Mastering the Anterior Cervical Approach: Longus Colli Muscle Insights

Key Takeaway
Discover the latest medical recommendations for Mastering the Anterior Cervical Approach: Longus Colli Muscle Insights. The anterior approach to the cervical spine exposes vertebral bodies C3-T1, disc spaces, and uncinate processes for procedures like disc excision, fusion, or tumor removal. Surgeons meticulously reflect the **longus colli muscle** to access these structures while safeguarding critical nerves like the recurrent laryngeal nerve. This approach is vital for various cervical spine pathologies.
Mastering the Anterior Cervical Approach Longus Colli Muscle Insights
Introduction and Epidemiology
The anterior approach to the cervical spine represents a cornerstone of modern spine surgery, providing direct access to the anterior vertebral column from C3 to T1. Its utility spans a broad spectrum of pathologies, allowing for effective decompression of neural elements and subsequent stabilization through arthrodesis. Historically pioneered by Robinson, Smith and Robinson, and Cloward in the mid-20th century, the anterior cervical discectomy and fusion (ACDF) remains one of the most frequently performed spinal procedures globally. The procedure's enduring relevance is attributed to its predictable outcomes in alleviating radiculopathy and myelopathy caused by degenerative disc disease, trauma, tumor, or infection.
The anterior cervical approach facilitates direct visualization and removal of anterior compressive pathology, including herniated discs, osteophytes, and tumor tissue, followed by interbody reconstruction to restore disc height, sagittal alignment, and achieve fusion. Its widespread adoption underscores a strong evidence base demonstrating favorable neurological improvement and pain relief in carefully selected patients. With an aging population and increasing incidence of degenerative spinal conditions, understanding the intricate surgical anatomy, meticulous technique, and potential complications of the anterior cervical approach is paramount for orthopedic surgeons and trainees alike. This comprehensive review will delve into the critical aspects of this approach, with a particular focus on the invaluable anatomical insights provided by the longus colli muscle.
Surgical Anatomy and Biomechanics
A thorough understanding of cervical spine anatomy is indispensable for safe and effective anterior cervical surgery. The approach navigates through several critical layers of anatomical structures, each demanding careful identification and protection.
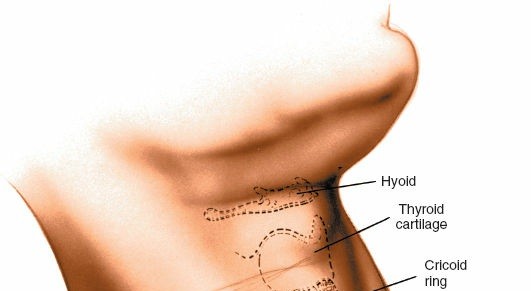
Superficial Anatomy and Musculature
The skin incision, typically transverse, is placed within a skin crease to optimize cosmetic outcome. Beneath the skin lies the platysma muscle, a thin sheet that must be sharply divided or carefully dissected to expose the deeper fascia. Deep to the platysma, the superficial cervical fascia encompasses the sternocleidomastoid (SCM) muscle. The SCM serves as a key landmark, separating the anterior and posterior triangles of the neck. The approach typically proceeds along the medial border of the SCM, although a true internervous plane is not strictly followed in the traditional approach, rather a fascial plane.
Visceral and Neurovascular Structures
Retraction of the SCM laterally exposes the carotid sheath, containing the common carotid artery, internal jugular vein, and vagus nerve. These vital neurovascular structures must be carefully protected and retracted laterally. Medial to the carotid sheath lie the trachea and esophagus, which are retracted medially. Identifying the pulsatile common carotid artery and maintaining it within the carotid sheath during lateral retraction is crucial to prevent vascular injury. The sympathetic chain, lying in the prevertebral fascia, is located lateral to the longus colli muscle, usually medial to the carotid sheath, but anterior to the transverse processes of the cervical vertebrae. Injury to the sympathetic chain can result in Horner's syndrome.
The recurrent laryngeal nerve (RLN) is the most important neurological structure at risk during the anterior approach to the cervical spine. Its course is asymmetric and highly variable. The left recurrent laryngeal nerve branches from the vagus nerve at the level of the aortic arch, ascends in the neck between the trachea and the esophagus, typically lying in the tracheoesophageal groove. The right recurrent laryngeal nerve branches from the vagus nerve in the lower neck, hooks around the right subclavian artery, and ascends more obliquely alongside the trachea. It often crosses from lateral to medial to reach the tracheoesophageal groove in the lower part of the neck, rendering it slightly more vulnerable during exposure than the left RLN. This anatomical variability contributes to the surgeon's choice of approach side, with some preferring the left due to the more predictable and less vulnerable course of the left RLN, while others approach from the side of pathology.
Illustration depicting the general anatomical planes of the anterior cervical approach, highlighting structures for medial and lateral retraction.
