Optimizing Retrograde Nailing for Challenging Femur Fractures

Key Takeaway
This topic focuses on Optimizing Retrograde Nailing for Challenging Femur Fractures, Retrograde femoral nailing is a surgical technique for treating femur fractures retrograde. It is defined as any femoral nailing method with a distal entry point from the condyles or an intercondylar, intra-articular starting point. For full-length nails, this involves an intercondylar start extending through the shaft to the proximal femur, while shortened nails can fix distal fractures.
As a highly respected academic orthopedic surgeon and medical educator, I am pleased to present this comprehensive review on optimizing retrograde nailing for challenging femur fractures. This guide aims to provide a high-yield reference for orthopedic surgeons, residents, and medical students, emphasizing scientific rigor and clinical applicability.
Introduction and Epidemiology
Intramedullary nailing has long been established as the gold standard for diaphyseal femur fractures due offering superior biomechanical stability and promoting early mobilization compared to external fixation or plate osteosynthesis. While antegrade nailing remains the predominant technique, retrograde intramedullary nailing (RIMN) has gained significant acceptance and expanded indications, particularly for complex and polytrauma patients. Its evolution stems from a need for alternative fixation strategies when antegrade access is challenging or contraindicated, or when concomitant injuries demand a less invasive approach to the proximal femur.
Femoral shaft fractures account for approximately 1-2% of all adult fractures, with a bimodal distribution affecting young adults involved in high-energy trauma and the elderly due to low-energy falls. Distal femur fractures, including supracondylar and intercondylar patterns, represent about 4-7% of all femoral fractures. RIMN offers a versatile solution for a significant subset of these injuries, especially in the setting of polytrauma, ipsilateral lower extremity injuries (e.g., floating knee), pelvic or acetabular fractures, spinal injuries requiring supine positioning, and in patients with morbid obesity where antegrade positioning can be problematic. The growing body of literature supports RIMN as a safe and effective method, demonstrating comparable union rates and complication profiles to antegrade techniques in appropriately selected cases, while offering distinct advantages in specific clinical scenarios.
Surgical Anatomy and Biomechanics
Definition of Retrograde Femoral Nailing
Retrograde femoral nailing can be precisely defined as any femoral nailing technique utilizing a distal entry point from the condyles or through an intercondylar, intra-articular starting point. For the purpose of this review, retrograde femoral nailing will specifically refer to nails that originate from an intercondylar starting point and extend through the femoral shaft region to achieve fixation in the proximal femur. In specific fracture patterns, such as isolated distal femoral fractures, shorter supracondylar nails utilizing the same intercondylar starting point can be employed. This approach allows for rigid intramedullary fixation without the need for hip positioning and offers a streamlined surgical corridor, particularly beneficial in polytrauma settings.
Distal Femoral Anatomy and Entry Point
The femoral shaft transitions in its cross-sectional morphology. It is predominantly tubular over the extent of the isthmus, gradually flaring infraisthmally into the distal femur, which assumes a more trapezoidal configuration in cross-section. This anatomical transition is critical for appropriate nail design and trajectory.
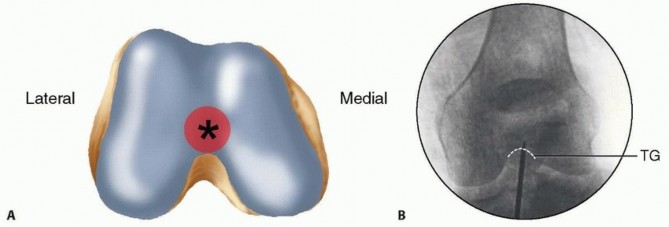
The ideal entry point for the retrograde femoral nail is a paramount consideration for successful implantation and avoidance of iatrogenic complications. It is consistently located at the most distal aspect of the patellofemoral groove, situated just anterior to the posterior cruciate ligament (PCL) insertion site. This area represents a relatively flat articular surface that experiences minimal to no contact with the patella until approximately 120 degrees of knee flexion, thereby minimizing the risk of iatrogenic patellofemoral chondrosis or impingement in physiological ranges of motion.
