Operative Management of Femoral Shaft Fractures: A Comprehensive Surgical Guide
Key Takeaway
Femoral shaft fractures are high-energy injuries requiring meticulous surgical management to restore lower extremity biomechanics. Interlocking intramedullary nailing remains the gold standard, offering superior biomechanical stability and high union rates. This guide details the indications, surgical approaches, and postoperative protocols for intramedullary nailing, plate osteosynthesis, and external fixation, providing orthopedic surgeons with an evidence-based framework for optimizing patient outcomes and minimizing complications.
Introduction to Femoral Shaft Fractures
Fractures of the shaft of the femur are among the most common and significant fractures encountered in acute orthopaedic trauma practice. Because the femur is the largest bone in the human body and the principal load-bearing structure of the lower extremity, fractures here can cause prolonged morbidity, massive hemorrhage, and extensive disability unless treatment is prompt and biomechanically appropriate.
Femoral shaft fractures are predominantly the result of high-energy trauma—such as motor vehicle collisions, motorcycle accidents, and falls from height—and are frequently associated with multiple system injuries, including closed head injuries, blunt chest trauma, and abdominal visceral injuries. Consequently, the orthopaedic surgeon must approach these fractures not merely as isolated osseous disruptions, but as critical components of the polytraumatized patient.
Several techniques are currently available for the treatment of femoral shaft fractures. The operating surgeon must be intimately aware of the advantages, disadvantages, biomechanical principles, and limitations of each modality to select the optimal treatment. Factors influencing the method of treatment include the type and location of the fracture, the degree of comminution (AO/OTA classification), the patient’s age, hemodynamic stability, and functional demands.
Regardless of the treatment method chosen, the following universal principles of femoral fracture management must be achieved:
1. Restoration of Anatomy: Precise restoration of alignment, rotation, and length.
2. Biological Preservation: Preservation of the endosteal and periosteal blood supply to aid union and prevent infection.
3. Functional Recovery: Early, aggressive rehabilitation of the extremity and the patient.
Deforming Forces and Biomechanics
Understanding the muscular anatomy of the thigh is critical for achieving and maintaining reduction. The femur is surrounded by large, powerful muscle groups that exert massive angular and translational forces on fracture fragments:
* Proximal Third Fractures: The proximal fragment is typically flexed (by the iliopsoas), abducted (by the gluteus medius and minimus), and externally rotated (by the short external rotators).
* Middle Third Fractures: Deformity depends on the exact level relative to the adductor insertion, often resulting in varus or valgus angulation.
* Distal Third Fractures: The distal fragment is characteristically pulled into recurvatum (extension) by the strong origin of the gastrocnemius muscle, complicating guide wire passage during intramedullary nailing.

Treatment Modalities
Traction and Cast Immobilization
Historically, skeletal traction followed by spica cast immobilization was a mainstay of treatment. Today, a femoral shaft fracture in an adult can rarely be reduced and held definitively in plaster. In contrast to its utility in pediatric orthopaedics, plaster immobilization early after a femur fracture in an adult almost universally leads to displacement, angulation, unacceptable shortening, and profound joint stiffness.
Surgical Warning: The length of confinement to bed required for definitive traction, combined with the high risk of deep vein thrombosis (DVT), pulmonary embolism, decubitus ulcers, and pulmonary compromise, makes this an impractical and dangerous definitive method in modern adult trauma care.
Skeletal traction (typically via a proximal tibial pin) is now primarily utilized as a preliminary, temporizing phase prior to definitive surgical management. A period of preliminary traction distracts the fracture, overcomes muscle spasm, and aligns the fragments, significantly easing subsequent closed intramedullary nailing.
External Fixation
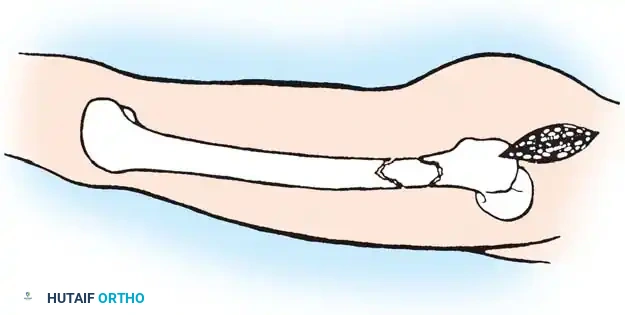
While immediate débridement, irrigation, and interlocking intramedullary nailing remain the gold standard for most open femoral shaft fractures, external fixation is a critical tool in specific clinical scenarios. Half-pin fixators are highly effective for:
* Massively contaminated open fractures (Gustilo-Anderson Type IIIB/IIIC).
