Brachial Plexus Injuries: Comprehensive Diagnosis and Surgical Management

Key Takeaway
Brachial plexus injuries present complex reconstructive challenges, often resulting from high-energy trauma such as motorcycle accidents. Successful management requires precise anatomical localization, differentiating preganglionic from postganglionic lesions. This guide details the etiology, clinical evaluation, advanced electrodiagnostics, and step-by-step surgical interventions—including neurolysis, nerve grafting, and neurotization—aimed at restoring critical upper extremity function, prioritizing elbow flexion and shoulder abduction.
Comprehensive Introduction and Patho-Epidemiology
Brachial plexus injuries represent one of the most devastating and functionally debilitating peripheral nerve injuries encountered in orthopedic and reconstructive surgery, frequently resulting in profound, life-altering impairment of the upper extremity. The etiology of these complex injuries is broadly categorized into high-energy blunt trauma, penetrating injuries, and iatrogenic or birth-related obstetric trauma. The sheer magnitude of kinetic energy required to disrupt the robust neural architecture of the brachial plexus dictates that these injuries are rarely isolated events; they are typically part of a polytrauma presentation requiring a multidisciplinary approach for initial stabilization and definitive management.
In military combat scenarios, penetrating wounds from high-velocity missiles, shrapnel, and blast mechanisms are the predominant cause of brachial plexus trauma. These injuries are characterized by extensive zones of concussive neurapraxia, severe axonotmesis, and unpredictable neurotmesis, often complicated by gross contamination and massive soft-tissue loss. Conversely, in civilian populations, closed traction injuries secondary to high-energy blunt trauma constitute the vast majority of cases. According to the foundational epidemiological principles established by Narakas, commonly referred to as the "Rule of Seven," approximately 70% of traumatic brachial plexus injuries occur secondary to motor vehicle accidents, and of these, roughly 70% involve motorcycles or bicycles. Furthermore, nearly 70% of these patients sustain multiple associated injuries, underscoring the high-energy nature of the mechanism.
The pathomechanics of closed traction injuries strictly dictate the anatomical pattern of neural damage and subsequent clinical presentation. An impact that forcibly depresses the shoulder girdle while simultaneously driving the cervical spine into lateral flexion toward the contralateral side places immense, destructive tensile stress on the upper roots (C5, C6, and occasionally C7). This mechanism frequently results in Erb-Duchenne palsy, characterized by a loss of shoulder abduction, external rotation, and elbow flexion. Conversely, hyperabduction injuries, such as those sustained when a patient attempts to arrest a high-velocity fall by forcibly grasping a stationary object overhead, disproportionately tension the lower roots (C8, T1), leading to Klumpke palsy and profound intrinsic hand dysfunction.
The sheer kinetic energy required to avulse or rupture the brachial plexus frequently results in severe concomitant trauma that can complicate both diagnosis and surgical intervention. Skeletal trauma, including fractures of the proximal humerus, scapula, clavicle, ribs, and cervical transverse processes, is exceedingly common. The presence of a displaced fracture of the first rib or a fracture of the cervical transverse process should immediately raise the index of suspicion for a severe root avulsion. Furthermore, scapulothoracic dissociation—a devastating injury characterized by complete disruption of the scapulothoracic articulation—must be highly suspected in massive traction injuries. Vascular injury, particularly rupture or intimal avulsion of the subclavian or axillary artery, occurs in up to 20% of patients and constitutes an absolute surgical emergency. Concomitant spinal cord injury or traumatic brain injury is reported in a significant subset of patients, while traumatic rotator cuff tears are frequently masked by the overwhelming neurological deficit and must be considered during the comprehensive evaluation.
Detailed Surgical Anatomy and Biomechanics
The surgical anatomy of the brachial plexus is an intricate network of neural elements that demands a profound three-dimensional understanding for successful exploration and reconstruction. The plexus is classically formed by the ventral rami of the fifth through eighth cervical nerve roots (C5-C8) and the first thoracic nerve root (T1). Anatomical variations, such as a prefixed plexus (with significant contribution from C4) or a postfixed plexus (with substantial contribution from T2), occur in approximately 10% to 15% of the population and can alter the expected clinical presentation and intraoperative findings. As the roots exit the intervertebral foramina, they pass between the anterior and middle scalene muscles, a critical anatomical bottleneck where they are vulnerable to compression and scarring.
