Surgical Management of Distal Radius and Forearm Malunions
Key Takeaway
Distal radius and forearm malunions frequently result in significant biomechanical derangement, leading to pain, restricted motion, and distal radioulnar joint (DRUJ) instability. While conservative management suffices for low-demand patients, symptomatic malunions in active individuals necessitate precise surgical correction. This guide details the indications, preoperative 3D planning, corrective osteotomy techniques, and DRUJ reconstruction protocols required to restore native wrist kinematics and optimize functional outcomes.
INTRODUCTION TO DISTAL RADIUS MALUNION
Despite profound advancements in fracture fixation techniques and implant technology since the early 1980s, malunion remains a prevalent and challenging cause of residual disability following distal radial fractures. Historically, the medical community relied on Abraham Colles’ classic 1814 observation, which posited that while the visible deformity of a distal radius fracture would persist, the wrist would eventually “enjoy perfect freedom in all its motions and be completely exempt from pain.”
Modern biomechanical and clinical investigations have unequivocally refuted this historical assertion. We now understand that anatomical distortion at the radiocarpal and distal radioulnar joints (DRUJ) fundamentally alters load transmission, leading to accelerated arthrosis, midcarpal instability, and significant functional impairment. However, it is critical to recognize that not all distal radial malunions are symptomatic. In elderly patients with low functional demands, a malunion may be well-tolerated, and in such cohorts, no further surgical treatment is indicated. Conversely, posttraumatic wrist deformities in younger, active patients are frequently disabling enough to warrant complex surgical correction. Contemporary outcome studies demonstrate that malunion is independently associated with higher arm-related disability scores (e.g., DASH and PRWE), regardless of the patient's chronological age, emphasizing physiological demand over age alone.
Fracture characteristics (e.g., severe initial comminution, intra-articular extension) and the chosen initial treatment modality heavily contribute to the development of a malunion. Ultimately, malunion is the direct result of a failure to achieve an accurate anatomical reduction or a failure to maintain that reduction throughout the bone healing phase.
PATHOMECHANICS AND BIOMECHANICAL DERANGEMENT
To master the surgical correction of a distal radius malunion, the orthopaedic surgeon must possess a profound understanding of normal wrist biomechanics and the consequences of spatial distortion.
Normal Radiographic Parameters
- Radial Inclination: Averages 22 degrees (range, 13 to 30 degrees).
- Volar Tilt: Averages 11 degrees (range, 1 to 21 degrees).
- Radial Height: Averages 11 to 12 mm.
- Ulnar Variance: Neutral (0 mm), though highly dependent on grip and forearm rotation.
Consequences of Deformity
When a fracture heals in a dorsally angulated position (the classic Colles-type malunion), the biomechanical consequences are severe:
1. Altered Load Transmission: Normal load distribution across the wrist is approximately 80% through the radiocarpal joint and 20% through the ulnocarpal joint. A dorsal tilt exceeding 20 degrees shifts up to 50% of the axial load onto the ulna and the triangular fibrocartilage complex (TFCC), leading to ulnar-sided wrist pain and TFCC degeneration.
2. Kinematic Dysfunction: Dorsal angulation alters the resting posture of the carpus, frequently inducing a dorsal intercalated segment instability (DISI) deformity. This limits palmar flexion and weakens grip strength.
3. DRUJ Incongruity: Loss of radial height and altered volar/dorsal tilt distort the sigmoid notch's relationship with the ulnar head. This incongruity restricts forearm pronation and supination and is a primary driver of DRUJ arthrosis.
Clinical Pearl: A loss of radial height greater than 2 mm or a dorsal tilt exceeding 10 degrees past neutral are the most critical radiographic thresholds associated with symptomatic DRUJ instability and ulnocarpal abutment.
CLINICAL AND RADIOGRAPHIC EVALUATION
Patient Assessment
A meticulous history and physical examination are paramount. The surgeon must differentiate between radiocarpal pain (often dorsal and exacerbated by extension/loading) and DRUJ/ulnocarpal pain (exacerbated by forearm rotation and ulnar deviation).