Radiographically, precise localization of this entry point is crucial. On the anteroposterior (AP) view of the knee, the entry point is typically found in the midline or slightly medial to the midline, positioned symmetrically between the femoral condyles. On the lateral radiographic view, the entry point is situated just anterior to the line of Blumensaat as it intersects with the trochlear groove. These radiographic landmarks serve as critical guides for initial guidewire placement, ensuring an optimal sagittal and coronal plane trajectory for the intramedullary implant. Care must be taken to avoid posterior penetration into the PCL insertion, which can lead to ligamentous injury, or excessively anterior placement, which can cause patellofemoral tracking issues.
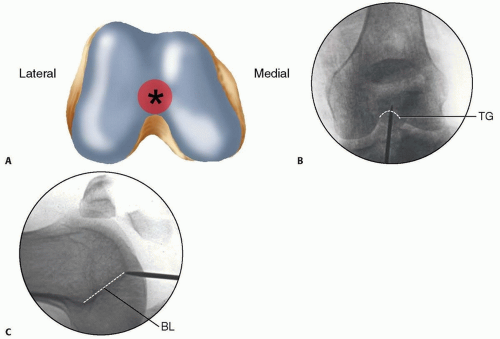
FIG 1 • A. Distal femur viewed end on, with ideal starting point for retrograde femoral nailing identified (asterisk) just anterior to the posterior cruciate ligament insertion. B,C. AP and lateral radiographs of the knee, with the initial starting guidewire positioned at the ideal starting point for retrograde femoral nailing. The radiographic landmark for the trochlear groove (TG) is indicated on the AP radiograph and for the line of Blumensaat (BL) on the lateral radiograph.
Biomechanical Considerations
Retrograde femoral nailing offers significant biomechanical advantages, particularly in load sharing and stability. As an intramedullary device, the nail functions as an internal splint, distributing stress along the length of the bone and providing relative stability conducive to secondary bone healing. The central location of the nail minimizes bending moments compared to extramedullary plating, leading to lower stress on the implant.
Compared to antegrade nailing, RIMN typically utilizes nails with a smaller radius of curvature, designed to accommodate the distal femoral anatomy. The distal locking screws provide multiplanar stability in the metaphysis or epiphysis, resisting shear and rotation. Proximal locking screws secure the nail in the diaphyseal or metaphyseal segment, preventing shortening and rotation. For distal femoral fractures, the shorter nail constructs provide excellent stability for metaphyseal and some intra-articular patterns, preserving the biological environment more effectively than extensive plate osteosynthesis. The critical challenge in RIMN biomechanics lies in ensuring adequate purchase in both the distal and proximal segments, particularly in osteoporotic bone or comminuted fractures, to prevent construct failure or loss of reduction. The precise entry point and correct nail trajectory are essential to maximize load transfer and prevent iatrogenic stress risers.
Indications and Contraindications
Retrograde intramedullary nailing has specific advantages that make it the preferred technique in various challenging clinical scenarios. Careful patient selection and thorough preoperative planning are paramount.
Indications for Retrograde Intramedullary Nailing
- Polytrauma Patients Patients with multiple injuries, including significant head, chest, or abdominal trauma, where supine positioning on a standard operating table is often preferred for airway management and access to other injuries.
- Concomitant Ipsilateral Injuries
- Ipsilateral Pelvic or Acetabular Fractures Retrograde nailing avoids the need for hip flexion and abduction that might compromise reduction or fixation of pelvic/acetabular injuries.
- Ipsilateral Tibial Plateau or Shaft Fractures (Floating Knee Injuries) Allows for simultaneous or sequential management of both femur and tibia fractures without repositioning, especially if antegrade tibial nailing is performed.
- Ipsilateral Distal Radius or Humeral Fractures Facilitates surgical access to upper extremities without changing patient position.
- Distal Femoral Fractures
- Certain supracondylar and intercondylar femoral fractures (AO/OTA 33-A, 33-C1, and some 33-C2 patterns) are well-suited for retrograde nailing, especially when articular comminution is limited or can be anatomically reduced.