The architecture of the plexus follows a highly organized, hierarchical progression from proximal to distal: roots, trunks, divisions, cords, and terminal branches. The C5 and C6 roots converge to form the upper trunk; the C7 root continues independently as the middle trunk; and the C8 and T1 roots unite to form the lower trunk. Each trunk subsequently bifurcates into anterior and posterior divisions behind the clavicle, marking the transition from the supraclavicular to the infraclavicular plexus. The anterior divisions of the upper and middle trunks form the lateral cord; the anterior division of the lower trunk continues as the medial cord; and all three posterior divisions coalesce to form the posterior cord. These cords, named for their anatomical relationship to the second part of the axillary artery, ultimately divide into the terminal mixed motor and sensory branches that innervate the upper extremity.
Accurate anatomical classification is paramount for prognostication and the formulation of a rational surgical plan. The most critical distinction lies in determining whether the neural lesion is preganglionic (a root avulsion) or postganglionic (a rupture). Preganglionic injuries occur proximal to the dorsal root ganglion (DRG), representing a true avulsion of the delicate rootlets from the spinal cord. Because the central nervous system lacks robust regenerative capacity and the proximal stump is inaccessible or non-existent, these lesions are irrepairable by direct primary neurorrhaphy or interfascicular grafting. Consequently, preganglionic avulsions necessitate complex nerve transfer (neurotization) procedures utilizing expendable regional or extra-regional donor nerves.

Conversely, postganglionic injuries occur distal to the neural foramen and the DRG. In these scenarios, the neuronal cell bodies remain contiguous with the spinal cord, allowing for Wallerian degeneration to proceed distally while maintaining the theoretical potential for axonal regeneration if anatomical continuity is surgically restored. This restoration can be achieved via meticulous neurolysis, primary end-to-end repair (if tension-free), or, more commonly, interfascicular nerve grafting. Biomechanically, peripheral nerves exhibit viscoelastic properties; they can accommodate up to 8% to 10% elongation before structural failure begins. However, once the elastic limit is exceeded, the internal fascicular architecture ruptures, leading to varying degrees of injury as classified by Seddon (neurapraxia, axonotmesis, neurotmesis) and Sunderland (grades I through V), ultimately culminating in complete mechanical discontinuity and neuroma formation.
Exhaustive Indications and Contraindications
The management algorithm for brachial plexus injuries is highly nuanced, dictated by the mechanism of injury (open versus closed), the precise anatomical level of the lesion, the patient's physiological age, and the temporal progression of neurological recovery. Surgical intervention is rarely a singular event but rather a carefully orchestrated sequence of reconstructive procedures designed to maximize functional independence. The decision to operate must balance the natural history of spontaneous neural recovery against the inexorable, time-dependent degradation of the distal motor endplates, which typically become refractory to reinnervation after 18 to 24 months.
In the setting of open injuries, the indications for immediate surgical exploration are relatively straightforward. Sharp lacerations, such as those sustained from a knife or glass, warrant immediate exploration and primary microsurgical neurorrhaphy, provided the wound is clean and the patient is hemodynamically stable. Conversely, high-velocity missile wounds or severe crush injuries present a more complex clinical dilemma. Immediate neural exploration in these cases is generally contraindicated unless dictated by a concomitant, life-threatening vascular injury. The concussive blast effect and extensive zone of injury cause widespread neurapraxia and axonotmesis that cannot be accurately delineated in the acute setting. A period of clinical observation (typically 3 to 4 weeks) followed by baseline electrophysiological testing is the gold standard.
For closed traction injuries, which represent the overwhelming majority of brachial plexus trauma, expectant management is the initial standard of care. The patient is monitored clinically and electrophysiologically for the first 3 months. Immediate physical therapy is instituted to maintain passive range of motion and prevent debilitating joint contractures. The primary indications for surgical intervention at the 3-to-6-month mark include a complete absence of clinical or electrodiagnostic recovery, an arrested recovery trajectory after initial transient improvement, or the presence of severe, intractable neuropathic pain that is highly characteristic of root avulsions. Furthermore, if advanced imaging and clinical examination unequivocally confirm preganglionic root avulsions, early surgery (at 3 to 4 weeks) is increasingly advocated by specialized centers to perform nerve transfers before irreversible motor endplate fibrosis occurs.