* Range of Motion (ROM): Document precise arcs of flexion/extension and pronation/supination.
* Grip Strength: Compare to the contralateral, uninjured extremity using a Jamar dynamometer.
* Provocative Testing: Perform the DRUJ ballottement test in neutral, full pronation, and full supination to assess stability. Evaluate for ulnocarpal impaction using the ulnocarpal stress test.
Imaging Protocols
- Standard Radiographs: Posteroanterior (PA), lateral, and oblique views of both wrists. Contralateral views are essential to establish the patient's native anatomical baseline.
- Computed Tomography (CT): A fine-cut CT scan with 3D reconstructions is mandatory for surgical planning. It delineates intra-articular step-offs, the exact plane of the deformity, and the congruity of the sigmoid notch.
- Magnetic Resonance Imaging (MRI): Reserved for cases with suspected concomitant soft-tissue pathology, such as high-grade TFCC tears or scapholunate ligament ruptures.
INDICATIONS AND CONTRAINDICATIONS FOR SURGERY
Indications
- Symptomatic malunion (pain, weakness, restricted ROM) in a physiologically active patient.
- Extra-articular malunions with >15 degrees of dorsal tilt, >20 degrees of volar tilt, or >3 mm of radial shortening.
- Intra-articular malunions with >2 mm step-off or gap.
- Secondary DRUJ instability or ulnocarpal impaction directly attributable to the radial deformity.
Contraindications
- Asymptomatic malunions in low-demand or elderly patients.
- Advanced radiocarpal or midcarpal osteoarthritis (salvage procedures such as total wrist arthrodesis or proximal row carpectomy are more appropriate).
- Active infection or severe complex regional pain syndrome (CRPS).
PREOPERATIVE PLANNING AND 3D MODELING
Modern corrective osteotomy relies heavily on computer-assisted 3D planning. By superimposing the mirrored CT image of the contralateral (normal) wrist onto the malunited wrist, the surgeon can precisely calculate the required angles of correction in the sagittal, coronal, and axial planes.
Patient-specific instrumentation (PSI), including 3D-printed cutting guides and pre-contoured plates, has revolutionized this procedure. These guides ensure the osteotomy is performed at the exact planned location and trajectory, minimizing intraoperative guesswork and reducing fluoroscopy time.
SURGICAL TECHNIQUE: DISTAL RADIUS CORRECTIVE OSTEOTOMY
Patient Positioning and Setup
The patient is placed supine with the operative arm extended on a radiolucent hand table. A well-padded proximal tourniquet is applied. Prophylactic intravenous antibiotics are administered prior to inflation. The C-arm fluoroscope is positioned parallel to the table to allow seamless PA and lateral imaging.
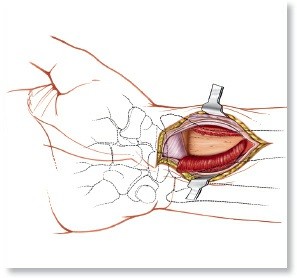
The Volar Approach (Modified Henry)
For the majority of dorsally and volarly angulated malunions, a volar approach is preferred due to the robust soft-tissue coverage it provides for the implant and the ability to release the deforming forces of the brachioradialis.