* Fractures requiring rapid stabilization for concomitant vascular repair.
* "Damage Control Orthopaedics" (DCO) in hemodynamically unstable, severely injured polytrauma patients.
* Patients where further blood loss is a critical concern (e.g., Jehovah’s Witnesses).
Most frequently, an anterior spanning fixation frame is applied to provide rapid immobilization across the joint. A six-pin uniplanar or multiplanar frame is used laterally; ring fixation with thin wires in a multiplanar configuration can also be utilized.
Clinical Pearl: If external fixation is used temporarily, early conversion (within 14 days) to intramedullary fixation is recommended. Prolonged external fixation increases pin-tract colonization, significantly elevating the risk of deep infection upon conversion to an intramedullary nail.
Intramedullary Nailing (The Gold Standard)
Internal fixation of femoral shaft fractures revolutionized trauma care following World War II with the introduction of the Küntscher nail. Today, interlocking intramedullary (IM) nailing is universally considered the treatment of choice for the vast majority of femoral shaft fractures.
In a young adult patient with a fracture through the isthmus of the medullary canal, a reamed, locked IM nail provides the ultimate biomechanical construct. It acts as a load-sharing device, allowing for early weight-bearing, a short hospital stay, rapid return of joint motion, and a high rate of union.

Closed vs. Open Technique
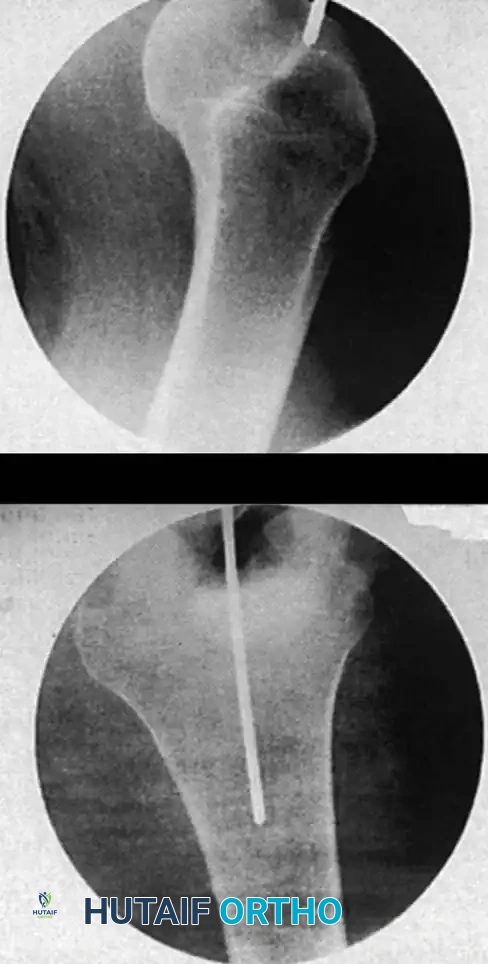
With the advent of high-quality fluoroscopic image intensifiers, closed nailing techniques have almost entirely replaced open nailing. Closed nailing preserves the fracture hematoma (rich in osteogenic factors) and minimizes disruption of the periosteal blood supply, drastically reducing the risk of infection and nonunion compared to open techniques.
Reamed vs. Unreamed
Reaming the medullary canal offers several advantages: it allows for the insertion of a larger diameter, biomechanically stronger nail; it increases the contact area between the nail and the endosteum; and the reamings themselves act as an autologous bone graft at the fracture site.
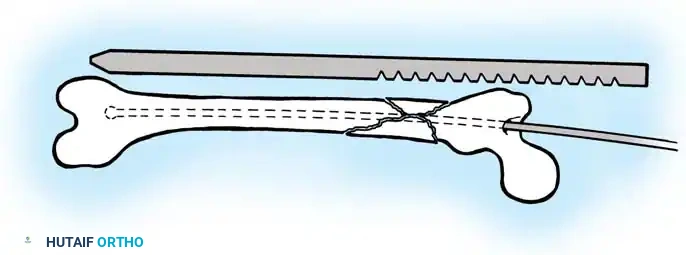
Surgical Technique: Antegrade Interlocking Intramedullary Nailing
Preoperative Planning and Positioning
Careful preoperative planning includes measuring the contralateral intact femur on full-length radiographs to determine the estimated nail length and diameter.