Deep Cervical Musculature The Longus Colli
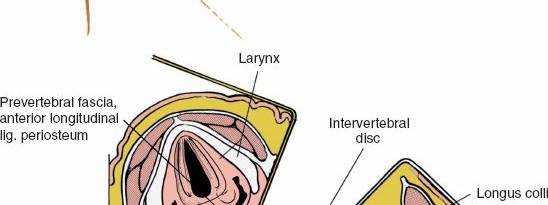
After retracting the trachea/esophagus medially and the carotid sheath laterally, the prevertebral fascia is encountered. This dense fascial layer overlies the anterior cervical vertebral bodies and the longus colli muscles. The longus colli muscles are a pair of long, flat muscles situated bilaterally on the anterior surface of the cervical and upper thoracic vertebral bodies, originating from the anterior tubercles of the transverse processes of C3-C6 and inserting into the anterior surface of C2-T3. Their primary function is to flex and rotate the neck.
For the anterior cervical approach, the longus colli muscles serve as invaluable surgical landmarks and protective barriers. They define the lateral extent of the vertebral body and delineate the safe working corridor. Meticulous subperiosteal dissection along the anterior aspect of the vertebral bodies involves detaching the longus colli muscles from their midline attachments. This dissection should be performed carefully, keeping a thin layer of muscle and periosteum on the vertebral body to protect the sympathetic chain, which often runs directly on the surface of the longus colli muscle, lateral to the vertebral body.
Detailed anatomical view demonstrating the longus colli muscles overlying the anterior cervical vertebral bodies.
Vertebral Arteries
The vertebral arteries ascend through the transverse foramina of C6 to C1. While typically protected within these bony canals, they are vulnerable to injury during lateral dissection at the uncovertebral joints, particularly if the dissection extends too far laterally, or in cases of anatomical variations or anomalous courses. Awareness of their position is critical during uncinatectomy or wide decompression.
Biomechanics of Anterior Cervical Fusion
The biomechanical rationale for anterior cervical decompression and fusion involves restoring physiological sagittal alignment, decompressing neural structures, and achieving stable arthrodesis. After discectomy and decompression, an interbody graft is inserted to maintain disc height and lordosis. Anterior plating provides immediate stability, acting as a tension band and protecting the graft from subsidence and expulsion. Multilevel fusions demand careful consideration of sagittal balance and the potential for increased stress at adjacent segments.
Indications and Contraindications
The anterior cervical approach is a versatile tool for addressing a wide array of cervical spinal pathologies. Indications are generally categorized into operative and non-operative groups, necessitating careful patient selection.
Operative Indications
The primary indications for anterior cervical intervention are rooted in neural compression or spinal instability.
- Cervical Radiculopathy: Persistent arm pain, numbness, or weakness due to nerve root compression from disc herniation or osteophytes, unresponsive to conservative management.
- Cervical Myelopathy: Spinal cord compression leading to gait disturbance, hand clumsiness, spasticity, and bladder dysfunction. This is an absolute indication for surgical intervention if progressive.
- Cervical Disc Herniation: Excision of herniated discs, particularly those centrally or paracentrally located, causing symptomatic radiculopathy or myelopathy. (R.B. Cloward, personal communication, 1969)
- Cervical Spondylotic Myelopathy CSM: Chronic spinal cord compression from disc degeneration, osteophyte formation, and ligamentum flavum hypertrophy.
- Cervical Instability: Resulting from trauma (fractures, dislocations), tumor resection, or severe degenerative changes. Open reduction and internal fixation of fractures can be achieved.
- Deformity Correction: Restoration of cervical lordosis and sagittal balance in cases of kyphotic deformity.
- Tumors: Excision of vertebral body tumors, often requiring extensive corpectomy and reconstruction with bone grafting.
- Infection: Drainage of abscesses and debridement for osteomyelitis, followed by stabilization.
- Biopsy: Diagnostic biopsy of vertebral bodies and disc spaces for suspected infection or tumor.
- Osteophyte Removal: Excision of osteophytes from the uncinate processes and from either the anterior or the posterior lip of the vertebral bodies contributing to neural compression.
- Failed Posterior Surgery: Select cases of persistent anterior compression after a posterior approach.
Contraindications
While generally safe, several factors may contraindicate an anterior cervical approach.
* Active Infection (Uncontrolled): Local or systemic infection that has not been adequately treated.
* Severe Dysphagia: Pre-existing severe swallowing difficulties may be exacerbated by the approach.
* Severe Anterior Scarring/Radiation History: Previous surgery or radiation to the neck can make dissection extremely challenging and increase the risk of complications.
* Severe Osteoporosis: Compromised bone quality may limit hardware purchase and fusion rates.
