Operative Management of Osteochondritis Dissecans of the Knee

Key Takeaway
The treatment of osteochondritis dissecans (OCD) is dictated by patient skeletal maturity, lesion size, and stability. While juvenile OCD often resolves with conservative management, adult or unstable lesions necessitate surgical intervention. Operative strategies range from arthroscopic drilling to promote vascularity, to internal fixation of unstable fragments, and excision of loose bodies. The ultimate goal is to preserve joint congruity and prevent early-onset osteoarthritis.
INTRODUCTION AND TREATMENT PHILOSOPHY
The treatment of osteochondritis dissecans (OCD) is a highly nuanced orthopedic challenge that depends fundamentally on two critical factors: the patient’s age (specifically, skeletal maturity and physeal patency) and the degree of lesional involvement (stability, size, and location). The overarching objective of any treatment modality—whether conservative or surgical—is to promote the biological healing of the subchondral lesion prior to the closure of the physes, while concomitantly preventing the mechanical detachment of the osteochondral fragment.
Careful clinical assessment is mandatory. The surgeon must correlate the surface topography, size, and location of the lesion with the patient’s chronological age, skeletal maturity, and subjective symptoms. Failure to achieve healing leads to fragment separation, intra-articular loose body formation, and accelerated articular cartilage attrition, ultimately culminating in early-onset osteoarthritis.
NONOPERATIVE MANAGEMENT
In young patients with open physes (Juvenile Osteochondritis Dissecans or JOCD), the lesions possess a robust biological capacity for spontaneous healing. Consequently, conservative management is the first-line treatment for stable, intact lesions in this demographic.
Modalities of Conservative Care
Nonoperative protocols encompass a spectrum of interventions designed to unload the affected subchondral bone while maintaining joint health:
* Activity Modification: Immediate cessation of high-impact, repetitive loading sports (e.g., running, jumping).
* Weight-Bearing Restrictions: Utilization of crutches for partial or strict non–weight-bearing ambulation, depending on lesion severity and location.
* Immobilization: Short-term use of a cylinder cast or hinged knee brace to protect the joint during the acute symptomatic phase.
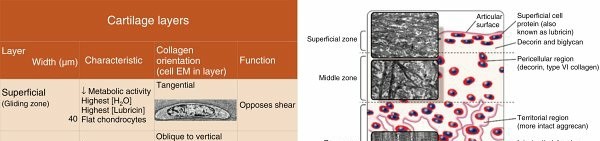
Clinical Pitfall: Prolonged immobilization must be strictly avoided. Articular cartilage relies on cyclical loading and joint motion for the diffusion of synovial fluid and essential nutrients. Extended periods of rigid immobilization lead to cartilage starvation, atrophy, and accelerated attrition.
While nonoperative treatment is highly successful in JOCD, it has a markedly limited role in older adolescents and adults, or in patients of any age presenting with unstable, symptomatic osteochondral lesions.
PREOPERATIVE IMAGING AND TEMPLATING
Accurate determination of the lesion's surface topography and subchondral stability is essential before proceeding to the operating room.
* Magnetic Resonance Imaging (MRI): The gold standard for evaluating the integrity of the overlying articular cartilage, the presence of synovial fluid behind the fragment (indicating instability), and the extent of subchondral bone edema.
* Computed Tomography (CT): Highly valuable for assessing the true osseous dimensions of the lesion and planning internal fixation trajectories.
* Plain Radiographs: Essential for initial diagnosis and monitoring healing. Notch views are particularly useful for classic posterolateral lesions of the medial femoral condyle.
INDICATIONS FOR OPERATIVE INTERVENTION
In older adolescents and adults, the prognosis for spontaneous healing is significantly less satisfactory than in younger patients, regardless of the conservative treatment applied. Surgical intervention becomes necessary to alter the natural history of the disease.
Primary Indications for Surgery:
* A symptomatic knee in a patient who is skeletally older than 12 years.
* A lesion larger than 1 cm in diameter.
* Involvement of the primary weight-bearing surface of the femoral condyle.
* Evidence of lesion instability (e.g., a high T2 signal rim behind the fragment on MRI).
* Failure of a compliant 3- to 6-month trial of nonoperative management.
* Presence of intra-articular loose bodies.
ARTHROSCOPIC SURGICAL TECHNIQUES
Arthroscopy is the cornerstone of modern OCD management. It serves a dual purpose: establishing a definitive diagnosis of surface topography and providing a minimally invasive therapeutic intervention.
Advantages of Arthroscopy:
* Immediate, tactile evaluation of articular cartilage integrity.
* Significant decrease in total rehabilitation time.
* Avoidance of the morbidity, physical scarring, and psychological impact of open arthrotomy.
* Reduced risk of postoperative infection and decreased length/cost of hospitalization.
