Subcutaneous Fasciotomy for Dupuytren Contracture

Key Takeaway
Subcutaneous fasciotomy is a minimally invasive surgical technique primarily indicated for the release of well-defined pretendinous cords in Dupuytren contracture. By selectively dividing the pathological palmar fascia, surgeons can restore metacarpophalangeal joint extension with minimal morbidity. This guide details the biomechanical principles, precise surgical steps—including the Luck technique and Z-plasty flap design—and postoperative rehabilitation protocols essential for optimizing functional outcomes and minimizing neurovascular complications.
INTRODUCTION TO SUBCUTANEOUS FASCIOTOMY
Dupuytren disease is a progressive, fibroproliferative disorder of the palmar fascia that leads to debilitating flexion contractures of the digits. While formal fasciectomy remains the gold standard for extensive disease, subcutaneous fasciotomy (often referred to as the Luck procedure or percutaneous needle aponeurotomy in modern iterations) serves as a highly effective, minimally invasive alternative for carefully selected patients.
The primary objective of a subcutaneous fasciotomy is to mechanically disrupt the pathological pretendinous cord, thereby restoring metacarpophalangeal (MCP) joint extension without the morbidity associated with extensive skin flaps and wide fascial excision. This technique is particularly advantageous for elderly patients, those with significant medical comorbidities, or individuals seeking rapid return to function with isolated, well-defined cords.
This comprehensive guide details the pathoanatomy, biomechanical principles, and step-by-step surgical execution of both the closed subcutaneous cordotomy and the limited open fasciotomy utilizing Z-plasty principles.
PATHOANATOMY AND BIOMECHANICS
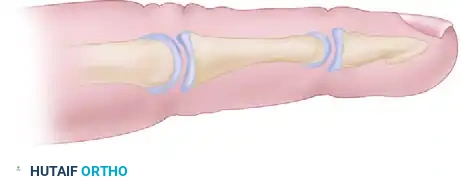
A profound understanding of the palmar fascial anatomy is mandatory to safely perform a subcutaneous fasciotomy. The normal palmar fascia consists of longitudinal, transverse, and vertical fibers that stabilize the palmar skin and protect underlying neurovascular structures. In Dupuytren disease, normal fascial bands hypertrophy and contract to become pathological cords.
The Pretendinous Cord
The pretendinous band, which normally inserts into the skin and the base of the proximal phalanx, transforms into the pretendinous cord. This structure is primarily responsible for MCP joint contractures. Because the pretendinous cord lies superficial to the neurovascular bundles, it is highly amenable to subcutaneous division.
The Spiral Cord
The spiral cord is the most critical anatomical structure to identify, as it is responsible for proximal interphalangeal (PIP) joint contractures and poses the greatest risk to the digital nerve. Formed by the amalgamation of the pretendinous band, spiral band, lateral digital sheet, and Grayson’s ligament, the spiral cord contracts and displaces the neurovascular bundle centrally, proximally, and superficially.
Surgical Warning: Blind subcutaneous fasciotomy is generally contraindicated for severe PIP joint contractures due to the high risk of transecting a superficially displaced digital nerve intertwined with a spiral cord.
INDICATIONS AND CONTRAINDICATIONS
Indications
- Well-defined, palpable pretendinous cord.
- Isolated MCP joint contracture greater than 30 degrees.
- Elderly patients or those with severe medical comorbidities precluding prolonged anesthesia.
- Patients requiring rapid postoperative recovery.
Contraindications
- Rapidly progressive, aggressive diathesis (e.g., early onset, bilateral involvement, ectopic deposits).
- Severe PIP joint contractures (due to the risk of neurovascular injury).
- Recurrent disease in a previously operated field (scar tissue obscures neurovascular anatomy).
- Ill-defined, diffuse fascial thickening without a discrete cord.
PREOPERATIVE PLANNING AND ANESTHESIA
Thorough preoperative assessment includes measuring the exact degree of MCP and PIP joint contractures using a goniometer. The skin should be inspected for deep pits, nodules, and areas of diminished vascularity, as these will dictate incision placement if an open technique is required.
Anesthetic Considerations
Subcutaneous fasciotomy can frequently be performed under local anesthesia with epinephrine (Wide Awake Local Anesthesia No Tourniquet - WALANT). This allows the surgeon to assess active tendon excursion intraoperatively and ensures the patient can report any paresthesias, adding a layer of safety regarding the digital nerves.