Indications and Contraindications Table
| Parameter | Absolute Indications | Relative Indications | Contraindications |
|---|---|---|---|
| Timing & Mechanism | Clean, sharp open lacerations (Immediate exploration). Concomitant vascular injury requiring repair. | High-velocity missile wounds failing to recover by 3-6 months. Closed traction injuries with no EMG recovery at 3 months. | Immediate exploration of high-velocity gunshot wounds (unless vascular compromise). Exploration of closed injuries < 3 weeks post-injury. |
| Clinical Presentation | Intractable neuropathic pain secondary to confirmed root avulsion (DREZ lesioning or early neurotization). | Arrested neurological recovery after initial partial improvement. | Advanced physiological age with severe medical comorbidities rendering prolonged anesthesia unsafe. |
| Anatomical Findings | Confirmed preganglionic root avulsion (Early nerve transfer). | Postganglionic rupture with a neuroma-in-continuity showing no NAP conduction. | Time elapsed since injury > 18-24 months for direct nerve repair (motor endplates irreversibly degraded). |
| Patient Factors | Motivated patient compliant with rigorous, multi-year rehabilitation protocols. | Partial injuries where the risk of downgrading function via exploration is outweighed by potential gain. | Severe cognitive impairment or psychiatric instability precluding post-operative motor re-education. |
Pre-Operative Planning, Templating, and Patient Positioning
A meticulous, systematic clinical examination forms the absolute foundation of brachial plexus injury diagnosis and subsequent preoperative planning. The surgeon must painstakingly document motor strength grading for every upper extremity muscle group, map sensory deficits across all dermatomes, and assess deep tendon reflexes. The presence of a Horner syndrome (ptosis, miosis, anhidrosis) is a pathognomonic clinical hallmark of a T1 root avulsion, indicating disruption of the sympathetic chain. Similarly, paralysis of the serratus anterior (long thoracic nerve), rhomboids (dorsal scapular nerve), or diaphragm (phrenic nerve) strongly suggests highly proximal, preganglionic injuries at the C5-C7 levels. A positive Tinel's sign in the supraclavicular fossa suggests a postganglionic rupture with a developing neuroma, whereas an absent Tinel's sign in a completely flail arm points toward multi-level root avulsions.
Electrodiagnostic studies, comprising Electromyography (EMG) and Nerve Conduction Studies (NCS), are indispensable but must be timed appropriately. These studies should be delayed until 3 to 4 weeks post-injury to allow for complete Wallerian degeneration to occur; testing prematurely will yield falsely optimistic results as the distal axonal segments may still conduct action potentials. The evaluation of Sensory Nerve Action Potentials (SNAPs) is particularly critical. The preservation of robust SNAPs in a clinically anesthetic dermatome is the electrophysiological hallmark of a preganglionic injury. In this scenario, the sensory cell body residing in the DRG remains intact and viable, supporting the distal axon, but its central connection to the spinal cord has been irrevocably severed. Serial EMGs are utilized to monitor for fibrillation potentials (indicating active denervation) and nascent motor unit potentials (signaling early, subclinical reinnervation).
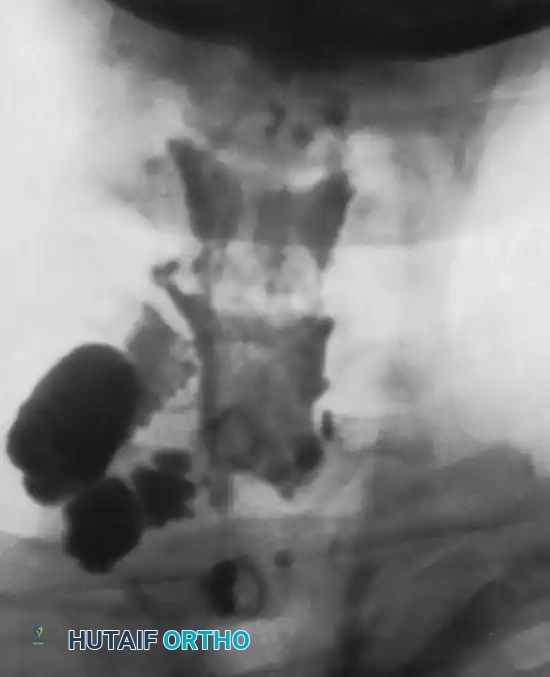
Advanced neuroimaging has revolutionized the preoperative mapping of brachial plexus lesions. Magnetic Resonance Imaging (MRI), specifically high-resolution MR Neurography, and Computed Tomography (CT) Myelography are the contemporary gold standards for evaluating root integrity and guiding the surgical approach. CT Myelography is exquisitely sensitive for detecting pseudomeningoceles—extravasations of intrathecal contrast through an empty, avulsed dural root sleeve—which strongly correlate with preganglionic root avulsions. MRI provides superior soft-tissue contrast, making it excellent for visualizing postganglionic neuromas, periplexus scarring, edema within the denervated musculature, and the anatomical continuity of the extraforaminal trunks and cords.