Diagnostic Assessment and Topography
Upon entering the joint, the surgeon must carefully probe the lesion.
Surgical Pearl: When arthroscopy is performed, the intra-articular injection of methylene blue can be highly effective in defining the margins of the lesion. The dye selectively stains the fibrillated cartilage and fissures, highlighting the exact boundaries of the unstable fragment.
The knee must be flexed fully (often past 120 degrees) to view the entire lesion, particularly to locate lesions situated far posteriorly on the condyles. If the articular surface appears entirely intact with little to no visible change, intraoperative fluoroscopy is mandatory to precisely locate the subchondral defect.
Drilling of Intact Lesions
For lesions with intact articular cartilage but underlying subchondral sclerosis or non-healing defects, drilling is the procedure of choice. The goal is to breach the sclerotic rim, creating vascular channels that allow marrow-derived mesenchymal stem cells and angiogenic factors to access the lesion, thereby stimulating creeping substitution and bone healing.
- Technique: Using a 0.062-inch Kirschner wire or a specialized microfracture awl, multiple perforations are made through the articular surface into the subchondral bone.
- Depth: Holes must be drilled to a depth of 1.0 to 1.5 cm to ensure adequate penetration into healthy, vascularized cancellous bone.
- Physeal Warning: In skeletally immature patients, retrograde drilling, pinning, or bone grafting trajectories must be meticulously planned under fluoroscopy to ensure they do not cross the physis, which could precipitate premature growth arrest.
Fixation of Separated or Unstable Lesions
Lesions demonstrating early separation or partial detachment require mechanical stabilization. Partial detachment inevitably leads to a break in the cartilaginous border and the protrusion of fibrous tissue into the crater.
Step-by-Step Fixation Protocol:
1. Debridement: The fragment is hinged open (if partially attached) or temporarily removed. The underlying crater is meticulously curetted and trephined to remove all fibrous tissue down to healthy, bleeding subchondral bone.
2. Grafting: If there is a volumetric bone loss, the crater is packed with autologous cancellous bone graft to restore surface congruity and provide an osteoconductive matrix.
3. Reduction and Compression: The fragment is anatomically reduced. Whatever implant is utilized, it is a biomechanical imperative that it provides appropriate compression across the fixation point to facilitate primary bone healing.
4. Implant Selection: Fixation can be achieved using headless metallic compression screws, cannulated screws, or biodegradable pins/screws.
Clinical Warning regarding Bioabsorbables: While biodegradable implants are currently a preferred method of fixation due to the avoidance of hardware removal, surgeons must remain vigilant. Literature indicates that in some cohorts (e.g., a study of 21 knees fixed with bioabsorbable implants), there was a surprisingly low rate of clinical healing coupled with a high rate of complications, including sterile sinus tract formation and foreign body reactions.
The "Matchstick" Bone Peg Technique
An alternative, purely biological method of fixation involves the use of autologous bone pegs. While technically demanding, it avoids the use of synthetic hardware.
* Small "matchstick" grafts are fashioned from a local donor site (e.g., the proximal tibial metaphysis).
* The crater bed is curetted to bleeding cancellous bone, and the OCD fragment is carefully replaced.
* Using an appropriate-size drill, the fragment is perforated to receive two, three, or four matchstick grafts.
* These grafts are gently tapped through the holes in the fragment and into the underlying cancellous bone of the condyle.
* These biological pegs can be used alone for press-fit fixation or supplemented with temporary Kirschner wires.
EXCISION OF LOOSE BODIES
When an OCD fragment completely detaches, it becomes an intra-articular loose body.
Indications for Excision:
* Small fragments (< 2 cm).
* Multiple fragmented pieces.
* Fragments with inadequate bone stock (often purely cartilaginous, lacking the osseous base required for bony union).
* Fragments that cannot be anatomically reduced or secured with internal fixation.
Most loose bodies are currently removed via arthroscopic techniques. However, locating them can be challenging.
Surgical Pitfall: Loose bodies often move freely from one compartment to another when the joint is moved, manipulated, or distended with fluid. Therefore, if an arthrotomy or arthroscopy is planned, radiographs should be made in the operating room after the tourniquet has been applied but before the incision is made. The loose body may have migrated since the preoperative clinic films were taken, necessitating a change in portal placement or surgical approach.
Furthermore, surgeons must remember that some loose bodies may be composed entirely of uncalcified cartilage; therefore, they will not be visible on standard radiographs and require careful arthroscopic exploration of the suprapatellar pouch and posterior gutters.