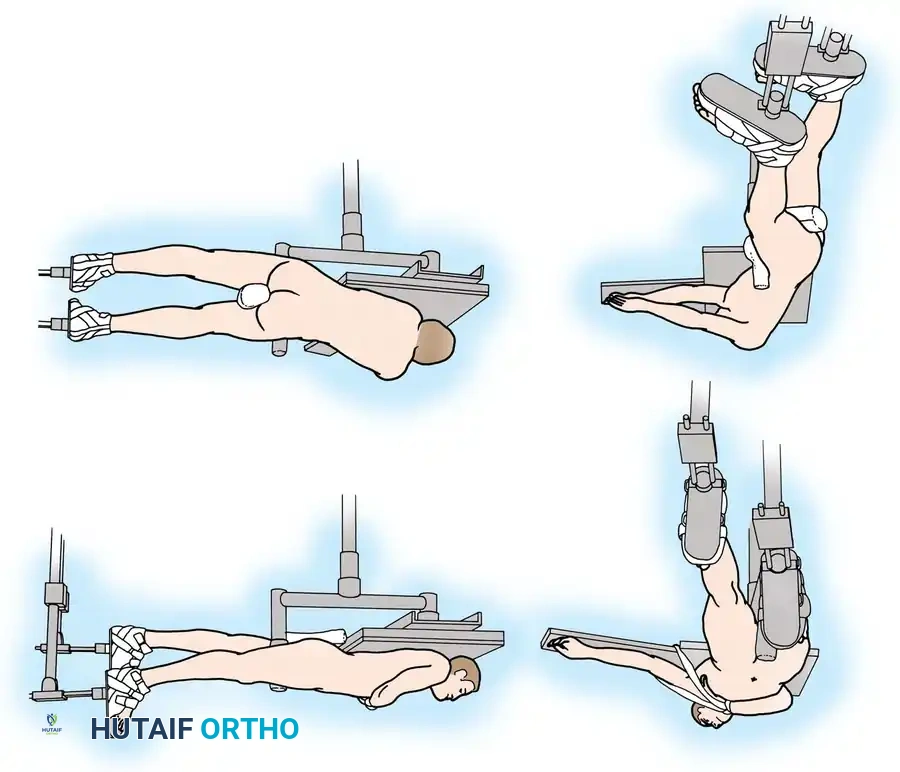
The patient may be positioned supine or in the lateral decubitus position on a radiolucent fracture table. The supine position is generally preferred for polytrauma patients as it allows simultaneous access to the airway, chest, and abdomen, and facilitates concurrent procedures.
- Traction Setup: Apply skeletal traction via a distal femoral or proximal tibial pin, or use a fracture boot. Ensure the perineal post is well-padded.
- Reduction: Achieve closed reduction using longitudinal traction, rotation, and manipulation. Fluoroscopy is used to confirm alignment in both the anteroposterior (AP) and lateral planes.
Pitfall: Avoid excessive traction against the perineal post, as this can cause devastating pudendal nerve damage or perineal skin sloughing.
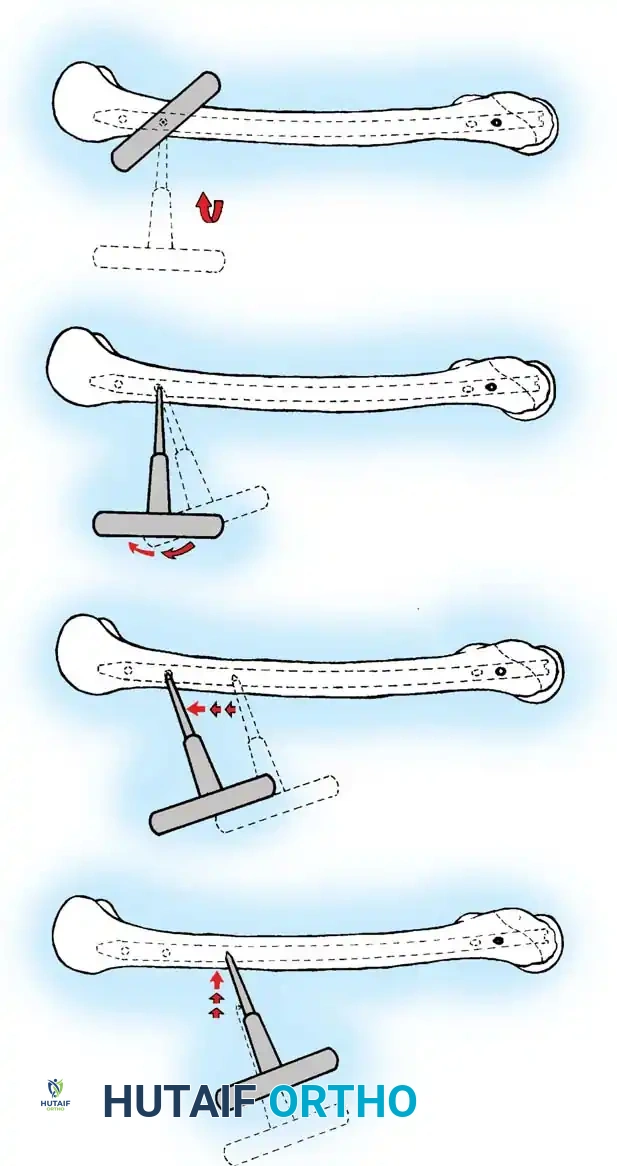
Entry Point and Guide Wire Placement
The choice of entry point—piriformis fossa versus greater trochanter—depends on the specific nail design.
