Felon (Pulp Space Infection): Advanced Surgical Drainage & Management
Key Takeaway
Pulp space infections (felons) are critical fingertip infections. Prompt surgical drainage is essential to decompress confined compartments, relieve acute pressure, and restore vascular perfusion. This prevents severe complications like tissue necrosis, osteomyelitis of the distal phalanx, and septic arthritis, thereby preserving crucial digital function.
Pulp Space Infection: Master Essential Drainage Steps
Introduction & Epidemiology
Pulp space infections, commonly known as felons, represent one of the most prevalent and critical infections encountered in the hand, frequently necessitating surgical intervention. These infections are confined within the distal phalanx pulp, a unique fibro-fatty compartment susceptible to rapid pressure accumulation. The typical inciting event is a trivial penetrating injury, allowing inoculation of microorganisms into this confined space.
Epidemiologically, felons show a high incidence, particularly among individuals engaged in manual labor or those with compromised immunity (e.g., diabetes mellitus, HIV). While often considered a minor ailment, the distinct anatomy of the digital pulp predisposes to severe complications if not managed promptly and appropriately. The tightly packed fibrous septa that anchor the skin to the periosteum of the distal phalanx act as barriers, preventing proximal spread of infection but simultaneously limiting outward expansion of pus. This results in an acute rise in intra-compartmental pressure, which can rapidly compromise the vascular supply to the pulp tissue and the underlying distal phalanx, leading to tissue necrosis, osteomyelitis, or even septic arthritis of the distal interphalangeal (DIP) joint.
The predominant causative organisms are Gram-positive cocci, primarily Staphylococcus aureus , including methicillin-resistant S. aureus (MRSA), and Streptococcus pyogenes . Less commonly, Gram-negative organisms may be involved, especially in immunocompromised patients, those with specific exposures (e.g., freshwater injuries), or polymicrobial infections. Early diagnosis and judicious management are paramount to prevent irreversible tissue damage and preserve digital function. Differential diagnoses include herpetic whitlow (characterized by vesicles and typically managed non-surgically), cellulitis (lacks a localized abscess), paronychia (infection of the nail fold), and occasionally foreign body reactions.
Surgical Anatomy & Biomechanics
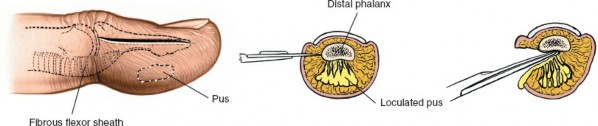
A thorough understanding of the unique surgical anatomy of the fingertip pulp is fundamental to effective and safe surgical drainage of a felon. The distal finger pulp consists of a dense network of fibrous septa that extend radially from the periosteum of the distal phalanx to the dermis of the volar skin. These septa divide the pulp into numerous small, vertically oriented compartments, each containing fat, sweat glands, nerve endings, and a rich vascular supply.
The vascularity of the fingertip is robust, supplied by the terminal branches of the radial and ulnar digital arteries. These vessels form an extensive capillary network within the pulp. The close proximity of these delicate vessels to the unyielding fibrous septa is critical: even a small collection of pus within one of these compartments can lead to a significant increase in local tissue pressure. This pressure elevation can quickly exceed capillary perfusion pressure, resulting in localized ischemia, infarction, and necrosis of the pulp tissue and potentially the underlying bone.
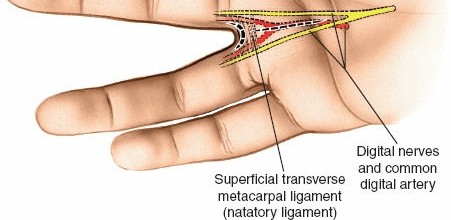
Sensory innervation is provided by the terminal branches of the digital nerves, which are highly concentrated in the fingertips, contributing to their exquisite tactile sensitivity. Incisions must be planned meticulously to avoid damage to these neurovascular structures, particularly the main digital neurovascular bundles that run along the lateral aspects of the digits, slightly volar to the mid-lateral line.
The distal phalanx lies directly beneath the pulp, making it vulnerable to osteomyelitis, particularly if the infection is deep-seated or inadequately drained. The phalanx contributes to the stability of the fingertip and supports the nail complex. The nail matrix, responsible for nail growth, is located at the base of the nail and can be inadvertently damaged by aggressive surgical techniques, leading to permanent nail deformities.