If a limited open fasciotomy (Technique 75-2) is planned, regional anesthesia (axillary or supraclavicular block) combined with a well-padded pneumatic arm tourniquet is preferred to provide a bloodless surgical field.
SURGICAL TECHNIQUE: SUBCUTANEOUS CORDOTOMY (LUCK TECHNIQUE)
The Luck subcutaneous fasciotomy relies on the precise, controlled division of the pretendinous cord using a small scalpel blade or fasciotome.
Step 1: Positioning and Preparation
The patient is positioned supine with the operative arm extended on a hand table. The hand is prepped and draped in a standard sterile fashion. The palpable cord is marked. In this classic example, we address a well-defined pretendinous cord in the ring finger causing a 60-degree MCP joint contracture.
Step 2: Blade Insertion
A No. 15 scalpel blade (or a specialized fasciotome) is utilized. The blade is introduced through the skin directly over or slightly lateral to the palpable cord.
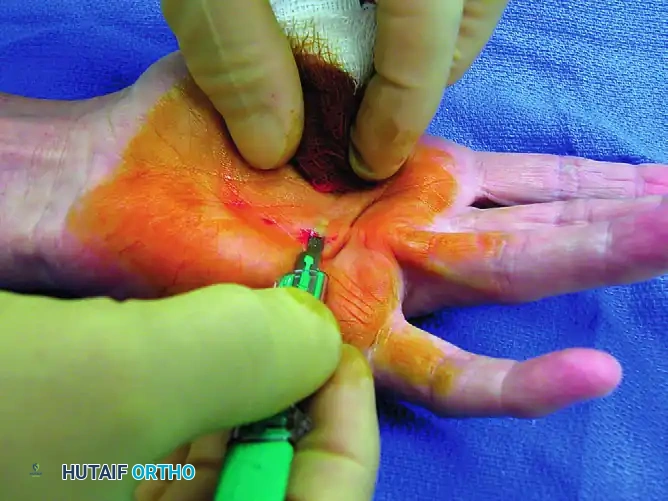
The blade is inserted flat, parallel to the skin surface, passing between the dermis and the superficial aspect of the pretendinous cord. It is imperative that the blade remains strictly superficial to the cord to avoid inadvertent injury to the underlying flexor tendons or adjacent neurovascular bundles.
Step 3: Cross-Sectional Anatomy and Orientation
Understanding the cross-sectional anatomy at the level of the metacarpal is vital. The palmar fascia lies superficial to the flexor tendons and neurovascular bundles.
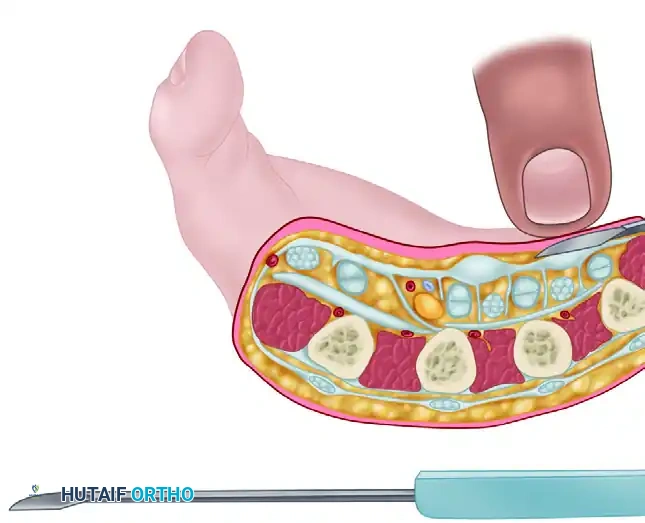
Once the blade is positioned between the skin and the cord, the cutting edge is rotated 90 degrees so that it faces the pathological tissue.

Step 4: Forceful Extension and Cordotomy
With the blade held firmly at a 90-degree angle to the tight cord, the surgeon applies forceful passive extension to the affected digit.