1. Make a longitudinal incision proximal to the greater trochanter.
2. Split the gluteus maximus fascia and bluntly dissect to the starting point.
3. Insert a guide pin or awl. For a piriformis entry, the starting point is in the piriformis fossa, slightly posterior to the central axis of the femoral neck on the lateral view.
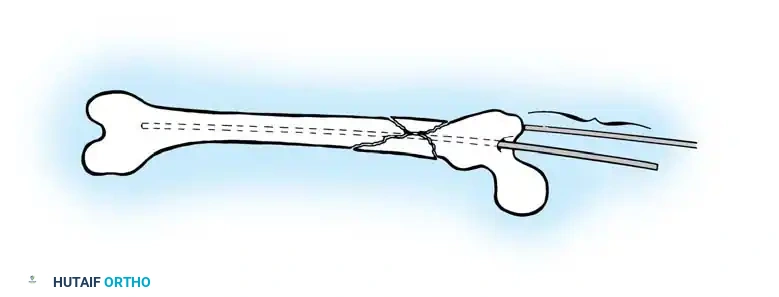
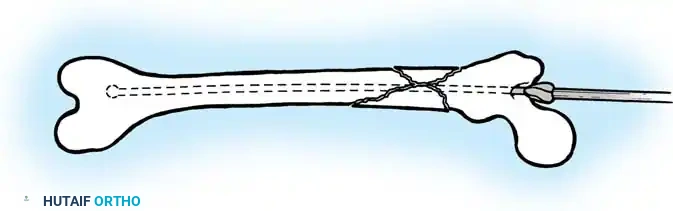
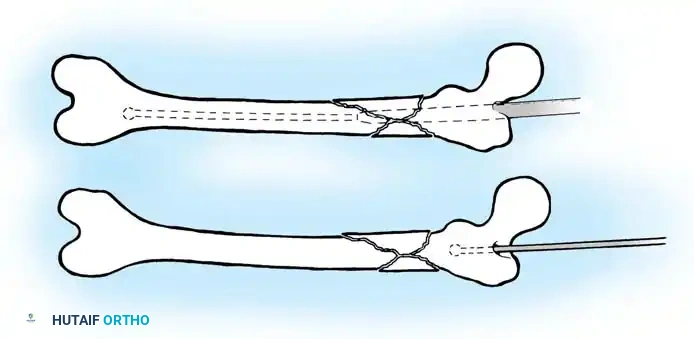
4. Pass a ball-tipped guide wire down the proximal fragment, across the reduced fracture site, and into the distal metaphysis, centering it in the intercondylar notch.
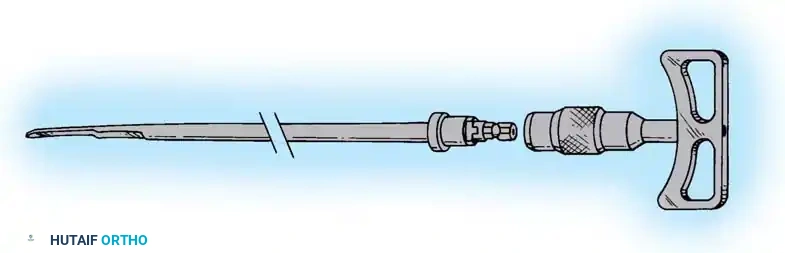
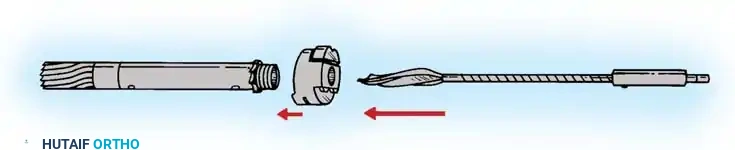
Reaming and Nail Insertion
- Determine the required nail length by measuring the remaining exposed guide wire against a second wire of identical length.