Biomechanically, the rapid accumulation of exudate within these confined fibrous compartments creates a true 'compartment syndrome' of the fingertip. This pressure-mediated vascular compromise is the primary mechanism by which a felon can progress rapidly from a localized infection to tissue necrosis and deeper structural involvement. The goal of surgical drainage is to decompress these compartments, relieve pressure, and allow for unimpeded drainage of purulent material, thereby restoring perfusion and preventing further tissue destruction.
Indications & Contraindications
The decision to proceed with surgical drainage of a felon is based on a comprehensive clinical assessment, acknowledging the rapid destructive potential of these infections.
Indications for Operative Management:
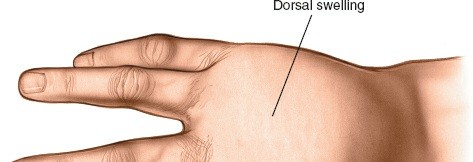
- Clinical Signs of Abscess Formation: The presence of fluctuance on palpation, severe throbbing pain, localized erythema, and marked swelling suggestive of a walled-off pus collection. Pain is often disproportionate to the visible swelling due to the compartmental nature of the infection.
- Failure of Conservative Management: If initial empiric antibiotic therapy and elevation fail to improve symptoms or halt progression within 24-48 hours, especially in cases where an abscess is suspected but not yet overtly fluctuant.
- Signs of Deep-Seated Infection or Complications: Suspicion or confirmed diagnosis of underlying osteomyelitis of the distal phalanx (e.g., based on imaging or clinical findings like exposed bone in a penetrating injury), or septic arthritis of the DIP joint.
- Systemic Signs of Infection: Fever, chills, lymphangitis, or lymphadenopathy accompanying a localized pulp space infection, indicating systemic involvement and requiring aggressive source control.
- Immunocompromised Patients: Patients with diabetes, HIV, or those on immunosuppressive medications often have a blunted inflammatory response and rapidly progressing infections, necessitating a lower threshold for surgical intervention.
Contraindications for Operative Management (Relative):
- Early Cellulitis Without Abscess Formation: If the infection is purely cellulitic, without any evidence of pus collection or fluctuance, a trial of oral or intravenous antibiotics, elevation, and warm soaks may be appropriate. Careful monitoring is essential.
- Herpetic Whitlow: This viral infection of the fingertip is characterized by vesicular lesions and should not be incised, as surgical drainage is ineffective and can exacerbate the condition or lead to secondary bacterial infection. Diagnosis is typically clinical, but Tzanck smear or viral culture can confirm.
- Poorly Controlled Coagulopathy: While not an absolute contraindication, severe bleeding diatheses should ideally be corrected prior to surgery to minimize intraoperative and postoperative complications.
- Patient Refusal: After thorough discussion of risks and benefits, if a patient declines surgical intervention, alternative management strategies (e.g., observation, increased antibiotics) may be considered, but with careful documentation and counseling regarding potential adverse outcomes.
Summary of Operative vs. Non-Operative Indications
| Feature / Condition | Operative Management | Non-Operative Management |
|---|---|---|
| Clinical Presentation | Fluctuance, severe throbbing pain, spreading erythema, systemic signs (fever, chills) | Early cellulitis without fluctuance or systemic signs |
| Infection Depth | Deep-seated infection, suspected or confirmed osteomyelitis | Superficial, non-abscess forming infection |
| Response to Treatment | Worsening despite 24-48 hours of antibiotic therapy | Improvement with initial empiric antibiotic therapy and local care |
| Specific Conditions | Immunocompromised patients (lower threshold) | Herpetic whitlow (viral etiology) |
| Diagnostic Findings | Ultrasound confirming abscess, X-ray showing osteomyelitis | Absence of abscess on ultrasound, normal X-rays |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential to ensure a successful outcome and minimize complications during felon drainage.
Patient Evaluation
- History: Obtain a detailed history focusing on the mechanism and timing of injury, previous infections, relevant comorbidities (especially diabetes, peripheral vascular disease, immunosuppression), allergies, and current medications. Ascertain tetanus immunization status.