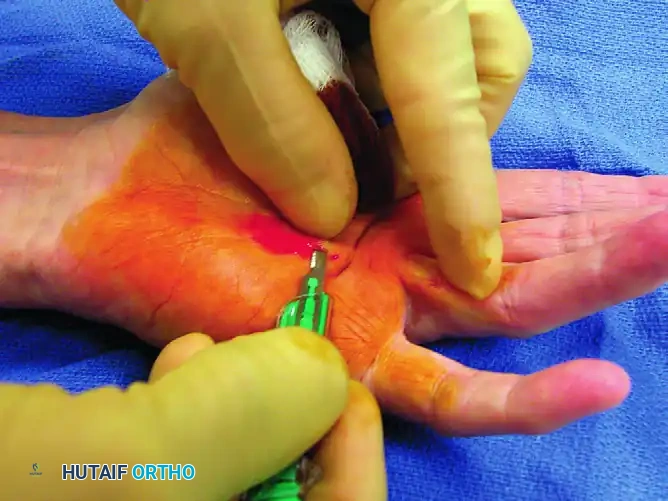
This forceful extension effectively delivers the abnormal cord superficially, pressing it directly onto the stationary scalpel blade. The tension causes the cord to yield and snap against the sharp edge. The surgeon should feel a distinct "give" as the fascial fibers part.
Clinical Pearl: Do not use a sawing motion with the scalpel. The blade should remain relatively stationary while the passive extension of the finger drives the taut cord into the cutting edge. This minimizes the risk of collateral damage.
Step 5: Assessment of Release
Following the release, the resultant MCP joint extension is evaluated.

If residual contracture remains, the process may be repeated at a slightly different level (usually more proximally in the palm). Multiple small percutaneous releases are safer and more effective than attempting a single massive division.
SURGICAL TECHNIQUE 75-2: LIMITED OPEN FASCIOTOMY WITH Z-PLASTY
When the skin is heavily involved, pitted, or when the cord is too diffuse for a safe blind release, a limited open fasciotomy is indicated. This approach allows for direct visualization of the neurovascular structures and management of skin contractures via Z-plasty.
Step 1: Incision Planning
Outline the proposed incision with a surgical marking pen prior to the inflation of the tourniquet.
* Skin Pits: Take into consideration the pits and other areas of skin with diminished vascularity. Plan the incision over or near these areas, strictly avoiding placing them at the base of a planned skin flap, which could lead to ischemic necrosis. These pitted areas can sometimes be excised during the final rotation of the skin flaps.
* Incision Geometry: Make a zigzag or vertical incision directly over the deforming pathological structure. While zigzag incisions (Bruner type) tend to straighten out and cause tension lines at the creases, the triangular flaps created by them often heal more securely and provide excellent exposure.
* Z-Plasty Design: If a straight vertical incision is used, design Z-plasty flaps so that the transverse segment of the "Z" will fall within or near each joint crease. Continue the incision proximally into the palm, strictly avoiding crossing the palmar creases at right angles to prevent secondary scar contractures.
Step 2: Flap Elevation
Elevate the skin and underlying normal subcutaneous tissue away from the pathological fascia, working from proximal to distal. The skin in Dupuytren disease is often intimately involved with the fascia; meticulous sharp dissection is required to avoid buttonholing the dermis. Leave the creation of the actual Z-plasty transpositions until the wound is ready for closure.
Step 3: Fascial Excision and Neurovascular Protection
Excise the pathological fascia from proximal to distal.
Surgical Warning: The most critical step of this procedure is the isolation and protection of the neurovascular bundles. Always locate the digital nerve in the normal, unscarred fatty pad at the level of the mid-palm or MCP joint before tracing it distally into the diseased tissue.
- Carefully excise the pathological fascia by sharp dissection.
- Excision of the superficial transverse palmar fascial fibers is generally unnecessary unless they are directly contributing to the contracture.
- Avoid entering the flexor tendon sheaths. Bleeding into the flexor tendon sheaths can cause severe postoperative adhesions, severely limiting active range of motion.
- If the natatory ligament is contracted (preventing finger abduction), it must be systematically excised.
Step 4: Distal Dissection
Follow all contracted fascial cords to their distal insertions. These insertions may attach into the tendon sheaths, the periosteum of the bone, or the deep dermis of the skin. Occasionally, cords will spiral dorsolaterally to the PIP joint. Ensure all deforming forces are released.
Step 5: Verification of Release
When the excision of the diseased tissue has been completed, all involved joints should permit full passive extension. If full extension is not achieved, reassess for residual fascial bands. If the fascia is completely cleared and a contracture persists, it is likely due to secondary capsular contractures (e.g., volar plate contracture), which may require separate capsulotomy if deemed clinically necessary.