* Significant Posterior Compression: If the primary compression is posterior (e.g., extensive ligamentum flavum hypertrophy, posterior epidural mass), a posterior approach may be more appropriate or complementary.
* Anatomical Anomalies: Rarely, severe anatomical variations of major vessels may preclude the approach.
* Medical Comorbidities: Uncontrolled coagulopathy, severe cardiac or pulmonary disease making anesthesia high risk.
Summary of Operative vs Non-Operative Indications
| Indication Type | Operative Management | Non-Operative Management |
|---|---|---|
| Radiculopathy | Refractory arm pain, numbness, weakness from disc herniation or osteophytes. Progressive neurological deficit. | Physical therapy, NSAIDs, oral corticosteroids, cervical collar, epidural steroid injections, nerve root blocks. Typically pursued for 6-12 weeks prior to surgical consideration unless acute severe/progressive deficit. |
| Myelopathy | Any signs of spinal cord compression (gait disturbance, hand clumsiness, spasticity, hyperreflexia). Progressive symptoms. | Rarely indicated, as myelopathy often progresses without intervention. May include observation for very mild, stable cases in high-risk patients. |
| Instability | Traumatic fractures/dislocations with neurological compromise or significant instability. Tumor-related instability. Severe degenerative instability. | External immobilization (e.g., Halo vest) for select stable fractures without neurological compromise. Close observation. |
| Deformity | Progressive kyphosis or sagittal imbalance causing pain or neurological compromise. | Physical therapy, bracing for minor deformities, pain management. |
| Tumor/Infection | Symptomatic spinal cord/nerve root compression, instability, intractable pain. Biopsy for diagnosis. | Chemotherapy/radiation for certain tumors, antibiotics for infections (if no instability or severe neurological compromise). Close monitoring. |
| Pain | Severe, intractable neck/arm pain directly attributable to cervical pathology and refractory to all conservative measures. Often associated with radiculopathy or myelopathy. | NSAIDs, muscle relaxants, neuropathic pain medications, physical therapy, acupuncture, chiropractic care, facet injections, radiofrequency ablation, psychological support. |
Pre Operative Planning and Patient Positioning
Meticulous preoperative planning is critical to optimize surgical outcomes and minimize complications.
Preoperative Assessment
A comprehensive medical evaluation is essential to assess patient comorbidities, optimize medical status, and identify any potential contraindications. This includes a detailed history and physical examination, neurological assessment, and laboratory studies. Anesthesia consultation is vital for managing complex cases.
Imaging Studies
High-quality imaging is fundamental.
* Plain Radiographs: Anteroposterior, lateral, flexion-extension views provide information on alignment, stability, disc space height, and osteophyte formation. Dynamic views are critical for assessing instability.
* Magnetic Resonance Imaging (MRI): The gold standard for visualizing soft tissue compression, including disc herniations, spinal cord impingement, and ligamentous pathology. T1 and T2 weighted sequences, often with gadolinium contrast, are routinely employed.
* Computed Tomography (CT) Scan: Essential for detailed bony anatomy, assessing osteophyte burden, vertebral body destruction (e.g., tumors, fractures), and identifying anatomical variations (e.g., vertebral artery anomalies). CT myelogram may be beneficial if MRI is contraindicated or inconclusive.
* CT Angiography (CTA): Considered in revision cases or when concerns exist regarding vascular anomalies, particularly the vertebral arteries.
Patient Positioning
Correct patient positioning is paramount for optimal exposure, safety, and fluoroscopic access.
- Supine Position: The patient is placed supine on the operating table.
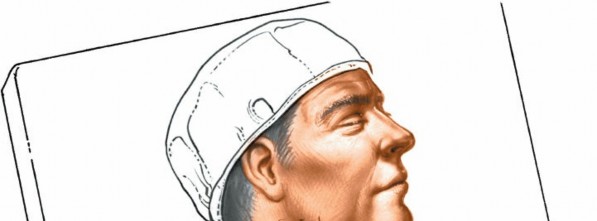
- Head and Neck Extension: A crucial step involves placing a shoulder roll (or gel roll) transversely beneath the patient’s shoulders. This extends the cervical spine, allows the head to drop back gently, and places the neck in a lordotic posture, stretching the anterior neck structures to facilitate exposure.
Patient positioned supine with a shoulder roll, illustrating cervical extension and gentle head support. - Head Support: The head is supported with a gel donut or specialized head holder, ensuring neutral rotation or slight rotation away from the operative side if preferred. Some cases may require application of halter traction so that it can be used later if distraction is required. The operating table can be elevated 30 degrees (reverse Trendelenburg) to reduce venous bleeding and make the neck more accessible.
- Arm Positioning: The patient’s arms are placed at their side, carefully padded to prevent pressure neuropathies.
- Taping: Adhesive tape is often applied to the shoulders and pulled caudally towards the feet. This depresses the shoulders, allowing for improved visualization of the cervicothoracic junction (C7-T1) on intraoperative fluoroscopy.