- Sequentially ream the medullary canal over the ball-tipped guide wire in 0.5 mm increments until cortical chatter is felt. Over-ream by 1.0 to 1.5 mm larger than the selected nail diameter.
- Exchange the ball-tipped wire for a smooth driving wire if required by the nail system.
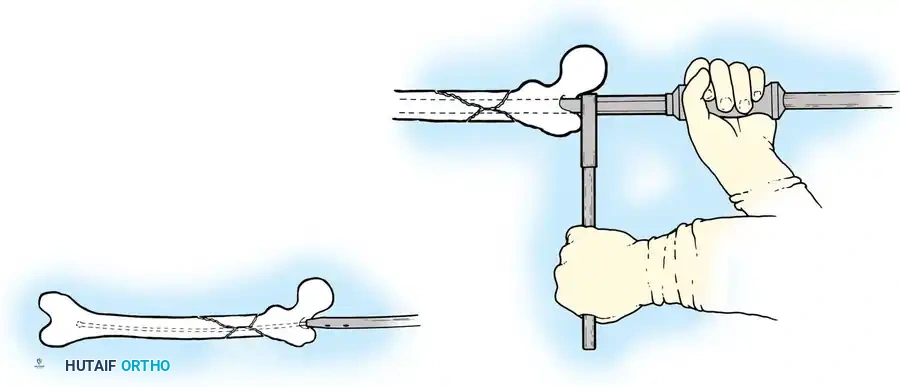
- Mount the selected interlocking nail on the insertion jig and advance it manually or with gentle mallet strikes.
Distal and Proximal Locking
Locking the nail prevents shortening and rotational malalignment, which is especially critical in comminuted (AO Type B and C) fractures.
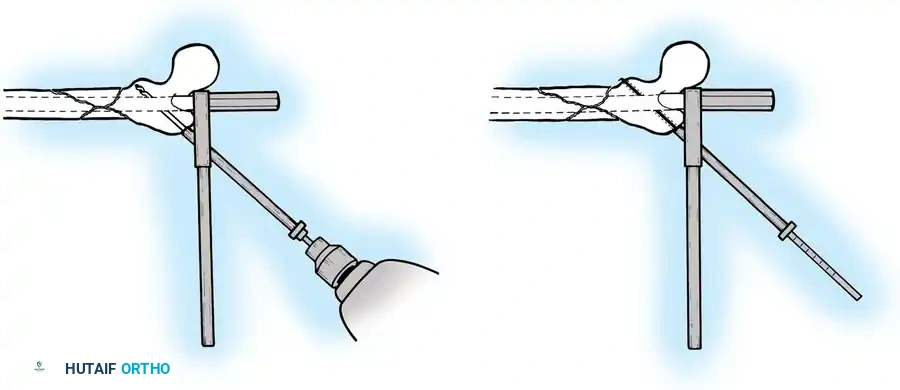
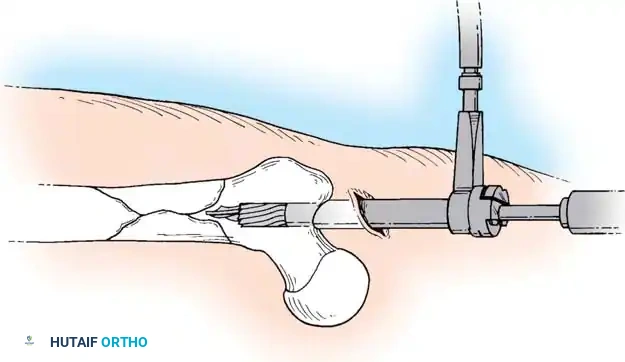
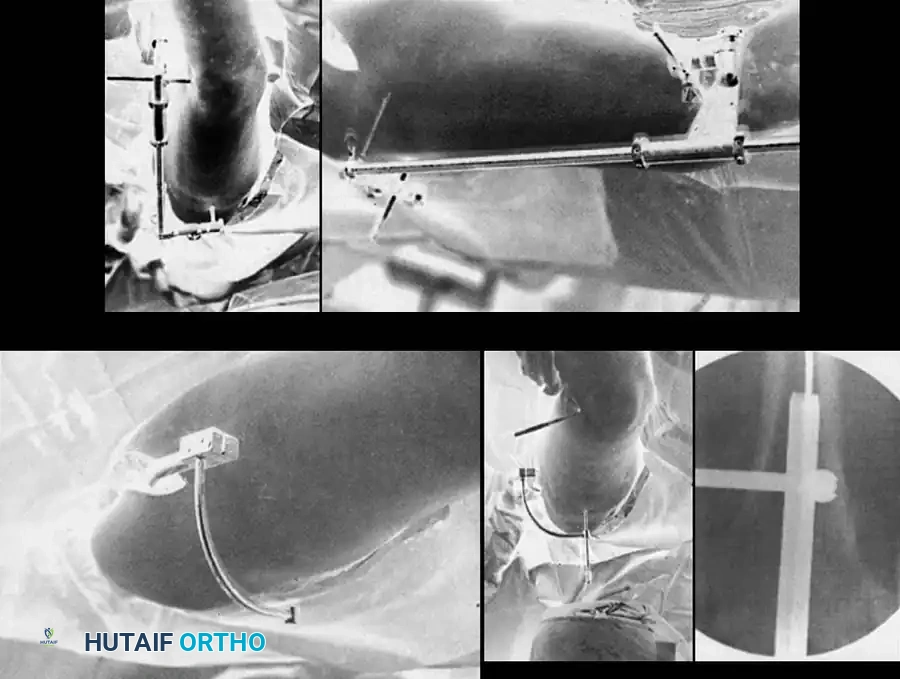