- Femoral Shaft Fractures
- Mid-diaphyseal and distal diaphyseal fractures.
- Segmental or comminuted shaft fractures where a long nail provides adequate stability.
- Specific Patient Cohorts
- Morbidly Obese Patients Antegrade nailing can be technically challenging due to thick soft tissues hindering access and imaging of the greater trochanter. Retrograde access from the knee is often less encumbered.
- Patients with Pre-existing Hardware in the Hip Region (e.g., total hip arthroplasty components, hip fusion, proximal femoral plates, ununited trochanteric fractures) that obstruct antegrade entry.
- Pregnancy Reduces radiation exposure to the pelvic region.
- Pathologic Femur Fractures or Impending Fractures Offers stable fixation for prophylactic or therapeutic management, particularly in the distal and mid-shaft.
- Periprosthetic Fractures Around total hip arthroplasties (Vancouver B1, C) when the fracture extends distally and bypassing the stem with antegrade nailing is not feasible.
Contraindications for Retrograde Intramedullary Nailing
- Active Knee Sepsis Absolute contraindication due to the risk of propagating infection along the nail tract.
- Severe Ipsilateral Knee Arthritis Relative contraindication. The intra-articular entry point may exacerbate symptoms or accelerate arthritic progression. Careful risk-benefit analysis is required, and some surgeons consider this an absolute contraindication for higher-grade arthritis.
- Open Fractures with Significant Knee Joint Contamination High risk of joint infection; typically managed by external fixation and staged conversion or alternative definitive fixation.
- Ipsilateral Patellar or Condylar Fractures That significantly compromise the integrity of the intercondylar notch or the patellofemoral articular surface, making a safe and stable entry point unattainable.
- Significant Intra-articular Comminution (AO/OTA 33-C3 patterns) Where anatomical reduction and stable fixation of the articular fragments cannot be achieved prior to or during nail insertion.
- Inadequate Bone Stock In the distal femur, precluding stable locking screw purchase.
- Severe Angular Deformity of the Distal Femur Precluding safe passage of the nail without iatrogenic cortical violation.
Operative Versus Non-Operative Indications
Non-operative management of adult femoral shaft fractures is rarely indicated due to the high rates of malunion, nonunion, and prolonged rehabilitation. However, distinguishing when RIMN is the optimal operative choice versus other operative techniques is crucial.
| Category | Operative Indication (Retrograde Nailing) | Operative Alternative (Other Methods) | Non-Operative Indication |
|---|---|---|---|
| Fracture Type | Distal femoral (supracondylar/intercondylar 33-A, 33-C1/C2) | Highly comminuted articular distal femur (33-C3) | Extremely rare for adult femur fractures; often only for severe medical contraindications for surgery. |
| Mid/Distal femoral shaft (32-A/B/C) | Proximal femoral shaft (31-A/B/C) if antegrade access is clear | Palliative care for terminally ill patients, select stress fractures. | |
| Segmental, comminuted patterns | |||
| Patient Factors | Polytrauma, Ipsilateral pelvis/acetabular fracture, Floating knee, Morbid obesity | Antegrade access feasible (no contraindications), patient preference, specific fracture types. | |
| Pre-existing hip hardware, pregnancy | |||
| Pathologic fractures | |||
| Local Anatomy | Intact knee joint, suitable intercondylar notch for entry point | Severe ipsilateral knee arthritis, compromised intercondylar notch. | |
| Proximal femur anatomical constraints for antegrade entry (e.g., severe deformity) | |||
| Contraindications | No active knee sepsis, no severe intra-articular comminution compromising entry | Active knee sepsis, significant intra-articular contamination, inability to reduce. |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is a cornerstone of successful retrograde femoral nailing, mitigating potential intraoperative challenges and optimizing patient outcomes.
Pre Operative Planning
- Radiographic Assessment:
- Standard Radiographs: AP and lateral views of the entire femur, including the hip and knee joints, are essential. Oblique views may be helpful for complex distal fractures.
- Contralateral Femur: AP and lateral radiographs of the contralateral femur are invaluable for templating nail length, diameter, and assessing the natural femoral bowing, especially if the ipsilateral bone stock is compromised.