Patient positioning with shoulder taping for caudal retraction, aiding visualization of lower cervical levels. - Fluoroscopy Setup: The C-arm must be positioned to allow unobstructed anteroposterior and lateral fluoroscopic views of the cervical spine without repositioning the patient or the C-arm during surgery. This typically involves positioning the C-arm from the patient's side, parallel to the floor, allowing for both views simply by rotating the detector.
- Neuromonitoring: Intraoperative neuromonitoring (SSEP, MEP, EMG) is routinely employed, especially in myelopathic patients, to assess neurological function throughout the procedure.
Detailed Surgical Approach and Technique
The anterior cervical approach demands precision through sequential anatomical planes.
Incision and Superficial Dissection
- Incision Placement: A transverse skin incision, typically 3-5 cm in length, is made within a skin crease over the desired cervical level. For multilevel procedures, a slightly longer incision or two separate incisions can be considered. The choice of left versus right approach is often based on surgeon preference or side of primary pathology. A left-sided approach is often favored due to the generally more predictable course of the left recurrent laryngeal nerve.

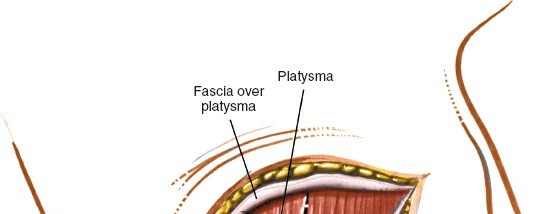
Surgical incision line, typically transverse within a skin crease for optimal cosmetic outcome. - Platysma Division: The platysma muscle is identified and sharply divided transversely. Subplatysmal flaps are then raised superiorly and inferiorly to optimize exposure.