Distal Locking (Perfect Circle Technique):
* Align the C-arm perfectly perpendicular to the nail so the distal locking hole appears as a "perfect circle" rather than an ellipse.
* Make a stab incision directly over the hole.
* Using a radiolucent drill drive, advance the drill bit directly down the path of the fluoroscopic beam through the near cortex, through the nail hole, and out the far cortex.
* Measure the depth and insert the appropriate locking screw.
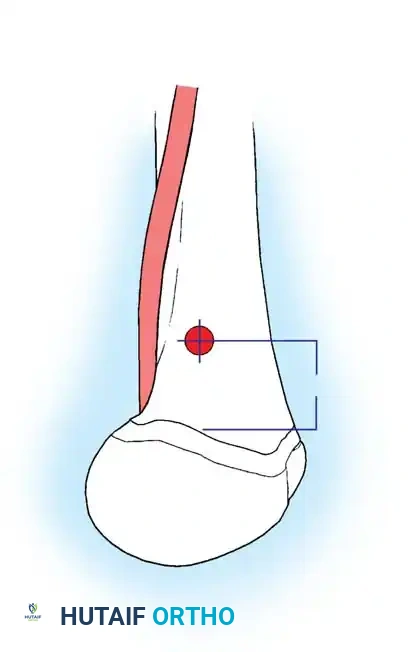
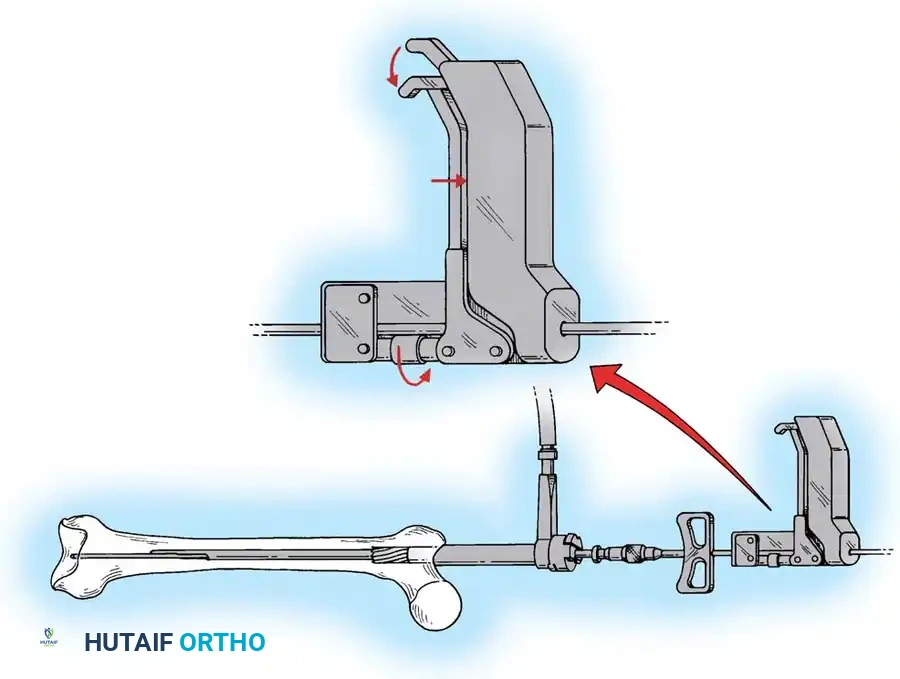
Proximal Locking & Final Checks:
* Move to the proximal locking hole. This should be placed in the anteroposterior plane at the level of the lesser trochanter to avoid neurovascular injury.