- Physical Examination: A thorough hand examination is crucial. Assess the extent of swelling, erythema, and tenderness. Palpate for fluctuance. Evaluate neurovascular status of the digit (capillary refill, two-point discrimination, sensation). Assess range of motion of the DIP and PIP joints to rule out septic arthritis. Examine for lymphangitis or regional lymphadenopathy.
Imaging Studies
-
Plain Radiographs:
Anteroposterior, lateral, and oblique views of the affected digit should be obtained. These are vital to:
- Rule out a retained foreign body as the inciting cause.
- Assess for early signs of osteomyelitis of the distal phalanx (e.g., periosteal reaction, cortical erosion, or lytic lesions).
- Evaluate for septic arthritis of the DIP joint (e.g., joint space widening, destruction, or effusion).
-
Ultrasound:
High-frequency ultrasound is an excellent, non-invasive tool to:
- Precisely localize the pus collection within the pulp space.
- Differentiate between cellulitis and an organized abscess, aiding in surgical planning.
- Guide aspiration for Gram stain and culture if diagnostic uncertainty exists.
- Magnetic Resonance Imaging (MRI): Reserved for complex cases with high suspicion of deep-seated infection, extensive osteomyelitis, or unclear etiology, where plain films and ultrasound are inconclusive. MRI can delineate the extent of soft tissue involvement and bone marrow edema more accurately.
Laboratory Studies
- Complete Blood Count (CBC) with Differential: To assess for leukocytosis and shifts suggestive of bacterial infection.
- Inflammatory Markers: Erythrocyte Sedimentation Rate (ESR) and C-Reactive Protein (CRP) can indicate systemic inflammation and monitor response to treatment, particularly in osteomyelitis.
- Blood Cultures: Indicated for patients presenting with systemic signs of infection (e.g., fever, chills).
Antibiotic Prophylaxis and Therapy
- Empiric Antibiotics: Initiate broad-spectrum antibiotics empirically after obtaining cultures (from pus, if available) and prior to incision. The choice should cover common skin flora, primarily Staphylococcus aureus (including MRSA, if prevalent in the region) and Streptococcus pyogenes . Common initial choices include clindamycin, vancomycin (for suspected MRSA), or a first-generation cephalosporin.
- Culture-Directed Therapy: Adjust antibiotics based on Gram stain results (if performed on pus) and definitive culture and sensitivity reports obtained during surgery.
Anesthesia
- Digital Block: The most common method. Infiltrate 1-2% lidocaine (without epinephrine) at the base of the digit, targeting the dorsal and volar neurovascular bundles. This provides excellent regional anesthesia for the procedure. Bupivacaine may be added for prolonged analgesia. Crucially, epinephrine must never be used in a digital block due to the risk of vasoconstriction and digital ischemia.
- Bier Block (Intravenous Regional Anesthesia): May be used for more extensive infections or if multiple digits are involved.
- General Anesthesia: Reserved for pediatric patients, highly anxious adults, or very extensive infections requiring prolonged operating time.
Tourniquet
A bloodless field is paramount for precise dissection and identification of critical structures. A digital tourniquet is applied at the base of the digit after exsanguination (e.g., with an Esmarch bandage or by manually wrapping from distal to proximal). A sterile glove finger or a small Penrose drain can serve as an effective digital tourniquet.
Patient Positioning
The patient is positioned supine on the operating table, with the arm placed comfortably on an arm board. The hand should be pronated or supinated as required for optimal access to the affected digit. Adequate lighting and magnification (e.g., surgical loupes) are highly recommended.
Detailed Surgical Approach / Technique
The primary objective of felon drainage is to adequately decompress the infected pulp space, evacuate purulent material, prevent further tissue destruction, and avoid iatrogenic injury to vital structures. A bloodless field with a digital tourniquet is essential.
Aseptic Preparation
The hand and affected digit are thoroughly prepped with an antiseptic solution (e.g., povidone-iodine or chlorhexidine) and sterilely draped.
Principles of Incision
Key principles for incision choice and execution include:
* Minimizing damage to neurovascular bundles and sensory nerves.
* Avoiding painful, adherent scars, especially on the critical tactile surface of the volar pulp.
* Ensuring complete drainage of all loculations.
* Preserving the integrity of the nail matrix and distal phalanx.
* Avoiding extension into the DIP joint or proximal to the distal interphalangeal crease.