Dissection through the platysma muscle, revealing deeper fascial layers. - Deep Cervical Fascia: The investing layer of the deep cervical fascia is incised longitudinally along the medial border of the sternocleidomastoid muscle.
Deep Dissection and Internervous Planes
- Identification of Sternocleidomastoid: The medial border of the SCM is identified.
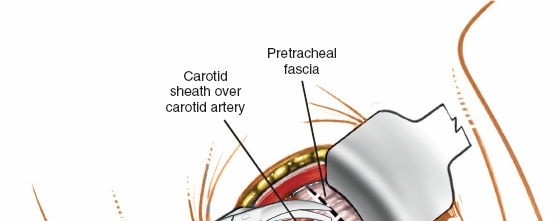
- Carotid Sheath Retraction: The surgeon digitally palpates for the carotid pulse. The plane between the carotid sheath (lateral) and the visceral compartment (medial) containing the trachea and esophagus is developed. The carotid sheath, with its contents (common carotid artery, internal jugular vein, vagus nerve), is gently retracted laterally using a deep blunt retractor.
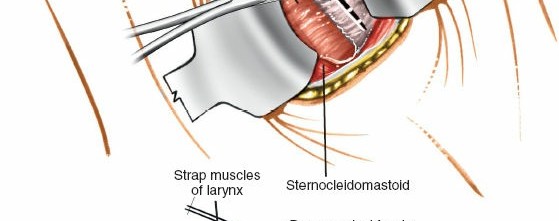
Initial deep dissection, identifying and separating the sternocleidomastoid and associated fascial planes.
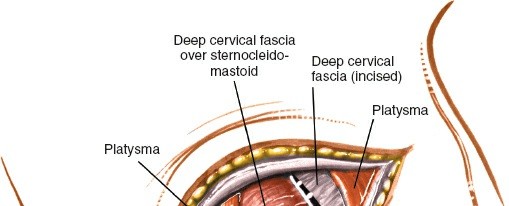
Further deep dissection, carefully isolating the carotid sheath for lateral retraction. - Visceral Retraction: The trachea and esophagus are retracted medially. Care must be taken to minimize trauma to the esophagus to prevent dysphagia. Intermittent release of retractors can help mitigate nerve and esophageal compression.
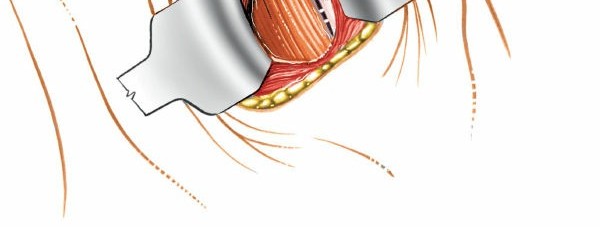
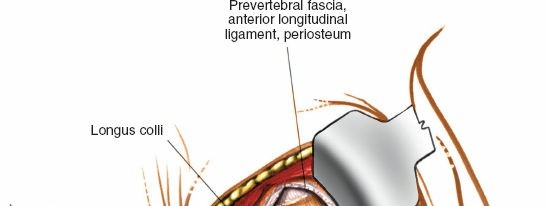
Placement of initial retractors, showing medial retraction of trachea/esophagus and lateral retraction of the carotid sheath. - Prevertebral Fascia Exposure: Once the carotid sheath is retracted laterally and the trachea/esophagus medially, the prevertebral fascia overlying the longus colli muscles and anterior vertebral bodies is exposed.
Exposure of the Vertebral Body and Longus Colli Muscle
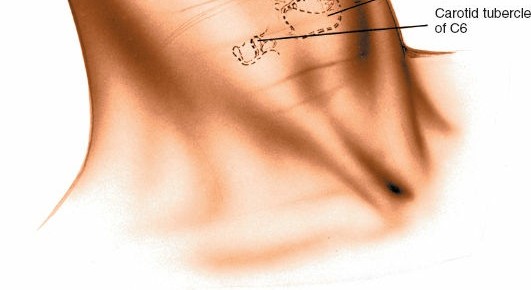
- Confirmation of Level: Intraoperative lateral fluoroscopy is used to confirm the correct surgical level. A needle can be inserted into the target disc space for precise localization.
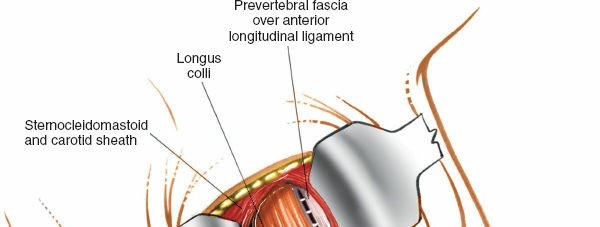
Intraoperative fluoroscopy for precise localization of the target cervical level. - Longitudinal Incision of Prevertebral Fascia: The prevertebral fascia is incised longitudinally along the midline of the vertebral bodies, extending across the superior and inferior limits of the planned dissection.
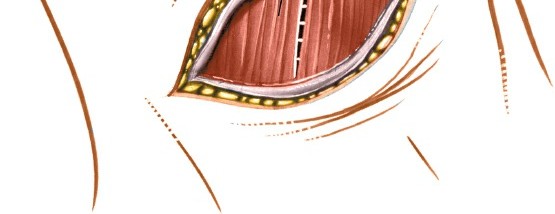
- Subperiosteal Dissection of Longus Colli: Using electrocautery and periosteal elevators, the longus colli muscles are meticulously dissected subperiosteally from the anterior surface of the vertebral bodies and disc spaces. This dissection should stay tightly on the bone. It is crucial to elevate the longus colli muscle from the midline laterally to expose the anterior vertebral bodies and disc space. This maneuver creates a bloodless field and protects the underlying sympathetic chain, which often runs deep to the longus colli, lateral to the vertebral body.

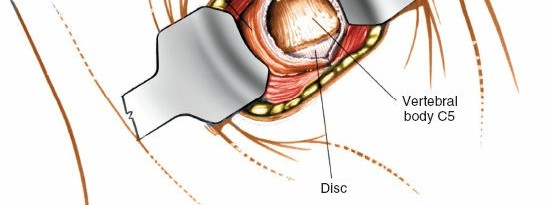
Incision of the prevertebral fascia and initial subperiosteal dissection of the longus colli muscles.
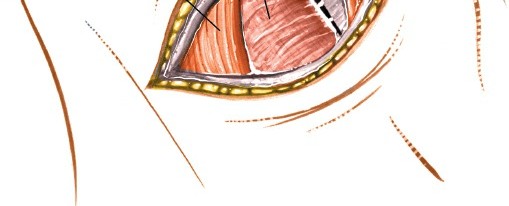
Further dissection illustrating the clear exposure of the anterior vertebral body after careful longus colli mobilization.
Discectomy and Decompression
- Placement of Caspar Pins and Distraction: Caspar self-retaining retractors are carefully placed by inserting pins into the vertebral bodies above and below the target disc space. Distraction is then applied to open the disc space and facilitate access. The pins should be placed centrally and parallel to the endplates.