- CT Scan: For complex distal femoral fractures (e.g., Hoffa fractures, extensive intra-articular comminution, or metaphyseal impaction), a CT scan with 3D reconstructions provides detailed information regarding fracture morphology, articular involvement, and potential challenges to nail insertion and locking.
- Templating:
- Nail Length and Diameter: Utilize templates to determine the appropriate nail length, ensuring it extends from the distal entry point to the desired level in the proximal femur (e.g., just proximal to the lesser trochanter). Nail diameter should be chosen after assessing the narrowest part of the medullary canal (isthmus) from radiographs. Undersizing can lead to rotational instability, while oversizing risks iatrogenic fracture.
- Nail Curvature: Retrograde nails typically have a sagittal bow designed to match the anterior curvature of the distal femur. Understanding the nail's curvature and its interaction with the femoral anatomy is crucial to prevent cortical impingement, particularly in the midshaft.
- Entry Point Confirmation: Preoperatively visualize the ideal entry point on radiographs and mentally confirm its feasibility based on the patient's anatomy and fracture pattern.
- Patient-Specific Considerations:
- Assess for comorbidities (e.g., obesity, osteoporosis, vascular disease) that might influence surgical technique, implant choice, or postoperative care.
- Discuss potential challenges with the anesthesia team, especially for polytrauma patients requiring extensive monitoring or specific positioning.
Patient Positioning
Optimal patient positioning is critical for unimpeded surgical access, accurate radiographic imaging, and effective fracture reduction.
- Positioning on Radiopaque Table: The patient is typically positioned supine on a radiolucent operating table to allow for unrestricted C-arm fluoroscopy. A general anesthetic or regional block is administered.
- Knee Flexion: The ipsilateral knee is flexed to approximately 90 degrees. This can be achieved by draping the foot off the end of the table, using a leg holder, or placing a padded bolster beneath the distal thigh/proximal calf. This flexion maneuver opens the intercondylar notch, relaxes the quadriceps mechanism, and positions the patella superiorly, facilitating access to the intercondylar entry point.
- Hip Positioning: The hip should be in a neutral adduction/abduction and rotation position. A small bump placed under the ipsilateral gluteal region may help to prevent external rotation of the limb, ensuring neutral alignment of the femur.
- C-arm Positioning: The C-arm must be able to obtain true AP and lateral views of the entire femur (hip, shaft, and knee). This often requires the C-arm to be positioned from the contralateral side of the patient, allowing it to swivel for both proximal and distal imaging. Confirming unrestricted C-arm access throughout the entire femoral length is a critical step before sterile draping.
- Traction: While manual traction is often sufficient for reduction, some surgeons prefer a fracture table with skeletal or skin traction, particularly for highly unstable or comminuted fractures, to maintain length and rotation. However, fracture tables can sometimes impede C-arm access to the hip.
Detailed Surgical Approach and Technique
The surgical technique for retrograde femoral nailing requires meticulous attention to detail to ensure precise entry, accurate reduction, and stable fixation while minimizing iatrogenic damage.
Anesthesia and Preparation
Following induction of general or regional anesthesia, the affected limb is prepped and draped in a sterile fashion from the mid-thigh to the foot. A tourniquet is not typically used but can be an option if significant bleeding is anticipated during distal articular work.
Incision and Arthrotomy
- Skin Incision: A longitudinal skin incision, approximately 3-5 cm in length, is made over the distal patellar tendon, centered in the midline. Some surgeons prefer a medial or lateral parapatellar incision, reflecting the patella to improve exposure and potentially reduce patellar tendon irritation.
- Mini-Arthrotomy: A small longitudinal incision is made through the patellar tendon or via a parapatellar approach. This creates a window into the knee joint. Care must be taken to avoid excessive incision of the patellar tendon, which could compromise extensor mechanism function.
- Visualization of Entry Point: With the knee flexed to 90 degrees, the patella is retracted superiorly. The intercondylar notch is exposed. The ideal entry point, as previously described, is located just anterior to the PCL insertion, at the most distal aspect of the patellofemoral groove. Palpation can confirm this soft spot.