Types of Incisions and Techniques
The choice of incision depends on the location and depth of the pus collection.
-
Lateral Longitudinal Incision (Unilateral Drainage):
This is the most widely accepted and preferred incision for deep-seated felons due to its efficacy and lower complication rate compared to older techniques.- Positioning: The digit is placed in a neutral position with gentle tension.
- Incision Placement: A straight incision is made on the lateral aspect of the terminal phalanx of the finger. It should be positioned slightly dorsal to the mid-lateral line, avoiding the main neurovascular bundle which runs more volarly. The incision extends from the level of the distal interphalangeal joint (but not crossing the joint crease) distally towards the tip of the finger, close to the nail edge. It should not extend proximally to the DIP joint to avoid damaging the digital nerve and potentially contaminating the joint.
-
 -
Dissection:
- Incise the skin and subcutaneous tissue.
- Carefully dissect through the fibrous septa into the pulp space. This can be done with a fine scalpel or preferably with a fine hemostat or blunt probe, directing it towards the center of the pulp. The goal is to break down the septa and enter all loculations.
-
 - Once pus is encountered, it should be sampled for Gram stain and aerobic/anaererobic culture and sensitivity testing.
- Exploration and Debridement: Using a fine blunt probe or hemostat, carefully explore the entire pulp space. Break down any remaining fibrous septa that are compartmentalizing the infection, ensuring all loculations are opened and pus is freely draining. Palpate the distal phalanx to assess for bone involvement (osteomyelitis), and if present, gently debride any necrotic bone fragments.
- Irrigation: Copiously irrigate the cavity with sterile saline to remove debris and residual pus.
- Drainage: The wound is typically left open to drain. A small, thin strip of non-adherent gauze (e.g., petroleum gauze) or a small Penrose drain may be loosely placed within the cavity to prevent premature skin closure and ensure continued drainage. Avoid tight packing , as this can recreate pressure and impair healing.
-
 -
-
Lateral Oblique Incision (for Superficial, Pointing Abscesses):
If the abscess is superficial and clearly pointing on the volar aspect of the distal pulp, a small, oblique incision can be made on the lateral side of the volar surface. This allows direct entry into the abscess cavity with minimal collateral damage. This approach is less common for typical felons which are often deep-seated. Midline volar incisions are generally avoided due to the high risk of painful, hypersensitive scars. -
Obsolete Incision Techniques:
-
"Through-and-Through" (H-shaped or Fishmouth) Incisions:
These techniques involved creating multiple incisions, often on both sides of the pulp or a large volar flap. They are
strongly discouraged
due to extremely high rates of complications including:
- Flail fingertip: Destabilization of the distal phalanx due to excessive tissue removal.
- Painful scars and neuromas: Due to extensive nerve damage and scarring on the tactile surface.
- Digital ischemia/necrosis: Compromised vascularity from aggressive dissection.
- Nail deformities.
-
"Through-and-Through" (H-shaped or Fishmouth) Incisions:
These techniques involved creating multiple incisions, often on both sides of the pulp or a large volar flap. They are
strongly discouraged
due to extremely high rates of complications including:
Post-Drainage Management
Once drainage is complete, the digital tourniquet is released, and hemostasis is ensured. A sterile, non-compressive dressing is applied.
Complications & Management
Despite appropriate surgical drainage, felons can lead to significant complications if not meticulously managed. Awareness of these potential issues is crucial for proactive prevention and effective salvage strategies.