Insertion of Caspar pins into the vertebral bodies for distraction, exposing the disc space. - Disc Annulus Incision: The anterior annulus fibrosus is sharply incised.
- Discectomy: Using various pituitary rongeurs, curettes, and osteotomes, the disc material is meticulously removed. The posterior longitudinal ligament (PLL) is then visualized.

The process of discectomy, removing disc material from the intervertebral space.
A different view of the discectomy, showing instruments used for thorough disc removal. - Decompression:
- Posterior Longitudinal Ligament (PLL): In cases of myelopathy or significant radiculopathy, the PLL is carefully resected using fine instruments (e.g., kerrison rongeurs, microcurettes) to ensure complete decompression of the spinal cord and nerve roots.
- Uncovertebral Joints (Uncinate Processes): Osteophytes arising from the uncinate processes (laterally) and posterior vertebral body lip (centrally) are removed using high-speed burrs and kerrison rongeurs. This step is critical for indirect foraminal decompression and release of nerve roots. Extreme caution is needed laterally to avoid vertebral artery injury.
- Endplate Preparation: The cartilaginous endplates are meticulously removed down to bleeding bone to promote fusion, while preserving the cortical bone to prevent graft subsidence.
Resection of osteophytes and preparation of the endplates for interbody graft placement.
Detailed view of endplate preparation, ensuring optimal surface for fusion.
Interbody Grafting and Fixation
- Graft Selection and Preparation: A variety of interbody fusion devices are available, including autogenous bone graft (e.g., iliac crest), allograft, and PEEK (polyetheretherketone) cages, often packed with bone morphogenetic proteins (BMPs) or local bone chips. The graft or cage size is carefully measured to match the disc space height and restore lordosis.

Measurement of the disc space to determine appropriate interbody graft size. - Graft Insertion: The selected graft or cage is impacted into the prepared disc space. Distraction is then slowly released, ensuring the graft is firmly seated and compressed within the intervertebral space.

Insertion of the interbody graft or cage into the prepared disc space. - Anterior Plating: An anterior cervical plate is then selected and contoured if necessary. It is secured to the anterior vertebral bodies above and below the fusion segment with bicortical or unicortical screws. The plate provides immediate stability and enhances fusion rates. Careful selection of screw length and trajectory is essential to avoid penetrating the spinal canal or adjacent disc spaces.

Application of the anterior cervical plate, securing the interbody graft and providing stability.

Screw insertion through the anterior plate into the vertebral bodies.
Final view of the anterior cervical plate and screws in place after fusion.
Illustration of single-level (ACDF) and multi-level (ACDF with plate) fixation.

Example of a multi-level anterior cervical fusion construct.
Closure
- Hemostasis: Thorough hemostasis is achieved. A small drain may be placed, especially in multilevel cases or if significant bleeding is encountered.
- Longus Colli Reapproximation: The longus colli muscles and prevertebral fascia are often reapproximated over the plate, providing an additional layer of soft tissue coverage.
- Muscle and Fascial Closure: The deep cervical fascia, platysma, and subcutaneous tissues are closed in layers with absorbable sutures.
- Skin Closure: The skin is closed with sutures or staples.
Surgical site prior to closure, showing the integrity of the approach.

Suture closure of the platysma layer.