Entry Portal Creation
- Guidewire Insertion: Under fluoroscopic guidance (both AP and lateral views), a small awl or a specific retrograde guidewire (often cannulated) is carefully advanced through the identified entry point.
- AP View: Ensure the guidewire is perfectly centered between the condyles or slightly medial.
- Lateral View: The guidewire should be positioned just anterior to Blumensaat's line where it meets the trochlear groove, targeting the central axis of the distal femur. Avoid posterior penetration which risks PCL injury or anterior penetration which can lead to patellofemoral issues.
- Confirmation of Trajectory: Once the initial guidewire is firmly seated in the distal femoral canal, its trajectory is assessed on both AP and lateral fluoroscopic views along the entire length of the femur. The wire should ideally be centered in the medullary canal at the level of the fracture and proximally. If the trajectory is off, the guidewire should be reinserted.
- Awl/Drill Placement: A cannulated awl or drill, typically 10-12 mm in diameter, is then advanced over the guidewire to create a sufficiently wide entry portal through the distal femoral cortex. This minimizes the risk of iatrogenic fracture during subsequent reaming and nail insertion.
Reduction Techniques
Achieving and maintaining fracture reduction is critical before and during nail insertion.
- Indirect Reduction:
- Traction: Longitudinal traction, either manual or mechanical (via a fracture table), is applied to restore length.
- Manipulation: External manipulation of the limb (flexion, extension, rotation) and fracture fragments can help align the fracture.
- External Aids: A temporary external fixator can be applied as a reduction tool, particularly for highly comminuted or unstable fractures, to maintain length and alignment while the nail is inserted.
- Blocking Screws (Poller Screws): For fractures with significant coronal or sagittal deformity, strategically placed blocking screws in the proximal or distal fragment (away from the nail path) can guide the nail into the correct anatomical axis.
- Direct Reduction: In situations where indirect methods are insufficient, a limited open approach may be necessary. Joysticks, pointed reduction clamps, or small plates can be used to anatomically reduce and temporarily stabilize fragments.
- Rotational Control: Rotational alignment is crucial. This can be assessed clinically (patellar orientation, foot position) and radiographically (cortical step-off, comparison with contralateral side, or lesser trochanter visibility).
Reaming
- Guidewire Exchange (if necessary): If a solid guidewire was used initially, it may be exchanged for a flexible reaming guidewire.
- Sequential Reaming: Reaming is performed sequentially, increasing the reamer diameter by 0.5 mm increments. The reamer should be advanced slowly and deliberately over the guidewire, particularly past the fracture site, to avoid iatrogenic cortical perforation or distraction.
- Reaming Diameter: The canal is typically over-reamed by 1-2 mm compared to the planned nail diameter. Adequate reaming ensures sufficient space for nail insertion, minimizes stress on the bone, and allows for better rotational stability. For certain nail designs or fracture types, undreamed nails may be used.
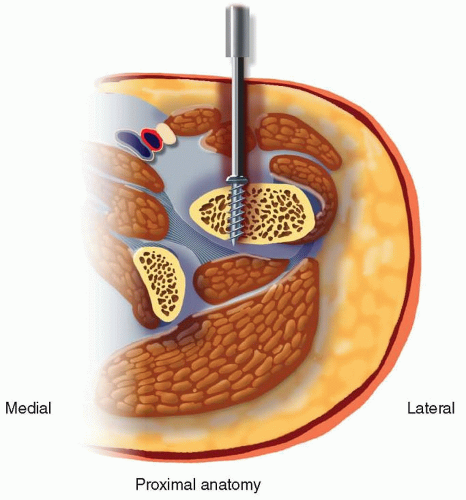
FIG 2 • Sequential reaming of the femoral canal is performed over a guidewire, gradually increasing the diameter to match the chosen nail size plus an appropriate over-ream. Fluoroscopic guidance is used to monitor reamer progression and ensure proper intramedullary trajectory.
Nail Insertion
- Nail Selection: The chosen retrograde nail, matched to the templated length and diameter, is mounted onto the insertion handle.