| Complication | Incidence | Etiology & Salvage Strategies | Recurrence/Persistent infection | ~10-20% | Inadequate drainage or resistant organism. |
Salvage:
Re-drainage, obtain deep cultures, adjust broad-spectrum or directed antibiotics, consider imaging for missed abscess/osteomyelitis. |
|
Osteomyelitis of Distal Phalanx
| 5-10% (higher with delayed/inadequate drainage) | Direct spread of infection, prolonged pressure on bone. |
Salvage:
Surgical debridement of necrotic bone, prolonged course of culture-directed IV followed by oral antibiotics (typically 4-6 weeks), consider partial amputation in severe cases. |
|
Septic Arthritis of DIP Joint
| <5% (higher with proximal incisions or iatrogenic spread) | Direct extension from felon or iatrogenic contamination during surgery. |
Salvage:
Prompt surgical irrigation and debridement of the joint, arthrotomy, intra-articular and systemic antibiotics, immobilization followed by controlled motion. |
|
Painful Scar / Neuroma
| Varies, ~5-15% (higher with midline volar or extensive incisions) | Incision on weight-bearing or tactile surface, nerve transection/entrapment. |
Salvage:
Scar massage, silicone sheeting, desensitization therapy, corticosteroid injections. For persistent pain, consider scar revision or neuroma excision (rarely required for appropriately placed lateral incisions). |
|
Flail Fingertip / Instability
| Rare with current techniques (historically common with "H" incisions) | Excessive tissue removal, compromise of distal phalanx soft tissue support. |
Salvage:
Primarily preventative. If severe, may require arthrodesis of the DIP joint or reconstructive surgery. |
|
Nail Deformity
| <5% (higher with aggressive dissection near nail matrix) | Injury to the nail matrix (germinal or sterile). |
Salvage:
Primarily preventative. Most resolve spontaneously. For persistent severe deformities, consultation with a hand surgeon for potential nail matrix excision or reconstruction. |
|
Digital Ischemia / Necrosis
| Very rare (related to tight packing or pre-existing vascular compromise) | Tight wound packing, undiagnosed peripheral vascular disease, prolonged tourniquet time. |
Salvage:
Remove all packing, re-evaluate digit vascularity. Consider systemic vasodilators, ensure adequate hydration. Surgical re-exploration if concern for vascular compromise (e.g., hematoma). |
|
Chronic Pain / Stiffness
| Variable, depending on severity of initial infection and patient compliance | Inflammation, prolonged immobilization, scar tissue formation. |
Salvage:
Aggressive hand therapy, pain management strategies (NSAIDs, neuropathic agents), judicious use of splinting to prevent contractures, consider corticosteroid injections for localized inflammation. |
Post-Operative Rehabilitation Protocols
Post-operative management following felon drainage is crucial for infection resolution, wound healing, pain control, and restoration of digital function.
Immediate Post-Operative Period (Day 0-3)
- Dressing: A light, non-compressive, sterile dressing is applied immediately after surgery. The dressing typically consists of a non-adherent contact layer (e.g., petroleum gauze), covered by sterile gauze and a conforming wrap. Ensure the dressing allows for inspection of the nailbed for vascularity.
- Elevation: The hand should be kept elevated above heart level continuously to minimize swelling and pain. This can be achieved with a sling, pillows, or elevation over the chest when supine.
- Pain Management: A multimodal approach is recommended, including NSAIDs (if not contraindicated), acetaminophen, and potentially short-term opioids for severe pain.
- Antibiotics: Continue the culture-directed antibiotic regimen, typically for 7-10 days, or longer if osteomyelitis or other complications are present (e.g., 4-6 weeks for confirmed osteomyelitis). Oral antibiotics are usually sufficient after initial intravenous therapy if signs of systemic infection have resolved.
- Wound Care: The first dressing change is typically performed within 24-48 hours. The wound should be inspected for signs of ongoing drainage, erythema, or re-accumulation of pus. If a drain was placed, it is usually removed within 24-48 hours. The wound is generally left open to heal by secondary intention. Daily dressing changes with saline soaks or antiseptic solution followed by a fresh sterile dressing are usually prescribed.
Early Mobilization and Healing Phase (Day 3 - 2 Weeks)
- Wound Care: Continue daily wound care. Encourage warm saline soaks (e.g., 10-15 minutes, 2-3 times daily) to promote drainage, clean the wound, and aid in softening any eschar.
- Gentle Range of Motion (ROM): As pain subsides and wound healing progresses, encourage gentle active and passive range of motion exercises for the unaffected joints (MCP and PIP joints) and the thumb. For the affected DIP joint, initiate very gentle active ROM as tolerated, ensuring the wound is not compromised. The goal is to prevent stiffness without disrupting healing or increasing inflammation.
- Elevation: Continue elevation, especially when resting, to manage residual swelling.
- Hygiene: Maintain strict hand hygiene to prevent secondary infection.
Intermediate Rehabilitation (Weeks 2-6)
- Progressive ROM: Gradually increase the intensity and frequency of active and passive ROM exercises for the affected digit. Focus on regaining full flexion and extension of the DIP joint. If stiffness is present, passive stretching may be incorporated.