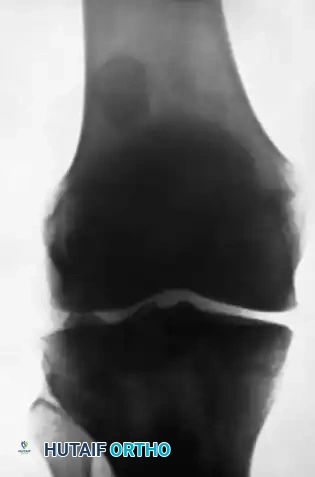
Figures A and B: Lateral and Anteroposterior radiographs demonstrating a large loose body in the lateral portion of the suprapatellar pouch, with a smaller body in the posterolateral compartment. Note: The small fragment of bone opposite the posterior surface of the lateral femoral condyle is the fabella (a normal sesamoid bone in the lateral head of the gastrocnemius muscle), which must not be mistaken for a loose body.
MANAGEMENT OF LARGE AND UNSALVAGEABLE DEFECTS
Treatment of larger lesions (> 2-3 cm) where the fragment is unsalvageable or highly fragmented requires advanced cartilage restoration techniques.
* Osteochondral Autograft Transfer System (OATS): Utilizing cylindrical osteochondral plugs harvested from non-weight-bearing areas of the knee to fill the defect.
* Osteochondral Allografting: Indicated for massive defects where autograft harvest would cause unacceptable donor-site morbidity.
* Autologous Chondrocyte Implantation (ACI): A two-stage procedure involving the harvest, expansion, and reimplantation of the patient's own chondrocytes.
OPEN ARTHROTOMY TECHNIQUES
Although arthroscopic techniques are utilized to treat the vast majority of OCD lesions requiring surgery, open arthrotomy remains a vital tool in the orthopedic surgeon's armamentarium. A well-executed arthrotomy is always preferable to a poorly visualized, inadequate arthroscopic procedure.
Indications for Open Arthrotomy:
* Inability to achieve optimal fixation or trajectory via arthroscopy.
* Lesions involving posterior or extreme peripheral areas inaccessible by standard arthroscopic portals.
* Massive lesions larger than 3 cm requiring multiple structural grafts.
* When complex reshaping and contouring of a large, chronic loose body is required prior to replacement.
* The presence of multiple, salvageable loose fragments requiring a mosaic-style reconstruction.
When required, this can often be accomplished through a minimally invasive "mini-incision" arthrotomy, minimizing disruption to the extensor mechanism.
DIFFERENTIAL DIAGNOSIS: DORSAL DEFECT OF THE PATELLA
When evaluating anterior knee pain and apparent osteochondral lesions, the surgeon must be aware of the dorsal defect of the patella. This is a benign, well-circumscribed radiolucent lesion typically located in the superolateral quadrant of the patella.
Histologically, it is thought to represent a fibrous cortical defect or a nonossifying fibroma of the patella.
* Clinical Course: The lesion is almost always self-limited and heals spontaneously over time.
* Treatment: In patients with symptomatic defects, treatment should be strictly conservative, focusing on the reduction of physical activity and routine radiographic follow-up. Operative treatment (curettage and bone grafting) is exceedingly rare.
* Significance: The most critical aspect of managing a dorsal defect of the patella is accurately differentiating it from true osteochondritis dissecans, ensuring that unnecessary surgical intervention is not performed on a benign, self-limiting condition.
OUTCOMES AND PROGNOSIS
The prognosis following surgical intervention for OCD varies significantly based on the size and location of the lesion, the chronicity of the detachment, and the specific treatment modality employed.
- General Success Rates: Reported results of operative treatment vary considerably among techniques and authors, but generally, good to excellent results are reported in 65% to 95% of patients.
- Mid-Term Outcomes: Follow-up evaluations of knees surgically treated with a variety of methods (debridement, drilling, loose body removal, arthroscopic reduction and internal fixation, microfracture, allograft, ACI) consistently demonstrate significant improvement in all validated outcome measures—including functional scores and symptom relief—at 4-year follow-up.
- Long-Term Outcomes: A comprehensive 6-year follow-up study revealed that, regardless of the specific type of cartilage repair utilized, knee function improved steadily over 5 to 8 years post-surgery. However, it is vital to counsel patients that the functional scores of the operative knee often remain significantly less than those of the healthy, contralateral knee.
COMPLICATIONS
Surgical management of OCD carries inherent risks that must be discussed during the informed consent process.
* General Postoperative Complications: These include standard risks such as surgical site infection, deep vein thrombosis, and postoperative hemarthrosis.
* Hardware Complications: Prominent hardware, migration of pins, or failure of bioabsorbable implants requiring secondary removal.
* Biological Failure: Nonunion of the fixed fragment, fibrous tissue interposition, or progressive avascular necrosis of the fragment.
* Chondral Attrition: If the fragment fails to heal or if the joint surface is left incongruous, the patient is at a high risk for accelerated articular cartilage wear and early-onset osteoarthritis.
Meticulous surgical technique, rigid compression of salvageable fragments, and strict adherence to postoperative rehabilitation protocols are paramount to minimizing these complications and achieving a successful, durable joint preservation.
You Might Also Like