- Insertion: The nail is carefully advanced over the guidewire, maintaining fracture reduction. Gentle rotational maneuvers may be necessary to navigate the canal curvature. Avoid forceful impaction, which can lead to iatrogenic fracture or distraction.
- Monitoring Reduction: Continuously monitor fracture reduction with fluoroscopy during nail insertion. If reduction is lost, withdraw the nail slightly, re-reduce the fracture, and then continue insertion.
- Final Position: The nail is advanced until its distal end is flush with or slightly recessed from the articular cartilage of the intercondylar notch, and its proximal end reaches the desired level (e.g., just proximal to the lesser trochanter).
FIG 3 • The retrograde intramedullary nail is carefully inserted over the guidewire into the reamed femoral canal. Continuous fluoroscopic monitoring confirms maintenance of fracture reduction, proper nail trajectory, and avoidance of cortical impingement throughout the insertion process.
Proximal and Distal Locking
- Distal Locking (Proximal Femur):
- The nail design dictates the number and orientation of distal locking screws (e.g., two transverse, two oblique).
- Using a targeting jig attached to the insertion handle, incisions are made, and drills are advanced bicortically through the appropriate screw holes.
- Screw length is measured, and screws are inserted. Ensure proper screw engagement in both cortices.
- Proximal Locking (Distal Femur):
- This is often performed freehand due to the acute angle and potential jig misalignment.
- Fluoroscopy is used to align the screw holes (perfect circle technique).
- An incision is made, and a trocar is advanced to the lateral femoral cortex. A drill is advanced bicortically through the nail hole.
- Screw length is measured, and screws are inserted. Two bicortical locking screws are generally preferred for robust distal fixation.
- Confirm final screw positions and nail position on AP and lateral fluoroscopic views.
Wound Closure
After irrigation of the knee joint and deep tissues, the arthrotomy is closed with absorbable sutures. The patellar tendon, fascia, subcutaneous tissue, and skin are closed in layers. A sterile dressing is applied.
Complications and Management
Despite its effectiveness, retrograde femoral nailing is not without potential complications. Awareness of these risks and preparedness for their management are essential.
Common Complications
| Complication | Incidence (Approximate) | Management Strategies |
|---|---|---|
| Intraoperative | ||
| Iatrogenic Articular Cartilage Damage | 5-15% | Meticulous entry point selection, use of appropriate awl/drill, careful guidewire insertion. If minimal, observe. If significant, consider arthroscopic debridement or microfracture. |
| Posterior Cruciate Ligament (PCL) Injury | <1% | Meticulous anterior entry, avoid posterior penetration with guidewire/awl. If partial, non-operative management with bracing. If complete, reconstructive surgery may be required, typically staged. |
| Malreduction (Rotational, Angulation, Length) | 5-10% (can vary with fracture type) | Intraoperative assessment with true AP/lateral views, comparison to contralateral limb. Revision of reduction before definitive locking. Use of reduction aids (traction, blocking screws, clamps). If recognized postoperatively, revision nailing, osteotomy, or exchange nailing may be indicated depending on severity and impact on function. |
| Iatrogenic Fracture (Proximal/Distal Femur) | <5% | Typically due to forceful reaming/nail insertion, or malreduction leading to cortical impingement. Manage by intraoperative extension of fixation (e.g., longer nail, plate) or revision nailing. |
| Neurovascular Injury | <1% | Careful dissection during access. Injury to geniculate vessels is rare but possible. If suspected, immediate vascular surgery consultation. |
| Early Postoperative | ||
| Infection (Superficial/Deep) | <5% (deep <1-2%) | Prophylactic antibiotics, meticulous sterile technique. Superficial: wound care, oral antibiotics. Deep: surgical debridement, irrigation, hardware retention with suppressive antibiotics or hardware removal/exchange nailing with antibiotic spacer, followed by definitive fixation. |
| Compartment Syndrome | Rare (<1%) | Clinical suspicion and measurement of compartment pressures. Emergent fasciotomy. |
