateral proprioception, vibration, and fine touch.

Pathoanatomy of Incomplete Cord Syndromes
Anterior Column Syndrome
This syndrome results from damage to the anterior two-thirds of the spinal cord, typically secondary to axial loading mechanisms resulting in burst fractures. Retropulsed bone fragments compress the anterior spinal artery or the cord parenchyma directly. Clinically, this manifests as complete motor paralysis and loss of pain and temperature sensation (spinothalamic tract), with preservation of proprioception and deep pressure (dorsal columns). It carries the worst prognosis of all incomplete syndromes; absence of sacral pinprick or temperature sensation at 24 hours portends a functional recovery rate of merely 10–15%.
Central Cord Syndrome
The most common incomplete syndrome, typically arising from a hyperextension injury in a patient with pre-existing cervical spondylosis. The osteophytic ventral ridges and hypertrophied ligamentum flavum buckle inward, pinching the cord. The central gray matter and the medial aspect of the corticospinal tracts are preferentially injured. This produces the classic "man in a barrel" syndrome (MIB): flaccid, lower motor neuron paralysis in the upper extremities (due to anterior horn cell damage) and spastic, upper motor neuron paresis in the lower extremities, often with variable sensory sparing.

Brown-Séquard Syndrome
Caused by a functional hemitransection of the cord, most frequently associated with unilateral facet joint fractures, dislocations, or penetrating trauma. The clinical picture is defined by ipsilateral loss of motor function and proprioception (corticospinal and dorsal columns) and contralateral loss of pain and temperature sensation (spinothalamic tract). This syndrome carries an excellent prognosis, with over 90% of patients regaining ambulatory capacity and sphincter control.
Posterior Cord Syndrome
A rare entity usually following disruption of the posterior ligamentous complex or targeted penetrating trauma. Motor function and pain/temperature sensation remain intact, but patients suffer from profound ataxia due to the loss of vibration and position sense.
Cauda Equina Syndrome
Technically a peripheral nerve root injury rather than a true spinal cord lesion, occurring below the conus medullaris (typically L1-L2). It is characterized by asymmetric lower extremity weakness, saddle anesthesia, loss of rectal tone, absence of the bulbocavernosus reflex, and urinary retention (the most sensitive finding).

Spinal Concussion and Spinal Shock
Spinal concussion represents a transient arrest of neural conduction with rapid, spontaneous recovery. If a patient presents with a clinically complete lesion that persists beyond 12 hours, spinal concussion is definitively ruled out.
Spinal shock is a physiological state of areflexia and flaccidity immediately following cord trauma. The absence of reflexes can last from hours to weeks. The return of the bulbocavernosus reflex in the setting of persistent complete motor and sensory loss signifies the end of spinal shock and confirms a complete spinal cord injury. Conversely, any sacral sparing (perianal sensation, voluntary anal sphincter contraction) indicates an incomplete lesion with potential for recovery.
Indications and Contraindications
The decision to proceed with operative intervention relies on the stability of the spinal column, the presence of ongoing neural compression, and the trajectory of the patient's neurological status.
| Clinical Scenario | Operative Indications | Non-Operative Indications |
|---|---|---|
| Complete SCI (Frankel A) | Unstable fracture pattern, failure of closed reduction, facilitation of nursing care/rehabilitation. | Stable fracture pattern without ongoing compression, medically unstable polytrauma patient. |
| Incomplete SCI (Frankel B-D) | Progressive neurological deficit (Absolute), persistent compression in the setting of a static deficit, unstable fracture. | Rapidly improving neurological status, stable fracture without cord compression. |
| Central Cord Syndrome | Ongoing compression with plateaued recovery, instability. Early surgery (<24h) is increasingly favored. | Mild deficits with rapid spontaneous improvement, severe medical comorbidities in the elderly. |
| Cauda Equina Syndrome | Acute onset with profound bowel/bladder dysfunction (Surgical Emergency). | Chronic, insidious onset with stable, longstanding deficits (Relative). |
| Spinal Shock | Surgery is not contraindicated if there is mechanical instability or compression, but neurological prognosis cannot be accurately established. | - |

Pre Operative Planning and Patient Positioning
Thorough preoperative planning is mandatory to prevent secondary spinal cord injury, which can occur due to hypotension, hypoxia, or iatrogenic manipulation during positioning.
Hemodynamic Optimization
Current guidelines mandate the maintenance of Mean Arterial Pressure (MAP) greater than 85 mmHg for 7 days post-injury to ensure adequate perfusion to the watershed areas of the spinal cord and minimize the penumbra of ischemic injury. Vasopressors (e.g., norepinephrine, dopamine) should be titrated accordingly, guided by an arterial line.
Advanced Neuroimaging
While plain radiographs and non-contrast CT scans delineate the osseous architecture and fracture morphology (e.g., burst fractures, facet dislocations), Magnetic Resonance Imaging (MRI) is the gold standard for evaluating the neural elements. MRI sequences (T1, T2, STIR) differentiate between spinal cord edema (hyperintense T2 signal, better prognosis) and intramedullary hemorrhage (hypointense T2 core with hyperintense rim, poor prognosis). MRI also identifies traumatic disc herniations, which is critical before attempting closed reduction of cervical facet dislocations in awake patients.