- Scar Management: Once the wound has epithelialized, begin scar massage with a moisturizing lotion to soften the scar tissue and prevent adherence. Silicone sheeting or gel can be introduced to help mature the scar.
- Sensory Re-education: If there was any nerve involvement or sensitivity, initiate sensory re-education exercises (e.g., textures, vibration) to improve tactile discrimination.
- Strengthening (as appropriate): As pain allows and ROM improves, introduce light grip strengthening exercises using soft putty or sponges.
- Activity Modification: Avoid strenuous activities, heavy lifting, or direct trauma to the healing digit. Gradually increase activity levels as tolerated.
Long-Term Follow-up (Beyond 6 Weeks)
- Functional Assessment: Assess overall hand function, grip strength, and dexterity.
- Scar Maturation: Continue scar management until the scar is soft, flat, and non-tender.
- Addressing Residual Issues: If persistent pain, stiffness, or functional limitations exist, further interventions may be considered (e.g., referral to hand therapy for advanced techniques, corticosteroid injections for localized inflammation, or rarely, surgical revision for painful neuromas or problematic scars).
- Education: Educate the patient on protective measures for the digit and recognition of signs of recurrence or new infection.
Throughout the rehabilitation process, close collaboration between the surgeon, patient, and a certified hand therapist is critical to optimize outcomes and ensure the best possible functional recovery.
Summary of Key Literature / Guidelines
The management of pulp space infections has evolved considerably, with a shift towards less invasive yet effective surgical techniques supported by a growing body of literature and clinical guidelines.
Historically, more aggressive "through-and-through" or H-incisions were common, but extensive research and clinical experience have clearly demonstrated their association with unacceptably high complication rates, including debilitating painful scars, digital instability, and nerve damage. Current evidence strongly advocates for unilateral lateral longitudinal incisions as the gold standard for deep-seated felons, and small oblique incisions for very superficial, pointing abscesses. This approach minimizes neurovascular injury, preserves critical tactile sensation, and yields better cosmetic and functional outcomes.
Key principles reinforced by hand surgery societies (e.g., American Society for Surgery of the Hand - ASSH) and orthopedic organizations (e.g., American Academy of Orthopaedic Surgeons - AAOS) include:
- Early and Accurate Diagnosis: Prompt clinical assessment, aided by ultrasound for abscess localization, is critical. Differentiating a felon from cellulitis or herpetic whitlow is paramount, as management strategies differ significantly.
- Timely Surgical Drainage: Once an abscess is identified, surgical drainage should not be unduly delayed. Procrastination increases the risk of complications such as osteomyelitis, septic arthritis, and soft tissue necrosis.
- Appropriate Incision Choice: The lateral longitudinal incision, placed carefully to avoid the neurovascular bundle, is the preferred method for deep felons. Midline volar and "through-and-through" incisions are to be avoided. The incision should be adequate for complete exploration and drainage but no more extensive than necessary.
- Thorough Debridement and Irrigation: Meticulous exploration to break down all fibrous septa and open loculations is essential. Copious irrigation ensures removal of purulent material and debris.
- Pus Culture and Antibiotic Management: Obtaining pus for Gram stain, culture, and sensitivity is mandatory. Empiric broad-spectrum antibiotics, typically targeting S. aureus (including MRSA, if indicated), should be initiated pre-operatively and adjusted based on sensitivity results. The duration of antibiotic therapy is typically 7-10 days, extending to 4-6 weeks for osteomyelitis.
- Leaving Wound Open: The wound should be left open to heal by secondary intention, often with a loose drain or non-adherent dressing, to prevent re-accumulation of pus.
- Post-Operative Rehabilitation: Early, gentle mobilization, elevation, and diligent wound care are crucial for preventing stiffness and promoting optimal functional recovery. Referral to a hand therapist is often beneficial.
Literature reviews and meta-analyses consistently support the superiority of conservative incision techniques over more aggressive historical methods regarding complication rates and functional outcomes. The importance of a multidisciplinary approach, involving orthopedic surgeons, infectious disease specialists, and hand therapists, is emphasized for complex cases, immunocompromised patients, or those with significant comorbidities. Adherence to these guidelines ensures optimal patient care and outcomes in the management of pulp space infections.
Clinical & Radiographic Imaging
You Might Also Like