| Knee Pain/Stiffness | 10-30% | Early rehabilitation, physical therapy. For persistent severe pain, hardware removal (especially distal screws) after union, or diagnostic arthroscopy for intra-articular causes. |
| Late Postoperative | ||
| Nonunion | 5-15% | Depends on fracture type, comminution, and bone quality. Managed with revision nailing (exchange nailing often preferred), dynamization, bone grafting (autograft/allograft), or plate augmentation. |
| Malunion | 5-10% | Functional impact assessed. Mild, asymptomatic malunions may be observed. Symptomatic malunions (e.g., limb length discrepancy, rotational deformity >15-20 degrees, significant angulation) may require corrective osteotomy. |
| Hardware Failure (Breakage/Migration) | <5% | Typically associated with nonunion or excessive loading. Managed in conjunction with nonunion treatment. May require hardware removal and revision fixation. |
| Anterior Knee Pain | 15-40% | Multifactorial (hardware prominence, patellofemoral irritation). Often resolves. If persistent and severe, hardware removal (especially prominent distal locking screws or nail tip) after fracture union. Conservative management with activity modification, NSAIDs, physical therapy. |
| Heterotopic Ossification | 5-20% | Prophylactic measures for high-risk patients (e.g., severe head injury, burn patients). For established HO causing functional limitation, surgical excision after maturation, often combined with radiation therapy or NSAIDs. |
| Patellofemoral Arthritis | Long-term risk, incidence unclear | Related to iatrogenic cartilage damage or altered patellofemoral mechanics. Non-operative management initially. Severe, debilitating cases may eventually require arthroplasty. |
Management Principles
- Prevention: The best management is prevention through meticulous preoperative planning, precise surgical technique, and appropriate patient selection.
- Early Recognition: Vigilant postoperative monitoring for signs of infection, neurovascular compromise, or evolving complications.
- Tailored Approach: Management strategies must be individualized based on the specific complication, its severity, the patient's overall health, and functional demands.
- Multidisciplinary Care: Involve specialists such as infectious disease, vascular surgery, or pain management when appropriate.
Post Operative Rehabilitation Protocols
A structured and progressive postoperative rehabilitation protocol is crucial for optimizing functional outcomes and facilitating return to activity following retrograde femoral nailing. The protocol must be individualized based on fracture stability, implant rigidity, bone quality, and patient comorbidities.
Immediate Postoperative Period (Days 0-14)
- Pain Management: Multimodal analgesia (opioids, NSAIDs, acetaminophen, nerve blocks) to control pain and facilitate early mobilization.
- DVT Prophylaxis: Standard DVT prophylaxis protocols, including pharmacological agents (e.g., LMWH) and mechanical methods (e.g., pneumatic compression devices).
- Weight Bearing:
- Stable Fractures (simple transverse/oblique, adequate locking): Immediate partial weight-bearing (PWB) with crutches or a walker (25-50% body weight) as tolerated.
- Unstable/Comminuted Fractures, Osteoporosis: Touch-down weight-bearing (TDWB) or non-weight-bearing (NWB) for the initial 4-6 weeks, progressing based on radiographic healing.
- Range of Motion (ROM):
- Knee: Active and passive knee ROM exercises initiated immediately, aiming for 0-90 degrees of flexion within the first week to prevent stiffness and reduce anterior knee pain. Continuous passive motion (CPM) machines may be used in some centers.
- Hip/Ankle: Active ROM exercises for the hip and ankle to maintain mobility and circulation.
- Muscle Activation: Isometric quadriceps and gluteal muscle strengthening exercises.
Early Rehabilitation Phase (Weeks 2-6)
- Progression of Weight Bearing: Gradually increase weight bearing as tolerated, guided by pain and radiographic signs of healing (e.g., callus formation). Advance from PWB to full weight-bearing (FWB).
- Increased ROM: Continue working on knee flexion and extension, aiming for at least 0-120 degrees flexion by 6 weeks.
- Strengthening: Initiate light resistance exercises for quadriceps, hamstrings, and gluteal muscles. Focus on controlled movements to protect the healing fracture.
- Gait Training: Progression from walker to crutches, then potentially to a single crutch or cane, as gait mechanics improve and pain decreases.
