Congenital Hand Undergrowth & Hypoplastic Thumb: Comprehensive Surgical Management
Key Takeaway
Congenital undergrowth deformities of the hand encompass a spectrum of incomplete developmental anomalies, most notably the hypoplastic thumb. Management depends heavily on the degree of osseous and musculotendinous deficiency, typically categorized by the Blauth classification. Surgical interventions range from intrinsic tendon transfers and ligament reconstructions for mild cases to index finger pollicization for severe deficiencies. Associated length discrepancies may require digital shortening techniques, such as the Barsky or Millesi procedures, to restore biomechanical function and aesthetics.
UNDERGROWTH DEFORMITIES OF THE HAND
Congenital hand anomalies classified as undergrowth deformities represent a complex spectrum of conditions in which embryological development is arrested or incomplete. This developmental failure renders the entire upper extremity, or specific anatomical subunits, dimensionally smaller or structurally deficient. While undergrowth can manifest in isolation, hypoplasia of digital parts frequently presents concomitantly with other profound congenital deformities of the hand and forearm, including radial clubhand (radial longitudinal deficiency), syndactyly, and paradoxical overgrowth anomalies such as macrodactyly.
From a strict taxonomic perspective, the categorization of "undergrowth" is optimally reserved for deformities that present a formed but quantitatively deficient part, devoid of other confounding syndromic anomalies. However, in clinical practice, the orthopedic surgeon must be prepared to address these deficiencies as part of a broader reconstructive strategy.
Epidemiology and Incidence
The true incidence of undergrowth anomalies varies based on the specific anatomical manifestation. In Flatt’s seminal series of congenital hand anomalies, the hypoplastic thumb constituted 3.6% of all presentations, whereas the Yokohama series reported an incidence of 1.3%. Global hypoplasia of the entire hand is exceedingly rare, representing merely 0.8% in Flatt’s series, with total absence of the thumb accounting for 1.4%. Because of the vast phenotypic variability produced by digital hypoplasia, the etiological factors are equally diverse. While many of these deformities arise as sporadic, non-hereditary occurrences, a significant subset is transmitted genetically or is intimately associated with systemic syndromes (e.g., VACTERL association, Holt-Oram syndrome, Fanconi anemia, and TAR syndrome).
Clinical Pearl: Any neonate presenting with a hypoplastic thumb or radial longitudinal deficiency mandates a comprehensive systemic evaluation. Echocardiography, renal ultrasonography, and a complete blood count (to rule out Fanconi anemia) are non-negotiable prerequisites before any surgical intervention is contemplated.
THE HYPOPLASTIC THUMB
The clinical designation “hypoplastic thumb” is a broad umbrella term applied to any thumb exhibiting some degree of deficiency in its foundational anatomical parts—whether osseous, musculotendinous, ligamentous, or ectodermal. The clinical presentation is highly variable; the thumb may be fully functional but simply shorter than its contralateral counterpart, or, in its most severe manifestation, it may be totally absent (aplasia).
Pathoanatomy and Biomechanics
The thumb contributes approximately 40% to 50% of overall hand function, primarily through its unique capacity for opposition, which facilitates pinch and grasp mechanics. In the hypoplastic thumb, biomechanical failure typically stems from a combination of:
1. Thenar Muscle Aplasia: Deficiency of the abductor pollicis brevis (APB) and opponens pollicis impairs palmar abduction and pronation.
2. Ligamentous Laxity: Attenuation or absence of the ulnar collateral ligament (UCL) at the metacarpophalangeal (MCP) joint leads to profound instability during pinch.
3. First Web Space Contracture: Fascial tightness and adductor pollicis contracture tether the thumb to the index finger, obliterating the functional web space.
4. Extrinsic Tendon Anomalies: Aberrant insertions or absence of the flexor pollicis longus (FPL) or extensor pollicis longus (EPL) further degrade kinematic function.
Classification Systems
Historically, hypoplastic thumbs were divided into six descriptive types based on gross appearance: short thumb, adducted thumb, abducted thumb, floating thumb, absent thumb, and clasped thumb. However, the Blauth Classification System has become the universally accepted academic standard, as it directly dictates the surgical algorithm.
- Type I: Minor generalized hypoplasia. All structures are present but proportionally smaller. Function is typically normal, and surgical intervention is rarely indicated.
- Type II: Characterized by an adduction contracture of the first web space, deficient thenar intrinsic musculature, and an unstable MCP joint (specifically the UCL).
- Type III: Further divided into IIIA and IIIB. Both feature the deficiencies of Type II, plus extrinsic tendon abnormalities and skeletal hypoplasia of the first metacarpal.
- Type IIIA: The carpometacarpal (CMC) joint remains stable.
- Type IIIB: The CMC joint is unstable or absent. This is the critical inflection point in the treatment algorithm.
- Type IV: The "pouce flottant" or floating thumb. The thumb is attached to the radial border of the hand by a mere rudimentary skin bridge containing a neurovascular bundle, with no functional osseous or tendinous continuity.
- Type V: Complete absence (aplasia) of the thumb.