Step 6: Hemostasis
Before closing the wound, meticulous hemostasis is mandatory to prevent postoperative hematoma, which is a primary catalyst for stiffness, infection, and severe flare reactions.
* Elevate the hand.
* Apply compressive gauze to the wound.
* Release the pneumatic tourniquet.
* Hold direct, firm pressure for a full 10 minutes by the clock.
* After 10 minutes, gently remove the compression and carefully cauterize any remaining small bleeding points using bipolar electrocautery.
Step 7: Flap Fashioning and Closure
Fashion the skin flaps according to the preoperative Z-plasty design. If there is redundant skin, or if pitted/thinned areas remain at the margins, they can be sharply excised at this stage.
Using skin hooks to ensure minimal handling and trauma to the delicate flap edges, suture the flaps in place. Use 4-0 or 5-0 monofilament nylon with interrupted sutures. Ensure there is no undue tension on the flap tips, as this will lead to marginal necrosis.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The success of a fasciotomy relies as much on postoperative rehabilitation as it does on surgical execution.
Immediate Postoperative Care
- A bulky, non-adherent compressive dressing is applied in the operating room.
- A volar plaster splint is applied with the wrist in neutral and the MCP joints in maximal comfortable extension. The PIP joints should be left free if they were not involved, or splinted in extension if released.
- The hand must be kept strictly elevated above heart level for the first 48 to 72 hours to minimize edema.
Hand Therapy and Splinting
- Days 3-5: The bulky dressing is removed. A custom thermoplastic extension splint is fabricated by a certified hand therapist.
- Active and active-assisted range of motion exercises for flexion and extension are initiated immediately to prevent tendon adhesions.
- Weeks 1-4: The extension splint is worn continuously, removed only for hygiene and structured exercise sessions.
- Weeks 4-12: Splint wear is gradually reduced to nighttime only. Night splinting may be continued for up to 3 to 6 months to prevent early recurrence of the contracture.
COMPLICATIONS AND PITFALLS
While subcutaneous and limited open fasciotomies are highly effective, they carry specific risks that the orthopedic surgeon must anticipate and mitigate.
- Digital Nerve Injury: The most devastating complication. Risk is highest when addressing PIP contractures or spiral cords. Prevention relies on proximal identification of the nerve and avoiding blind percutaneous releases in the digits.
- Hematoma Formation: Can lead to skin flap necrosis, infection, and severe postoperative stiffness. Strict adherence to the 10-minute post-tourniquet compression rule is essential.
- Skin Necrosis: Often results from placing incisions through avascular skin pits, creating flaps with inadequate bases, or closing under excessive tension. Z-plasty helps mitigate tension lines.
- Recurrence: Dupuytren disease is incurable. Subcutaneous fasciotomy has a higher recurrence rate than formal fasciectomy. Patients must be counseled preoperatively that the procedure is a management strategy, not a definitive cure, and that future interventions may be required.
- Flare Reaction: A hyperactive inflammatory response characterized by diffuse swelling, redness, and stiffness. Treated with aggressive hand therapy, continuous elevation, and occasionally a short course of oral corticosteroids.
By adhering to strict anatomical principles, careful patient selection, and meticulous surgical technique, the orthopedic surgeon can utilize subcutaneous fasciotomy to safely and effectively restore hand function in patients suffering from Dupuytren contracture.
📚 Medical References
- subcutaneous fasciotomy for chronic exertional compartment syndrome of the lower extremity, Am J Orthop 33:42, 2004.
- Rupture of Muscles and Tendons and Tendinitis Aarimaa V, Rantanen J, Heikkila J, et al: Rupture of the pectoralis major muscle, Am J Sports Med 32:1256, 2004.
- Abraham E, Pankovich AM: Neglected rupture of the Achilles tendon: treatment by V-Y tendinous fl ap, J Bone Joint Surg 57A:253, 1975.
- Agins HJ, Chess JL, Hoekstra DV, et al: Rupture of the distal insertion of the biceps brachii tendon, Clin Orthop Relat Res 234:34, 1989.
- Almenkinders LC, Garrett WE Jr, Seaber AV: Histopathology of muscle tears in stretching injuries, Trans Orthop Res Soc 9:306, 1984.
- Anderson E: Stenosing peroneal tenosynovitis symptomatically simulating ankle instability, Am J Sports Med 15:258, 1987.
- Assal M, Jung M, Stern R, et al: Limited open repair of
You Might Also Like