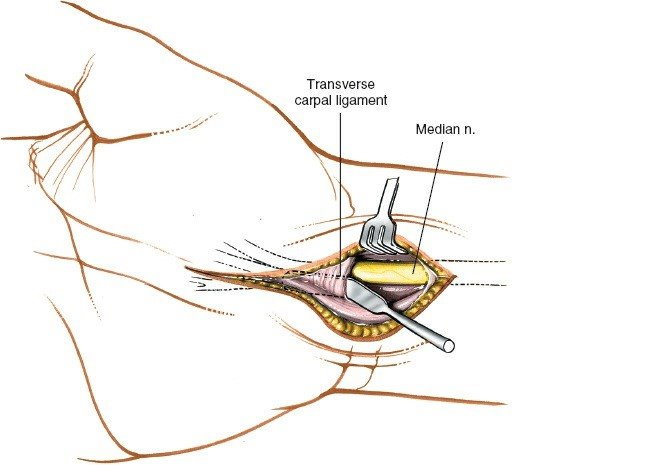
- Incision: A longitudinal incision is made over the flexor carpi radialis (FCR) tendon, extending proximally from the wrist crease.
- Superficial Dissection: The FCR sheath is incised, and the tendon is retracted ulnarly. The flexor pollicis longus (FPL) and the median nerve are protected and retracted ulnarly.
- Deep Dissection: The pronator quadratus (PQ) is identified. An L-shaped incision is made along the radial and distal borders of the PQ, and the muscle is elevated off the radius as a full-thickness flap.
- Brachioradialis Release: This is a critical step. The brachioradialis tendon insertion on the radial styloid must be completely released to mobilize the distal fragment and allow for restoration of radial length and inclination.
Surgical Warning: Failure to adequately release the brachioradialis and the first dorsal compartment will result in immense difficulty when attempting to distract the osteotomy site to restore radial length, often leading to hardware failure or loss of fixation.
Osteotomy and Deformity Correction
- Guidewire Placement: Using 3D-printed guides or fluoroscopic guidance, K-wires are placed parallel to the articular surface in both the AP and lateral planes.
- The Cut: An oscillating saw is used to perform the osteotomy parallel to the joint surface, typically at the site of the original fracture (the apex of the deformity). Copious saline irrigation is used to prevent thermal necrosis.
- Mobilization: Osteotomes and lamina spreaders are utilized to gently open the osteotomy site. The distal fragment is manipulated to restore volar tilt, radial inclination, and radial height.
- Temporary Fixation: Once anatomical alignment is confirmed via fluoroscopy, the reduction is provisionally held with K-wires.
Structural Grafting and Fixation
An opening wedge osteotomy creates a void that must be managed to ensure structural stability and bone healing.
* Graft Selection: For defects larger than 5 mm, structural autograft (tricortical iliac crest) remains the gold standard. For smaller defects, cancellous allograft, demineralized bone matrix (DBM), or synthetic bone substitutes (e.g., calcium phosphate cement) may be utilized.
* Plating: A volar locking plate is applied. The distal locking screws are placed subchondrally to support the articular surface. The proximal cortical screws are then inserted to secure the plate to the radial shaft.
* Closure: The PQ is loosely reapproximated over the plate to protect the flexor tendons. The skin is closed in layers.
FOREARM MALUNIONS WITH DRUJ INSTABILITY
Pathoanatomy of Diaphyseal Malunion
Malunions of fractures involving the radial shaft or both bones of the forearm can cause profound instability and incongruity at the distal radioulnar joint. This biomechanical disaster occurs most frequently with fractures located in the distal third of the forearm.
The radius normally possesses a complex lateral and dorsal bow that allows it to rotate around the fixed ulna during pronation and supination. A malunion that alters this radial bow, or one that results in a significant length discrepancy between the radius and ulna, will inevitably tether the interosseous membrane and distort the DRUJ. The ulnar head may subluxate dorsally or volarly, leading to painful impingement, restricted rotation, and eventual destruction of the TFCC.
Surgical Decision-Making
The management of DRUJ instability secondary to forearm malunion is highly nuanced. The primary goal is to restore the anatomical relationship of the radius and ulna.
* Corrective Osteotomy Alone: In many instances, a precise corrective osteotomy of the deformed diaphyseal bone (restoring length, alignment, and rotation) is all that is necessary to spontaneously restore stability to the DRUJ.