Patient Positioning and Airway Management
Airway management in the setting of cervical instability requires awake fiberoptic intubation or video laryngoscopy with manual in-line stabilization. Cervical extension must be strictly avoided.
For anterior cervical procedures, the patient is positioned supine with a gel roll placed vertically between the scapulae to induce gentle cervical lordosis. The head is stabilized using a Mayfield horseshoe or skeletal traction.

For posterior cervical or thoracolumbar procedures, the patient is carefully log-rolled onto a Jackson spinal table. The Jackson table allows the abdomen to hang free, reducing intra-abdominal pressure, which subsequently decreases epidural venous engorgement and intraoperative hemorrhage. The head is secured in Mayfield tongs, maintaining neutral alignment.

Detailed Surgical Approach and Technique
Surgical intervention aims to decompress the neural elements, restore spinal alignment, and provide rigid internal fixation. The approach is dictated by the location of the pathology (anterior vs. posterior compression) and the biomechanical requirements of the construct.
Anterior Cervical Discectomy and Fusion
The anterior approach (Smith-Robinson) is ideal for central cord syndrome secondary to ventral osteophytes or traumatic disc herniations.
- Incision and Superficial Dissection: A transverse incision is made within a natural skin crease. The platysma is divided in line with the incision.
- Internervous Plane: The superficial fascia is incised, and the plane between the sternocleidomastoid (SCM) and carotid sheath laterally, and the trachea, esophagus, and thyroid medially, is developed.
- Deep Dissection: The prevertebral fascia is identified and incised. The longus colli muscles are mobilized laterally using electrocautery to expose the uncovertebral joints.
- Decompression: A complete discectomy is performed. The posterior longitudinal ligament (PLL) must be resected to ensure adequate decompression of the ventral spinal cord and to identify any extruded disc fragments.
- Reconstruction: An interbody graft (allograft or PEEK cage) is inserted to restore disc height and lordosis, followed by the application of an anterior cervical plate.

Posterior Cervical Laminectomy and Instrumentation
Indicated for multilevel congenital stenosis exacerbating central cord syndrome, or for the reduction of facet dislocations (Brown-Séquard syndrome).
- Exposure: A midline longitudinal incision is made. Subperiosteal dissection of the paraspinal musculature is performed laterally to the outer edges of the lateral masses.
- Instrumentation: Lateral mass screws are placed using the Magerl or Roy-Camille trajectories. The starting point is typically 1 mm medial and 1 mm inferior to the center of the lateral mass.
- Decompression: A wide laminectomy is performed using a high-speed burr and Kerrison rongeurs. The decompression must extend laterally to the medial aspect of the pedicles to ensure the cord is free from dorsal impingement.
- Reduction: For facet dislocations, the superior facet is gently levered over the inferior facet using a Penfield elevator. If the facet is locked, a partial facetectomy may be required to facilitate reduction.

Thoracolumbar Posterior Approach for Burst Fractures
For anterior cord syndrome caused by thoracolumbar burst fractures, a posterior approach utilizing ligamentotaxis or direct transpedicular decompression is frequently employed.
- Exposure: Midline incision with subperiosteal exposure of the spinous processes, laminae, and transverse processes.
- Pedicle Screw Insertion: The starting point in the lumbar spine is the intersection of the pars interarticularis, the superior articular facet, and the transverse process. Screws are placed at least one or two levels above and below the fractured vertebra.
- Ligamentotaxis: Distraction is applied across the construct. The tension generated in the intact PLL aids in reducing the retropulsed bone fragments away from the thecal sac.
- Direct Decompression: If ligamentotaxis is insufficient (or if the PLL is disrupted), a hemilaminectomy is performed. A transpedicular approach allows the surgeon to impact the retropulsed ventral bone fragments anteriorly, away from the spinal cord, using a reverse angled curette or impactor.