* Make a stab wound in the skin, and bluntly dissect to bone. Avoid damage to the branches of the femoral nerve.
* Use a gold tissue-protection tube with a silver insert to protect the muscle and nerve branches.
* Drill into the femur when the position is acceptable by the perfect circle technique.
* Hold the guide steady, remove the insert, and place the 5-mm screw using the capturing screwdriver.
Intraoperative Alignment Verification
- Recheck the alignment and length of the femur using a Bovie cord (cable method) stretched from the anterior superior iliac spine (ASIS), over the middle of the patella, to the middle of the tibial plafond.
- Check the lateral reduction. Use blocking screws (Poller screws) as necessary to correct angular malalignment.
- CRITICAL STEP: Image the hip in full fluoroscopic mode with internal and external rotation and push-pull maneuvers to check for an occult femoral neck fracture.
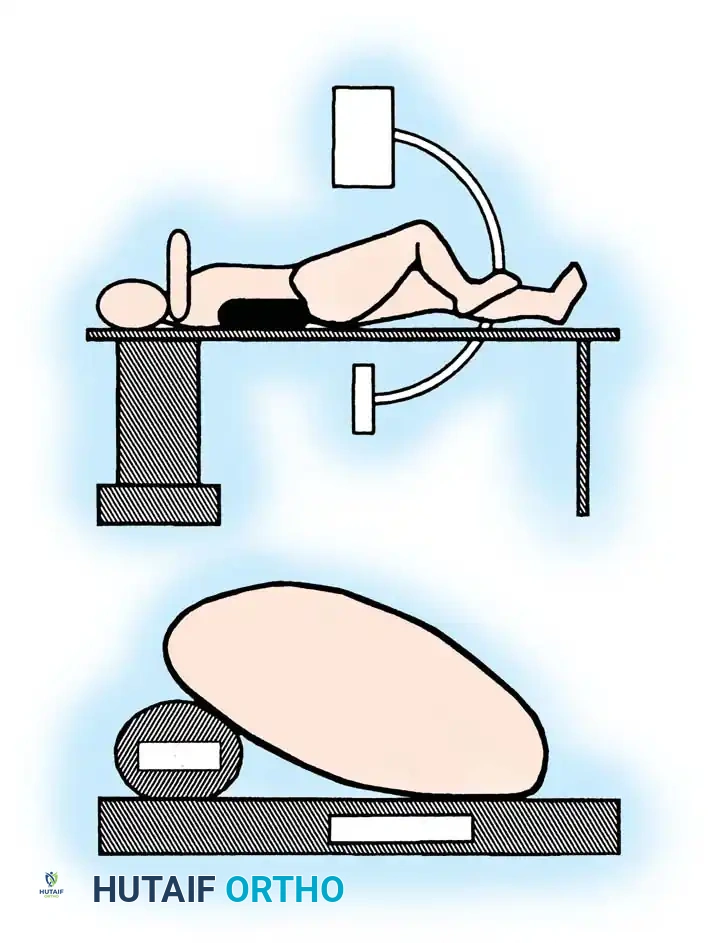
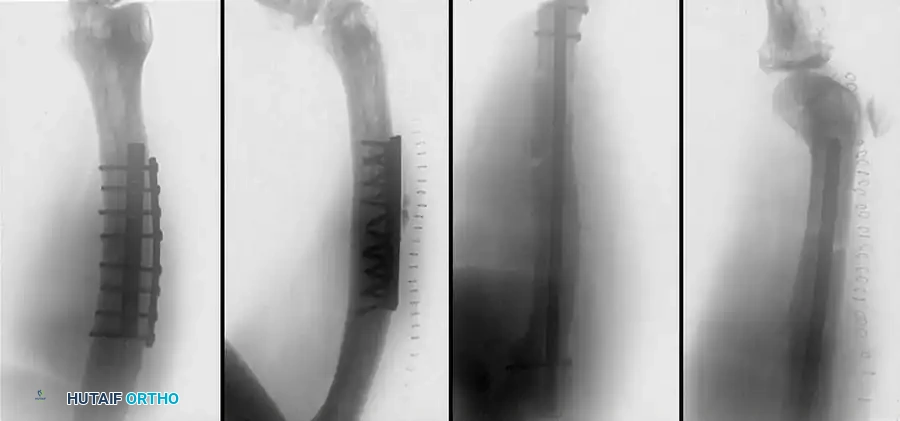
Plate Osteosynthesis
While IM nailing is the standard, plate and screw fixation remains a vital technique for specific indications, including fractures with severe periarticular extension, extremely narrow medullary canals, or in polytrauma patients where the pulmonary burden of reaming is contraindicated.