Surgical Warning: The distinction between Blauth Type IIIA and IIIB is the most critical decision-making node. Type IIIA thumbs are reconstructed (web space release, UCL reconstruction, opponensplasty). Type IIIB thumbs lack a stable basal joint and are functionally unsalvageable; they require ablation and index finger pollicization.
SURGICAL MANAGEMENT OF ASSOCIATED DIGITAL DISCREPANCIES
As noted, hypoplasia of digital parts frequently coexists with other complex deformities. In syndromic hands, it is not uncommon to encounter a hypoplastic digit adjacent to a hypertrophic digit (macrodactyly). To optimize both the biomechanical cascade of the hand and its aesthetic appearance, the orthopedic surgeon must master techniques for digital length equalization.
When addressing a hand with severe length discrepancies, digital shortening procedures are often employed. Two highly effective, textbook-standard techniques for digital shortening and reduction are the Barsky technique and the Millesi technique.
Digital Shortening for Macrodactyly (Barsky Technique)
The Barsky technique is a robust, reliable method for shortening a disproportionately long digit by resecting the distal half of the middle phalanx and the proximal portion of the distal phalanx, followed by a "pencil-cone" arthrodesis of the distal interphalangeal (DIP) joint.
Indications:
* Severe digital overgrowth interfering with grasp or pinch.
* Length discrepancies where epiphyseodesis is no longer viable or insufficient.
* Cases where DIP joint motion is expendable in favor of improved overall digital proportion and function.
Surgical Steps:
-
Incision and Exposure:
Under tourniquet control and loupe magnification, design an L-shaped midlateral and dorsal incision over the affected digit. This approach allows for the meticulous elevation of full-thickness flaps and the safe removal of excess dorsal soft tissue.
FIGURE 79-61A: L-shaped midlateral and dorsal incisions allow removal of excess dorsal tissue, the distal half of the middle phalanx, and the proximal portion of the distal phalanx (shaded area). -
Osteotomy and Resection:
Identify the DIP joint. Perform a transverse osteotomy to resect the distal half of the middle phalanx. Next, resect the proximal articular portion of the distal phalanx. Ensure that the extensor terminal tendon and the flexor digitorum profundus (FDP) insertions are managed appropriately, depending on the desired final resting posture of the distal phalanx. -
Pencil-Cone Preparation:
Using a fine multi-action rongeur or a high-speed burr, carefully sculpt and sharpen the distal end of the remaining middle phalanx into a tapered point (the "pencil"). Concurrently, prepare the medullary canal of the remaining distal phalanx to act as the receiving "cone."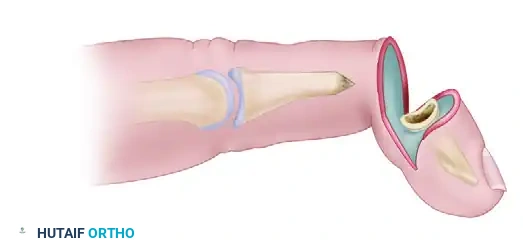
FIGURE 79-61B: Bone ends are prepared for pencil-cone reduction. The middle phalanx is sharpened to fit into the medullary canal of the distal phalanx. -
Reduction and Fixation:
Place the distal phalanx onto the middle phalanx, impacting the pencil tip into the cone. This recesses the finger, achieving the desired shortening. Assess the rotational alignment meticulously by observing the nail plate cascade relative to adjacent digits. Once alignment is perfect, secure the arthrodesis with a longitudinally directed 0.035-inch or 0.045-inch Kirschner wire (K-wire).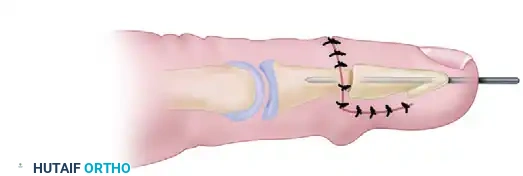
FIGURE 79-61C: The distal phalanx is reduced on the middle phalanx and secured with a Kirschner wire. -
Soft Tissue Management:
Excess volar soft tissue can often be left for a secondary debulking stage to avoid compromising the vascularity of the distal tip. Close the dorsal and midlateral incisions with non-absorbable monofilament sutures.
Thumb Reduction for Macrodactyly (Millesi Technique)
When overgrowth affects the thumb—particularly in the setting of a complex hand anomaly where relative proportions must be restored—the Millesi technique offers an elegant solution. This procedure focuses on shortening the distal phalanx while meticulously preserving the eponychial fold and nail matrix to maintain a cosmetically acceptable thumb tip.
Indications:
* Disproportionate enlargement of the thumb distal phalanx.
* Need for terminal shortening without sacrificing the interphalangeal (IP) joint.
Surgical Steps:
-
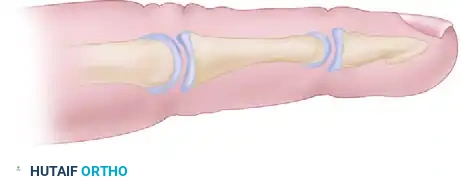
Distal Resection:
Begin by sharply excising the distal half of the nail plate and the underlying distal tuft of the distal phalanx. It is of paramount importance to preserve the proximal eponychial tissue and the germinal matrix to ensure continued, albeit shortened, nail growth.