Complications and Management
Surgical management of spinal cord injuries carries significant inherent risks. Anticipation, early recognition, and algorithmic management of complications are critical to preserving neurological function.
| Complication | Incidence | Etiology / Presentation | Salvage Strategy / Management |
|---|---|---|---|
| Neurological Deterioration | 1-3% | Epidural hematoma, iatrogenic contusion, loss of MAP parameters. | Immediate stat MRI. Emergent return to OR for evacuation of hematoma. Optimize MAP > 85 mmHg. |
| Autonomic Dysreflexia | Up to 70% in lesions > T6 | Uncontrolled sympathetic response to noxious stimuli below injury level (e.g., distended bladder). Presents with severe hypertension, bradycardia, headache. | Medical emergency. Sit patient upright. Identify and remove stimulus (catheterize bladder, disimpact bowel). Administer rapid-onset antihypertensives (nitrates, nifedipine). |
| Incidental Durotomy | 5-10% | Iatrogenic tear during decompression of severe stenosis or removal of retropulsed bone. | Primary repair with 4-0 or 5-0 non-absorbable suture. Augment with fibrin glue/sealant and muscle patch. Bed rest for 24-48 hours post-op. Consider lumbar drain if refractory. |
| Post-Traumatic Syringomyelia | 1-5% (Late) | Cystic cavitation of the spinal cord occurring months to years post-injury. Presents as ascending neurological deficit (loss of pain/temp). | MRI surveillance. Surgical untethering of the cord or placement of a syringosubarachnoid or syringopleural shunt. |
| Hardware Failure | 2-8% | Poor bone quality, inadequate fixation points, pseudoarthrosis. | Revision surgery with extension of the construct, utilization of cemented screws, or combined anterior-posterior approaches. |


Post Operative Rehabilitation Protocols
The postoperative phase demands a multidisciplinary approach encompassing orthopedic spine surgery, physical medicine and rehabilitation (PM&R), physical therapy, and occupational therapy.
Immobilization and Orthotics
Depending on the rigidity of the internal fixation and the patient's bone quality, postoperative orthotics may be utilized. A rigid cervical collar (e.g., Miami J or Aspen collar) is typically worn for 6 weeks following posterior cervical procedures or multi-level anterior constructs. For thoracolumbar injuries, a Thoracolumbosacral Orthosis (TLSO) may be prescribed, particularly if the anterior column is deficient and was not reconstructed.
Deep Vein Thrombosis Prophylaxis
Patients with severe neurological impairment (Frankel A-C) are at an exceptionally high risk for venous thromboembolism. Chemical prophylaxis (Low Molecular Weight Heparin) should be initiated within 24 to 72 hours post-injury, provided there is no evidence of ongoing epidural hemorrhage on postoperative imaging. Mechanical prophylaxis (pneumatic compression devices) must be utilized continuously.
Neurogenic Bladder and Bowel Management
Urinary retention is a hallmark of spinal shock and cauda equina syndrome. Intermittent catheterization is preferred over indwelling Foley catheters to reduce the risk of catheter-associated urinary tract infections (CAUTIs). A strict bowel regimen utilizing chemical stimulants and mechanical disimpaction is instituted to prevent autonomic dysreflexia and paralytic ileus.

Summary of Key Literature and Guidelines
Academic orthopedic practice is governed by high-quality evidence and established clinical guidelines. The management of spinal cord injuries has evolved significantly based on several landmark trials.
Surgical Timing
The STASCIS (Surgical Timing in Acute Spinal Cord Injury Study) trial fundamentally shifted the paradigm regarding operative timing. The study demonstrated that early surgical decompression (within 24 hours of injury) in patients with acute SCI results in a significantly higher rate of meaningful neurological improvement (defined as a 2-grade improvement on the ASIA Impairment Scale) compared to delayed decompression, without an increase in complication rates.
Corticosteroid Administration
The use of high-dose methylprednisolone in acute SCI remains one of the most debated topics in orthopedic surgery. The NASCIS II and III (National Acute Spinal Cord Injury Study) trials initially suggested a modest neurological benefit if steroids were administered within 8 hours of injury. However, subsequent critical analyses revealed significant methodological flaws and highlighted severe adverse effects, including increased rates of sepsis, pneumonia, and gastrointestinal hemorrhage. Currently, the AOSpine guidelines and the Congress of Neurological Surgeons (CNS) do not recommend the routine administration of methylprednisolone for acute SCI. It is considered an option only in highly selected cases, with shared decision-making regarding the substantial risks.
Hemodynamic Management Guidelines
The American Association of Neurological Surgeons (AANS) and CNS guidelines strongly recommend the avoidance of systemic hypotension (systolic blood pressure < 90 mmHg) and advocate for the maintenance of MAP > 85 mmHg for 7 days following acute SCI. This practice is supported by class III evidence demonstrating improved neurological outcomes due to enhanced perfusion of the spinal cord penumbra.
You Might Also Like