Final skin closure following the anterior cervical approach.
Complications and Management
Despite its high success rate, the anterior cervical approach is associated with a range of potential complications, necessitating vigilant perioperative management and a clear understanding of salvage strategies.
Common Complications
| Complication | Incidence (%) | Salvage Strategies / Management |
|---|---|---|
| Dysphagia | 10-70 | Post-operative swelling, direct esophageal trauma, recurrent laryngeal nerve palsy. Managed with dietary modification, anti-inflammatory medications, proton pump inhibitors. Persistent dysphagia may require swallow therapy or endoscopy. Usually resolves within weeks to months. |
| Recurrent Laryngeal Nerve Palsy | 0.5-12 | Unilateral vocal cord paresis/paralysis leading to hoarseness. Due to direct trauma, retraction injury, or thermal injury. Managed with voice therapy. Most cases resolve spontaneously within 6-12 months. Rarely requires vocal cord injection/medialization. |
| Hematoma | 0.1-3 | Neck swelling, airway compromise. Requires immediate re-exploration for evacuation and hemostasis, especially if rapidly expanding or causing respiratory distress. Vigilant post-operative airway monitoring is crucial. |
| Esophageal Perforation | <0.1 | Dysphagia, odynophagia, fever, leukocytosis, subcutaneous emphysema. Highly morbid. Requires immediate surgical repair, nasogastric tube placement, broad-spectrum antibiotics, and sometimes diversion. |
| Cerebrospinal Fluid (CSF) Leak | <0.1 | Clear fluid drainage, headache, wound dehiscence. Due to dural tear during decompression. Managed with primary repair, fibrin glue, Valsalva maneuvers, Trendelenburg positioning, lumbar drain. Rare, but if undetected, can lead to meningitis. |
| Pseudarthrosis / Nonunion | 2-25 (single-level) | Persistent pain, hardware failure, progressive deformity. Often asymptomatic but can necessitate revision surgery (anterior, posterior, or combined approach), with additional bone grafting, biological augmentation, or different instrumentation. |
| Hardware Failure | 1-5 | Screw pullout, plate fracture, graft extrusion. Leads to instability, pseudarthrosis. Requires revision surgery with new instrumentation, potentially different plating constructs, or supplemental posterior fusion. |
| Infection (Deep Space) | <1 | Fever, erythema, pain, purulent drainage. Managed with surgical debridement, washout, culture-directed antibiotics, and potentially hardware removal (if fusion achieved). |
| Vertebral Artery Injury | <0.1 | Catastrophic hemorrhage, stroke. Due to lateral dissection extending beyond the uncovertebral joint. Requires immediate vascular control, compression, vascular repair, or embolization. Risk is higher with uncinatectomy or revision surgery. |
| Sympathetic Chain Injury (Horner's Syndrome) | <1 | Ipsilateral miosis, ptosis, anhydrosis. Due to direct trauma or excessive retraction of the longus colli muscle. Most cases are transient and resolve spontaneously within weeks to months. Symptomatic management as needed. |
| Nerve Root Injury | <1 | New or worsened radiculopathy. Due to direct trauma during decompression. Managed with corticosteroids, observation. Revision surgery for persistent compression or new deficits. |
| Spinal Cord Injury | <0.1 | New or worsened myelopathy, paralysis. Catastrophic. Due to direct cord trauma, intraoperative ischemia, or compression. Requires immediate assessment, potentially re-exploration. Very rare with careful technique. |
| Adjacent Segment Disease (ASD) | 2-4% per year | Degeneration at levels adjacent to the fusion. Can present as radiculopathy or myelopathy. Managed initially with conservative measures. Surgical intervention (ACDF or posterior fusion at the adjacent level) for progressive symptoms. |
Prophylactic Measures
Many complications can be minimized through meticulous surgical technique:
* Recurrent Laryngeal Nerve: Use of gentle retraction, intermittent release of retractors, careful electrocautery, and choosing the less vulnerable side when appropriate.
* Dysphagia: Atraumatic retraction of the esophagus and avoiding excessive cautery in the posterior pharyngeal wall. Post-operative steroids may be considered.
* Hematoma: Meticulous hemostasis throughout the procedure and consideration of a drain for high-risk patients.
* Sympathetic Chain: Staying tightly subperiosteal when dissecting the longus colli muscle and avoiding excessive lateral retraction.
Post Operative Rehabilitation Protocols
Postoperative care following anterior cervical fusion focuses on pain management, wound care, early mobilization, and gradually progressing activity to ensure optimal recovery and promote fusion.
Immediate Postoperative Period (Days 0-7)
- Pain Management: Multimodal analgesia, including NSAIDs, acetaminophen, and opioid sparing strategies, is employed. Patient-controlled analgesia (PCA) may be used initially.
- Wound Care: The incision is kept clean and dry. Dressings are typically changed within 24-48 hours.
- Airway Management: Close monitoring for signs of airway compromise (e.g., stridor, dysphagia, hematoma expansion) is essential. Head of bed elevation can reduce swelling.
- Mobilization: Patients are encouraged to ambulate on the day of surgery or the first postoperative day. Early mobilization helps prevent pulmonary complications and deep vein thrombosis.
- Cervical Collar: The use of a rigid cervical collar is variable among surgeons and depends on the stability of the construct, number of levels fused, and patient comorbidities. For single-level ACDF with plate fixation, a soft collar or no collar may suffice. Multilevel fusions or constructs with compromised stability often warrant a rigid collar for 6-12 weeks.
- Diet: Clear liquids initially, progressing to a soft diet as tolerated, then regular diet. Swallowing difficulties are common and should be monitored.
- Discharge: Patients are typically discharged within 1-2 days, once pain is controlled, they can tolerate oral intake, and are ambulatory.