Preoperative templating involves synthesizing the clinical, electrodiagnostic, and imaging data to formulate a primary surgical strategy and multiple contingency plans. Patient positioning is a critical component of the operative setup. The patient is positioned supine on a radiolucent table with a gel bump placed horizontally under the ipsilateral scapula to elevate the shoulder girdle. The head is turned approximately 45 degrees to the contralateral side to maximize exposure of the posterior triangle of the neck. The entire ipsilateral upper extremity, the neck up to the mandible, the hemithorax, and both lower extremities (circumferentially prepped for sural nerve graft harvesting) are prepped and draped free. Crucially, the anesthesia team must be explicitly instructed to avoid all long-acting paralytic agents and neuromuscular blockade, as direct intraoperative nerve stimulation is mandatory for decision-making.
Step-by-Step Surgical Approach and Fixation Technique
Surgical exploration and reconstruction of the brachial plexus is a formidable undertaking that requires mastery of complex regional anatomy, microsurgical techniques, and intraoperative neurophysiology. Reconstruction of the completely flail upper extremity requires a highly pragmatic approach; the surgeon and patient must accept that restoring normal, pre-injury function is biologically impossible. The internationally accepted hierarchy of surgical priorities dictates the operative sequence: (1) Restoration of elbow flexion, which is the absolute primary goal, allowing the hand to be brought to the mouth or workspace; (2) Restoration of shoulder abduction and external rotation to provide a stable proximal platform and prevent inferior glenohumeral subluxation; (3) Restoration of protective sensation, specifically to the median nerve distribution (thumb and index finger); and (4) Restoration of wrist and finger flexion, which often requires delayed free functioning muscle transfers (FFMT) in pan-plexus injuries.
The Supraclavicular Approach is utilized to expose the roots, trunks, and proximal divisions. A generous zigzag or L-shaped incision is made along the posterior border of the sternocleidomastoid (SCM) muscle, extending laterally parallel to the superior border of the clavicle. The platysma is sharply divided, and the external jugular vein and supraclavicular sensory nerves are identified, mobilized, and preserved if possible. Deep dissection proceeds by identifying and dividing the omohyoid muscle. The transverse cervical and suprascapular vessels frequently traverse the operative field and must be meticulously ligated and divided to prevent catastrophic hemorrhage and to allow unhindered access to the neural elements. The anterior scalene muscle serves as the critical deep anatomical landmark. The phrenic nerve is identified coursing obliquely from lateral to medial across the anterior surface of the anterior scalene; it must be neurolysed and protected at all costs. The C5, C6, and C7 roots are then identified emerging from the interscalene triangle between the anterior and middle scalene muscles, and dissection proceeds distally to trace the trunks.
The Infraclavicular Approach is required for exposure of the cords and terminal branches, and is often performed in conjunction with the supraclavicular exposure for pan-plexus injuries. The incision extends from the supraclavicular incision, crossing the clavicle directly (clavicular osteotomy is historically described but rarely required with modern retraction techniques), and follows the deltopectoral groove distally. The cephalic vein is identified and retracted laterally with the deltoid. The pectoralis major muscle is retracted medially, and the pectoralis minor muscle is routinely tenotomized at its insertion on the coracoid process to widely expose the neurovascular bundle. The lateral, posterior, and medial cords are systematically identified based on their relationship to the axillary artery and traced distally to their terminal branches.

Intraoperative Neurophysiology and Interfascicular Grafting: Once the zone of injury is exposed, direct intraoperative nerve stimulation and the recording of Nerve Action Potentials (NAPs) across the lesion are mandatory. If a NAP is successfully conducted across a neuroma-in-continuity, it signifies that a critical mass of internal fascicular architecture remains intact, and simple external neurolysis is indicated. Conversely, if no NAP is recorded, the lesion represents a severe axonotmesis or neurotmesis. The dense, scarred neuroma must be sharply resected back to healthy, viable fascicles—evidenced microscopically by the "mushrooming" or pouting of healthy axoplasm from the cut nerve ends. When a postganglionic rupture is resected, the resulting defect cannot be closed under tension. Autologous interfascicular nerve grafting is required. The sural nerve is the standard donor, providing up to 40 cm of graft material per leg. The grafts are reversed (to minimize axonal loss out of distal branches), interposed between the proximal and distal nerve stumps, and meticulously secured using 9-0 or 10-0 nylon epineurial sutures supplemented with fibrin glue under high-power microscopic magnification.