* Osteotomy with DRUJ Reconstruction: In chronic cases where the soft tissues (capsule and TFCC) have become permanently attenuated or contracted, restoring bony anatomy alone is insufficient. In these cases, capsular imbrication, TFCC repair, and temporary transfixion of the DRUJ are required.
Clinical Evidence and Outcomes
The complexity of these combined injuries is well-documented in the literature. Trousdale and Linscheid evaluated six patients presenting with forearm malunions and associated instability of the DRUJ.
* In three patients, stability of the DRUJ was successfully obtained by osteotomy and rigid plate fixation of the bony deformity alone.
* The remaining three patients required additional soft-tissue reconstruction of the DRUJ.
The outcomes of this study highlight both the efficacy and the inherent risks of the procedure. A stable wrist was obtained in five of the six patients. However, four patients lost some degree of forearm motion (ranging from a 25-degree loss to a 25-degree gain). Complications were noted in three patients, including mild residual instability of the ulna, mild wrist pain, and pain in the radial nerve distribution.
DRUJ Reconstruction Techniques
When diaphyseal osteotomy alone fails to stabilize the DRUJ intraoperatively, the surgeon must proceed with joint reconstruction:
1. Capsular Imbrication: A dorsal approach to the DRUJ is utilized. The extensor retinaculum is opened over the fifth compartment (EDQ). The dorsal radioulnar capsule is incised, and redundant tissue is excised or imbricated (overlapped and sutured) to tighten the joint.
2. TFCC Repair: If a peripheral tear of the TFCC is identified, it is repaired back to the fovea of the ulnar head using suture anchors or transosseous tunnels.
3. Temporary Transfixion: To protect the soft-tissue repair, the forearm is placed in neutral rotation or slight supination (the position of maximum DRUJ stability), and one or two 0.062-inch K-wires are driven transversely from the ulna into the radius just proximal to the DRUJ. These wires are typically removed at 4 to 6 weeks postoperatively.
Pitfall: Pinning the DRUJ in extreme pronation or supination can lead to severe postoperative stiffness. Always pin the joint in a neutral or slightly supinated position where the capsule is under balanced tension.
POSTOPERATIVE REHABILITATION PROTOCOL
Successful outcomes depend as much on postoperative rehabilitation as on surgical execution.
* Phase 1 (0-2 weeks): The wrist is immobilized in a bulky plaster splint. Immediate active ROM of the digits, elbow, and shoulder is initiated to prevent stiffness and reduce edema.
* Phase 2 (2-6 weeks): Sutures are removed. If the DRUJ was not pinned, the patient is transitioned to a removable custom orthosis, and gentle active wrist ROM and forearm rotation begin under the guidance of a certified hand therapist. If DRUJ transfixion wires are present, forearm rotation is strictly prohibited until pin removal.
* Phase 3 (6-12 weeks): Transfixion pins (if used) are removed. Progressive strengthening and passive stretching are initiated. Dynamic splinting may be employed if stiffness persists.
* Phase 4 (12+ weeks): Return to heavy lifting and high-impact activities is permitted once radiographic union is confirmed and functional strength is restored.
COMPLICATIONS AND OUTCOMES
While corrective osteotomy significantly improves pain and function in the majority of patients, it is a technically demanding procedure with a recognized complication profile.
* Hardware Complications: Tendon irritation or rupture (particularly the FPL volarly or the EPL dorsally) can occur if plates are positioned past the watershed line or if screws protrude dorsally.
* Neurological Injury: Transient neurapraxia of the superficial radial nerve or the median nerve can occur due to traction during the approach or deformity correction.
* Nonunion/Delayed Union: More common in cases with large structural defects, inadequate fixation, or patient non-compliance (e.g., smoking).
* Residual Stiffness: As noted in the Trousdale and Linscheid series, some loss of terminal ROM is common, particularly in pronation and supination following DRUJ reconstruction. Patients must be counseled preoperatively that the goal is a functional, pain-free arc of motion, not necessarily a return to normal baseline kinematics.
You Might Also Like