FIGURE 79-62A: Removal of the distal half of the nail and distal phalanx, meticulously preserving eponychial tissue. -
Reduction Osteotomies:
Make a dorsal longitudinal or lazy-S incision proximal to the eponychial fold to expose the diaphysis of the distal phalanx. Perform precise reduction osteotomies (often a step-cut or transverse wedge) to shorten the bone while maintaining a broad surface area for healing.
FIGURE 79-62B: Reduction osteotomies performed through a dorsal incision. -
Fixation:
Reduce the remaining osseous segments. Ensure that the volar pulp is not excessively tensioned. Pin the osteotomy site with a retrograde K-wire, ensuring the pin does not tether the flexor pollicis longus tendon.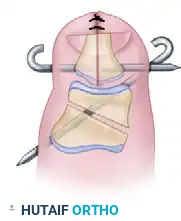
FIGURE 79-62C: The remaining bone is reduced and pinned securely.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The success of reconstructive procedures for undergrowth and associated length discrepancies relies heavily on rigorous postoperative management.
Phase I: Immobilization (Weeks 0-4)
* Immediately postoperatively, apply a bulky, non-compressive soft dressing reinforced with a custom-molded volar plaster or fiberglass splint.
* For the Barsky and Millesi techniques, the affected digit must be strictly immobilized to protect the osteosynthesis.
* Elevate the extremity strictly for the first 48 to 72 hours to mitigate edema.
Phase II: Pin Removal and Early Motion (Weeks 4-6)
* Radiographs are obtained at 3 to 4 weeks to assess callus formation and consolidation at the osteotomy/arthrodesis sites.
* Once clinical and radiographic union is evident, the K-wires are removed in the clinic.
* Initiate active range of motion (AROM) of the uninvolved joints. For the Barsky technique, DIP motion is permanently lost, but aggressive therapy is required to prevent stiffness in the proximal interphalangeal (PIP) and MCP joints.
Phase III: Strengthening and Integration (Weeks 6-12)
* Transition to passive range of motion (PROM) and dynamic splinting if joint contractures are noted.
* Begin progressive resistance exercises, focusing on pinch strength and functional grasp.
* Scar massage and silicone gel sheeting are employed to manage the surgical incisions, particularly the L-shaped flaps which are prone to hypertrophy.
COMPLICATIONS AND PITFALLS
Orthopedic surgeons undertaking these complex reconstructions must be vigilant regarding potential complications:
- Vascular Compromise: The most devastating complication. Over-resection of bone or aggressive soft tissue debulking can stretch or sever the delicate digital neurovascular bundles. Always release the tourniquet prior to final closure to confirm robust capillary refill.
- Nonunion/Delayed Union: The "pencil-cone" arthrodesis in the Barsky technique requires precise bony apposition. Inadequate preparation of the medullary canal or thermal necrosis from a high-speed burr can lead to nonunion.
- Nail Deformities: In the Millesi technique, failure to respect the germinal matrix will result in a split, ridged, or absent nail, leading to significant cosmetic dissatisfaction and potential functional tenderness.
- Infection: Pin tract infections are common with exposed K-wires. Meticulous pin site care with chlorhexidine or dilute peroxide is mandatory until pin extraction.
Pitfall: Attempting a single-stage bone shortening and massive soft-tissue debulking simultaneously dramatically increases the risk of digital ischemia. Always stage the soft tissue debulking 3 to 6 months after the osseous framework has healed.
By adhering to strict biomechanical principles, utilizing precise surgical techniques, and respecting the delicate vascular anatomy of the pediatric hand, the orthopedic surgeon can successfully navigate the complexities of congenital undergrowth deformities and restore both form and function to the afflicted upper extremity.
📚 Medical References
- Hypoplastic Thumb Ab del-Ghani H, Amro S: Characteristics of patients with hypoplastic thumb: a prospective study of 51 patients with the results of surgical treatment, J Pediatr Orthop B 13:127, 2004.
- Bayne LG: Abducted thumb (congenital hand deformities). In Green DP, ed: Operative hand surgery, New York, 1988, Churchill Livingstone. Blair WF, Omer GE Jr: Anomalous insertion of the fl exor pollicis longus, J Hand Surg 6A:241, 1981.
- Blauth W: The hypoplastic thumb, Arch Orthop Unfallchir 62:225, 1967.
- Blauth W, Schneider-Sickert F: Congenital deformities of the hand: an atlas on their surgical treatment, New York, 1981, Springer-Verlag. Bonatz E, Masear VR, Meyer RD, et al: Degenerative arthritis of the carpus associated with congenital hypoplastic thumb, J Hand Surg 14A:734, 1989.
- Brand PW, Milford LW: Web deepening with sliding fl ap for adducted thumb in the hand. In Crenshaw AH, ed: Campbell’s operative orthopaedics, 4th ed, St Louis, 1963, Mosby. Broadbent TR, Woolf RM: Flexion-abduction deformity of the thumb:
You Might Also Like