Neurotization (Nerve Transfers): In the setting of preganglionic root avulsions, no viable proximal stump is available for grafting. The paradigm shifts to neurotization, where expendable, healthy donor nerves are transected and transferred directly to critical, denervated distal motor nerves as close to the target muscle as possible. This proximity drastically reduces the required regeneration distance and time. For the restoration of elbow flexion, the Oberlin transfer is the gold standard; it involves transferring expendable motor fascicles from the ulnar nerve (typically those supplying the flexor carpi ulnaris) directly to the biceps motor branch of the musculocutaneous nerve. Alternatively, T3-T5 intercostal nerves can be harvested and coapted to the musculocutaneous nerve. For shoulder abduction, common transfers include the Spinal Accessory Nerve (CN XI) to the suprascapular nerve (restoring supraspinatus and infraspinatus function while preserving upper trapezius innervation) and the Somsak transfer, which utilizes triceps motor branches from the radial nerve to reinnervate the axillary nerve for deltoid function.
Complications, Incidence Rates, and Salvage Management
Surgical reconstruction of the brachial plexus is fraught with potential pitfalls, and even perfectly executed operations can yield suboptimal functional outcomes due to the inherent biological limitations of peripheral nerve regeneration. The profound distance between the cervical spinal cord and the intrinsic muscles of the hand means that regenerating axons—traveling at an average rate of 1 mm per day—often fail to reach their distal targets before irreversible fibrosis of the motor endplates occurs. Consequently, the failure of nerve regeneration remains the most significant long-term complication, necessitating a robust algorithm for salvage management.
Neuropathic pain is a devastating complication, particularly prevalent in patients with lower root (C8, T1) avulsions. The deafferentation of the spinal cord leads to hyperactive firing of the dorsal horn neurons, resulting in severe, burning, intractable pain that is often refractory to standard pharmacological management (gabapentinoids, tricyclic antidepressants, and opioids). In cases where neuropathic pain dominates the clinical picture and fails to respond to conservative measures, neurosurgical intervention via Dorsal Root Entry Zone (DREZ) lesioning may be required to ablate the hyperactive nociceptive pathways.
Joint contractures and secondary musculoskeletal deformities are ubiquitous in the paralyzed limb. Glenohumeral adhesive capsulitis, elbow flexion contractures, and severe supination or pronation deformities of the forearm can render even successfully reinnervated muscles functionally useless. Meticulous, lifelong physical therapy is required. When primary nerve reconstruction fails to yield adequate functional recovery by 18 to 24 months, secondary palliative procedures must be employed. These include complex tendon transfers (e.g., the Steindler flexorplasty for elbow flexion), free functioning muscle transfers (FFMT, such as a microvascular Gracilis flap innervated by the spinal accessory or intercostal nerves), and strategic joint arthrodesis (such as shoulder or wrist fusion) to provide a stable mechanical platform and maximize the patient's residual independence.
Complications and Salvage Management Table
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Palliative Strategy |
|---|---|---|---|
| Failure of Nerve Regeneration | 20% - 40% (varies by injury severity) | Prolonged denervation time (>12-18 months), extensive scar bed, advanced patient age. | Free Functioning Muscle Transfer (FFMT - e.g., Gracilis), Tendon transfers (Steindler flexorplasty), Arthrodesis. |
| Intractable Neuropathic Pain | 30% - 50% (highest in root avulsions) | Deafferentation of the spinal cord, particularly C8/T1 root avulsions. | Multimodal pharmacotherapy; Neurosurgical Dorsal Root Entry Zone (DREZ) lesioning for refractory cases. |
| Severe Joint Contractures | 40% - 60% | Lack of early passive range of motion, prolonged immobilization post-operatively. | Aggressive physical therapy, serial casting, surgical capsular release, or corrective osteotomies. |
| Donor Site Morbidity | 10% - 15% | Sural nerve harvest (sensory loss/neuroma); Intercostal harvest (pleural tear/atelectasis). | Conservative management for sensory deficits; chest tube thoracostomy for iatrogenic pneumothorax. |
Phased Post-Operative Rehabilitation Protocols
Surgical reconstruction of the brachial plexus is only the beginning of a protracted, arduous recovery process that requires immense psychological resilience from the patient and unwavering dedication from the rehabilitation team. Because peripheral axons regenerate at a maximum rate of approximately 1 mm per day (roughly 1 inch per month), clinical evidence of motor recovery may not manifest for 9 to 18 months following a proximal reconstruction. The post-operative rehabilitation protocol is meticulously phased to protect the fragile microvascular nerve coaptations initially, maintain joint suppleness during the prolonged denervation period, and ultimately facilitate profound cortical remapping.