Intermediate Rehabilitation Phase (Weeks 6-12)
- Full Weight Bearing: Most patients should be FWB by this stage, assuming adequate radiographic healing.
- Advanced Strengthening: Progress to higher resistance exercises, including closed-chain kinetic activities (e.g., squats, lunges) as appropriate. Incorporate balance and proprioceptive training.
- Functional Activities: Work on activities of daily living (ADLs) that require sustained weight bearing and dynamic balance.
- Aerobic Conditioning: Stationary cycling, swimming, or elliptical training to improve cardiovascular fitness without excessive impact.
Advanced Rehabilitation and Return to Activity (Weeks 12+)
- Strength and Endurance: Continue progressive strengthening, focusing on restoring limb symmetry and power.
- Agility and Sport-Specific Training: For patients aiming to return to higher-impact activities or sports, initiate sport-specific drills, agility training, and plyometrics under the guidance of a physical therapist.
- Impact Activities: Gradual reintroduction of impact activities (e.g., running, jumping) only after documented radiographic union and full strength recovery, typically around 4-6 months post-surgery.
- Hardware Removal: While not routinely performed, hardware removal may be considered after 12-18 months if patients experience persistent hardware-related pain (e.g., anterior knee pain from distal screws, prominence of the nail tip). Decision for removal is made on a case-by-case basis.
Throughout the rehabilitation process, regular clinical and radiographic assessments are essential to monitor fracture healing, identify complications, and adjust the protocol as needed. Patient education regarding expected recovery milestones and adherence to the prescribed exercises is paramount for achieving optimal functional outcomes.
Summary of Key Literature and Guidelines
The literature on retrograde intramedullary nailing has steadily evolved, establishing its role as a versatile and effective treatment modality for a broad spectrum of femoral fractures.
Early studies primarily focused on its application in polytrauma patients, demonstrating significant advantages in terms of reduced operative time, decreased blood loss, and easier management of concomitant injuries, particularly ipsilateral pelvic or acetabular fractures and floating knee injuries. A meta-analysis by Ricci et al. (2009) comparing antegrade and retrograde nailing for femoral shaft fractures found no significant differences in union rates or complication profiles, underscoring the comparable efficacy of both techniques in appropriate indications.
For distal femoral fractures, a systematic review by Frank et al. (2014) highlighted excellent union rates with retrograde nailing, ranging from 90-100%, albeit with varying rates of anterior knee pain (15-40%). This complication, often related to prominent hardware or articular irritation, frequently resolves with conservative management or subsequent hardware removal. The surgical technique, particularly precise entry point determination, has been refined through various anatomical and biomechanical studies, emphasizing the importance of staying anterior to the PCL insertion and centered within the trochlear groove.
In morbidly obese patients, several studies have supported retrograde nailing due to improved surgical access, reduced C-arm challenges, and better supine positioning for respiratory management, as evidenced by a study by Bong et al. (2003). For periprosthetic femur fractures around total hip arthroplasties (THA), especially Vancouver B1 and C types, retrograde nailing can offer a viable option when antegrade nail insertion is precluded by existing implants, providing stable fixation and allowing for early mobilization.
Current guidelines from orthopedic trauma associations, such as the Orthopaedic Trauma Association (OTA), recognize retrograde intramedullary nailing as a primary treatment option for specific patterns of femoral shaft and distal femoral fractures, especially in the context of polytrauma, ipsilateral lower extremity injuries, and patient-specific factors like morbid obesity or hip hardware. The choice between antegrade and retrograde approaches often hinges on surgeon preference, available resources, specific fracture characteristics, and the patient's overall clinical status.
Future directions in retrograde nailing research include continued advancements in nail design, such as improved locking mechanisms and biologically friendly coatings, further exploration of patient-specific instrumentation, and long-term studies on articular cartilage effects, particularly in younger, active patients. The integration of advanced imaging modalities like navigation systems could further enhance precision, especially in complex intra-articular fractures. As the understanding of femoral biomechanics and fracture healing evolves, so too will the optimization of retrograde nailing techniques, ensuring continued improvement in patient outcomes.
You Might Also Like