Fig. 51-91 Femoral shaft fracture stabilized with plate and interfragmentary screws.
AO Principles and Clinical Outcomes
Since the 1960s, AO surgeons have utilized compression plate fixation. The most accurate anatomical reduction of comminuted fractures can be obtained with interfragmentary lag screws and neutralization plating. However, historical open plating techniques required massive soft-tissue stripping, leading to unacceptable rates of infection and implant failure.
Rüedi and Lüscher reported on 131 comminuted fractures fixed with AO plates, noting a 92% good functional result, but highlighted complications such as plate bending, refracture, and osteitis. They historically recommended routine medial bone grafting. Magerl et al. similarly noted that complications were excessive if rigid internal fixation with interfragmentary compression was not perfectly achieved.
Modern Biological Plating (MIPO)
Modern plating techniques emphasize biology over absolute mechanical rigidity. Mast and others proposed indirect reduction of intermediate fragments, preservation of medial soft-tissue attachments, and bridge plating. Most femoral shaft fractures treated with indirect reduction heal with robust secondary callus formation rather than primary cortical healing.
Riemer et al. demonstrated excellent results using indirect reduction and posterolateral plate application without medial bone grafting in blunt polytrauma patients. In their series of 141 fractures, the average time to union was 18 weeks, with a 99% return of full knee extension.
If plate fixation is indicated, a broad Low-Contact Dynamic Compression Plate (LC-DCP) or Locking Compression Plate (LCP) should be used. The scalloped undersurface of modern plates preserves periosteal blood supply. Generally, a minimum of eight cortical screws (four bicortical screws) should be placed on either side of a transverse fracture.
Associated Injuries and Complications
Occult Femoral Neck Fractures
Approximately 2% to 9% of femoral shaft fractures are associated with an ipsilateral femoral neck fracture. These are frequently non-displaced and easily missed on initial trauma radiographs. A dedicated AP internal rotation view of the hip and intraoperative fluoroscopic stress views are mandatory. Missed femoral neck fractures can lead to devastating avascular necrosis (AVN) or nonunion.
Knee Ligamentous Injuries
The high-energy nature of femoral shaft fractures frequently results in concomitant knee ligament injuries. We recommend that all ipsilateral knees be examined under anesthesia immediately after fracture fixation.
Walling et al. noted a 33% incidence of knee ligament injury by manual examination. De Campos et al. arthroscopically examined 30 knees immediately after IM nailing and found a 52% incidence of laxity, including partial and complete tears of the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), and meniscal tears.
Postoperative Rehabilitation
Postoperative rehabilitation depends heavily on the stability of the fixation, the fracture pattern, and the patient's overall polytrauma status. Protocols must be individualized.


📚 Medical References
- femoral shaft fractures, Clin Orthop Relat Res 296:168, 1993.
- Blair W, Hansen C: Traumatic closure of triradiate cartilage, J Bone Joint Surg 61A:144, 1979.
- Boitzy A: Fractures of the proximal femur. In Weber BG, Brunner C, Freuler F, eds: Treatment of fractures in children and adolescents, New York, 1980, Springer-Verlag. Bond SJ, Gotschall CS, Eichelberger MR: Predictors of abdominal injury in children with pelvic fracture, J Trauma 31:1169, 1991.
- Bos CFA, Eulderink F, Bloem JL: Bilateral pelvitrochanteric heterotopic ossifi cation in a child: a case report, J Bone Joint Surg 75A:1840, 1993.
- Brooks E, Rosman M: Central fracture dislocation of the hip in the child, J Trauma 28:1590, 1988.
- Bryan WJ, Tullos HS:
You Might Also Like