Phase I: Immobilization and Protection (Weeks 0-4). Immediately postoperatively, the affected upper extremity and the cervical spine are rigidly immobilized in a custom orthosis or a specialized sling. The primary objective during this phase is to strictly prevent any tensile stress or shearing forces across the delicate interfascicular nerve grafts and micro-sutured nerve transfers. The head and neck are maintained in a neutral or slightly ipsilaterally flexed position. During this period, rehabilitation is limited to active range of motion of the uninvolved joints (e.g., the contralateral limb and lower extremities) to prevent generalized deconditioning.
Phase II: Passive Range of Motion and Joint Preservation (Weeks 4 to Reinnervation). Once the microvascular coaptations have achieved sufficient tensile strength (typically around 4 weeks), the immobilization is discontinued, and a rigorous regimen of Passive Range of Motion (PROM) is initiated. The paralyzed limb is highly susceptible to rapid, severe joint contractures, particularly glenohumeral adhesive capsulitis and elbow flexion or extension contractures. Therapists and caregivers are instructed to perform daily PROM exercises encompassing all planes of motion. Edema control via compression garments and retrograde massage is also critical during this phase to prevent fibrotic induration of the soft tissues.
Phase III: Biofeedback, Motor Re-education, and Cortical Remapping (Onset of Reinnervation to 24+ Months). As regenerating axons begin to reach their target motor endplates, patients will exhibit nascent, often imperceptible muscle twitches. This marks the initiation of the most challenging phase: motor re-education. Because nerve transfers utilize donor nerves that originally controlled entirely different functions, the patient's brain must undergo intensive cortical plasticity. For example, a patient who has undergone an intercostal nerve transfer to the musculocutaneous nerve must consciously learn to take deep, forceful breaths to initiate elbow flexion. Surface electromyography (sEMG) and visual biofeedback are extensively utilized to help the patient isolate and amplify these novel motor signals. Over months to years of repetitive practice, cortical remapping allows these movements to become increasingly independent and subconscious.
Summary of Landmark Literature and Clinical Guidelines
The evolution of brachial plexus surgery from an era of therapeutic nihilism to the modern epoch of advanced microsurgical reconstruction is built upon a foundation of landmark anatomical studies and pioneering clinical trials. The epidemiological and prognostic framework utilized globally today remains heavily reliant on the seminal works of Algimantas Narakas in the 1980s, whose "Rule of Seven" and classification systems for traction injuries provided the first standardized language for comparing outcomes across institutions. Furthermore, the foundational classifications of nerve injury pathophysiology described by Seddon (1943) and Sunderland (1951) remain the absolute bedrock of peripheral nerve surgery.
The paradigm shift toward early neurotization for root avulsions was catalyzed by Christophe Oberlin's landmark 1994 publication detailing the transfer of ulnar nerve fascicles to the biceps motor branch. This technique revolutionized the restoration of elbow flexion, demonstrating superior, faster, and more reliable outcomes compared to traditional, lengthy interfascicular grafting from the neck. Subsequent advancements by pioneers such as Susan Mackinnon and David Chuang have vastly expanded the repertoire of nerve transfers, introducing techniques like the double fascicular transfer (Oberlin II) and complex free functioning muscle transfers for pan-plexus avulsions.
Current consensus guidelines, supported by the American Academy of Orthopaedic Surgeons (AAOS) and international peripheral nerve societies, strongly advocate for a multidisciplinary approach. The contemporary standard of care dictates early referral to specialized tertiary centers. While closed traction injuries are generally observed for 3 months, there is a growing, evidence-based consensus that isolated, radiographically confirmed preganglionic root avulsions should undergo early nerve transfer surgery (within 4 to 8 weeks) to bypass the lengthy regeneration distances and capitalize on pristine distal motor endplates, thereby maximizing the ultimate functional ceiling of the reconstructed limb.