Subacute Rehabilitation (Weeks 2-6)
- Activity Modification: Patients are advised to avoid heavy lifting, strenuous activities, and high-impact sports. Twisting and extreme neck movements should be avoided, especially if a collar is used.
- Wound Healing: The incision should be fully healed by this stage. Scar massage can be initiated after suture removal.
- Physical Therapy (Optional): For some patients, gentle physical therapy focusing on posture, cervical range of motion (within limits set by the surgeon), and scapular stabilization may begin. The emphasis is typically on protected motion and isometric exercises to avoid stress on the fusion.
Intermediate Rehabilitation (Months 2-6)
- Radiographic Assessment: Fusion status is typically assessed with plain radiographs (lateral and AP views, sometimes dynamic flexion/extension views) at 3, 6, and 12 months post-surgery. CT scans may be used if pseudarthrosis is suspected.
- Gradual Increase in Activity: As fusion progresses, activity restrictions are gradually lifted. Physical therapy intensifies, focusing on strengthening the deep neck flexors, scapular stabilizers, and improving cervical range of motion.
- Return to Work/Sport: Return to sedentary work is often possible within 4-6 weeks, while return to manual labor or contact sports is typically delayed until radiographic evidence of solid fusion (6-12 months).
Long-Term Follow-up (Beyond 6 Months)
- Monitoring for Adjacent Segment Disease (ASD): Long-term follow-up is important to monitor for the development of adjacent segment degeneration or disease, a known consequence of cervical fusion.
- Lifestyle Modifications: Patients are encouraged to maintain good posture, engage in core strengthening, and continue with a healthy lifestyle to support spinal health.
Summary of Key Literature and Guidelines
The anterior cervical approach has been extensively studied, with a robust body of literature supporting its efficacy and safety. Key milestones and ongoing research continue to refine surgical indications, techniques, and rehabilitation strategies.
Historical Context and Evolution
The foundational work of Robinson and Smith (1955) describing anterior cervical discectomy and interbody fusion, along with Cloward's development of specific instrumentation and techniques (1958), revolutionized the treatment of cervical disc pathology. Their innovations established the anterior approach as a viable and highly effective method for direct decompression. Early techniques primarily utilized autogenous bone graft, most commonly from the iliac crest. Subsequent advancements included the introduction of anterior cervical plating in the 1980s, which significantly improved fusion rates, reduced graft complications, and allowed for earlier patient mobilization. The development of allograft, synthetic cages (e.g., PEEK), and biologic adjuncts has provided surgeons with a broader array of reconstruction options.
Efficacy and Outcomes
Numerous prospective and retrospective studies, including randomized controlled trials, consistently demonstrate the effectiveness of ACDF for symptomatic cervical radiculopathy and myelopathy. Outcomes include significant improvement in arm pain, neurological deficits, and functional status. Fusion rates for single-level ACDF with anterior plating typically range from 90-98%. While the long-term incidence of adjacent segment disease remains a topic of ongoing research, ACDF remains a gold standard for specific indications.
Current Trends and Controversies
- Arthroplasty vs. Fusion: Cervical disc arthroplasty (CDA) has emerged as an alternative to ACDF, particularly for single-level degenerative disc disease causing radiculopathy, with the theoretical advantage of preserving motion and potentially reducing the incidence of adjacent segment disease. Current literature suggests comparable clinical outcomes between ACDF and CDA in the short to mid-term for appropriately selected patients, though long-term data for CDA is still evolving.
- Optimal Graft Choice: The debate continues regarding the optimal interbody graft material (autograft, allograft, PEEK cage with or without biologics). While autograft remains the biological gold standard, allograft and PEEK cages offer advantages in terms of avoiding donor site morbidity. The use of biologics like BMP-2 is controversial due to potential side effects (e.g., dysphagia, swelling, osteolysis).
- Multilevel Fusion: While single-level ACDF is highly successful, multilevel fusions, particularly three or more levels, are associated with higher rates of pseudarthrosis and potentially increased stress on adjacent segments. Considerations for alternative strategies, such as hybrid procedures (fusion at one level, arthroplasty at another) or posterior approaches, may arise in select multilevel cases.
- Minimally Invasive Techniques: Efforts to further minimize tissue disruption are ongoing, although the anterior cervical approach is already relatively minimally invasive compared to posterior approaches. Advances in endoscopic and navigation technologies continue to be explored.
Professional Guidelines
Guidelines from organizations such as the North American Spine Society (NASS), the American Academy of Orthopaedic Surgeons (AAOS), and various international spine societies provide evidence-based recommendations for the diagnosis and management of cervical degenerative conditions. These guidelines emphasize careful patient selection, comprehensive preoperative workup, consideration of non-operative management first for radiculopathy, and detailed informed consent regarding risks and benefits of surgery. The meticulous understanding of anatomy, particularly the relationship of critical structures like the recurrent laryngeal nerve and the longus colli muscles, continues to be a central tenet underscored by these professional bodies for safe and effective anterior cervical spine surgery.
Clinical & Radiographic Imaging

You Might Also Like