The Medial Open Reduction Approach: Keys to Success

Key Takeaway
This topic focuses on The Medial Open Reduction Approach: Keys to Success, Medial open reduction is a surgical technique for developmentally dislocated hips in babies, typically those 12 months or younger. It is used when closed reduction has failed or is unstable. This approach addresses anatomical impediments like the iliopsoas tendon, constricted capsule, and infolded labrum, aiming to achieve stable hip reduction.
Introduction and Epidemiology
Developmental dysplasia of the hip (DDH) encompasses a spectrum of pathology ranging from mild acetabular dysplasia to frank, irreducible dislocation of the femoral head. Epidemiological data indicate that DDH occurs in approximately 1.5 babies per 1000 live births, though the incidence of clinical instability in the newborn period is higher, often resolving spontaneously. When diagnosed in the newborn period, closed treatment utilizing the Pavlik harness is highly efficacious, demonstrating a 95% success rate in dysplastic hips and up to an 80% success rate in frankly dislocated hips.

The pathogenesis of DDH is multifactorial, involving both mechanical and genetic variables. It is significantly more common in female infants and is strongly linked with intrauterine mechanical factors such as breech presentation, oligohydramnios, and primigravida status (first-born children). DDH is also associated with other packaging disorders, including congenital knee hyperextension, congenital muscular torticollis, clubfoot, and metatarsus adductus. A positive family history is present in a minority of patients and most likely represents a genetic predisposition toward familial hyperlaxity. It is critical for the orthopedic surgeon to differentiate idiopathic DDH from teratologic hip dislocations, which are observed in infants with underlying neuromuscular or syndromic disorders such as arthrogryposis multiplex congenita and Larsen syndrome. Teratologic hips are typically refractory to closed management and require extensive surgical intervention.

The natural history of untreated DDH is highly variable. While ultrasonographic evidence of mild dysplasia in the newborn often resolves spontaneously without intervention, there is a significant and documented risk that babies with dislocatable or actively dislocated hips will progress to fixed dislocations. The physical examination is the cornerstone of early diagnosis. A positive Ortolani sign represents the reduction of a dislocated hip and is typically present in the newborn period, but this sign disappears as the soft tissues contract and the dislocation becomes fixed. Conversely, a positive Barlow sign represents the ability to dislocate a reduced but unstable hip. As the child ages and the dislocation becomes fixed, limited hip abduction during range-of-motion testing becomes the hallmark clinical sign. The Galeazzi sign (asymmetric knee height) is useful for unilateral dislocations, though apparent femoral lengths will remain equal in bilateral dislocations. Extra thigh folds may be present in unilateral DDH, but thigh fold asymmetry is a nonspecific finding.
Surgical Anatomy and Biomechanics
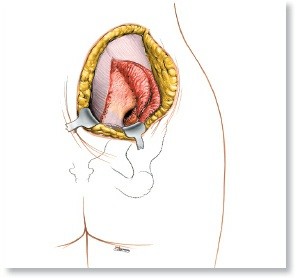
A thorough understanding of the regional anatomy is paramount for executing the medial approach to the hip safely and effectively. The primary objective of the open reduction is to clear the anatomical blocks to reduction, allowing the femoral head to seat concentrically within the true acetabulum without excessive tension.

Reduction of a dislocated hip is typically impeded by a predictable sequence of anatomical structures:
1. The Iliopsoas Tendon: As the femoral head migrates superolaterally, the iliopsoas tendon is drawn tightly across the anterior and inferior capsule, creating an hourglass constriction that physically blocks the reentry of the femoral head.
2. The Inferomedial Hip Capsule: The capsule itself becomes thickened, contracted, and adherent to the side of the ilium, further contributing to the hourglass deformity.
3. The Transverse Acetabular Ligament (TAL): This ligament spans the inferior aspect of the acetabular horseshoe. In DDH, it hypertrophies and is pulled superiorly, acting as a tension band that prevents inferomedial seating of the femoral head.
4. The Pulvinar: This fibrofatty tissue hypertrophies to occupy the void within the cavity of the true acetabulum, acting as a physical space-occupying lesion.
5. The Acetabular Labrum: The superior labrum can become blunted and infolded (often referred to as the neolimbus), serving as a mechanical doorstop that blocks deep and medial reduction.
6. The Ligamentum Teres: This structure often becomes significantly hypertrophied, elongated, and redundant, further occupying critical volume within the acetabular fossa.

The medial approach exploits the internervous and intermuscular planes of the medial thigh to access the inferior capsule directly. The critical anatomic landmarks and structures include:
* Adductor Longus: Originating on the pubis, this muscle serves as the primary superficial landmark for the incision.
* Pectineus: Lying anterior to the adductor brevis (which is situated deep to the adductor longus), the pectineus forms the floor of the femoral triangle.
* Femoral Neurovascular Bundle: The femoral artery, vein, and nerve are located as a contiguous bundle anterior to the pectineus muscle. Retraction of these structures is a critical step.
* Medial Femoral Circumflex Artery (MFCA): This is the most critical structure at risk during the medial approach. The MFCA lies in the interval between the pectineus and the iliopsoas/femoral neurovascular bundle. It provides the dominant blood supply to the developing ossific nucleus of the proximal femur. Iatrogenic injury to the MFCA leads to devastating avascular necrosis (AVN) of the femoral head.
Indications and Contraindications
The medial approach is a highly specialized technique utilized primarily in the young infant. Closed reduction is indicated when Pavlik harness treatment has failed or when the initial presentation for treatment is delayed past 6 months of age. Open reduction is strictly reserved for babies in whom closed reduction under general anesthesia is either unobtainable, requires excessive abduction (the "safe zone" of Ramsey is unachievable), or lacks stability.
The medial approach is most frequently employed in infants aged 12 months or less. Beyond 18 to 24 months of age, the medial approach is generally contraindicated because older children typically require a concomitant pelvic osteotomy (e.g., Salter or Pemberton) and a formal capsulorrhaphy to address secondary bony dysplasia and capsular redundancy. The medial approach does not provide the requisite superior access for these procedures; thus, an anterior (Smith-Petersen) approach is mandated in older toddlers.
| Parameter | Operative Management (Medial Open Reduction) | Non Operative Management (Closed Reduction) |
|---|---|---|
| Age at Intervention | 6 to 18 months (optimal < 12 months) | 6 to 18 months |
| Prior Treatment | Failed Pavlik harness or failed closed reduction | Failed Pavlik harness, delayed presentation |
| Intraoperative Findings | Unstable in acceptable "safe zone" (requires >60° abduction) | Stable reduction achieved within Ramsey's safe zone |
| Anatomical Blocks | Inverted labrum, tight TAL, hypertrophied pulvinar identified on arthrogram | Minimal mechanical blocks, dye pools medially but clears with gentle reduction |
| Concomitant Procedures | Iliopsoas tenotomy, adductor tenotomy | Adductor tenotomy (frequently performed percutaneously) |
| Contraindications | Age > 18-24 months, need for pelvic osteotomy, severe teratologic dislocation | Teratologic dislocation, rigid neuromuscular contractures |
Pre Operative Planning and Patient Positioning
Preoperative planning relies heavily on high-quality imaging. In infants younger than 6 months, dynamic ultrasound is the gold standard for assessing the morphology of the cartilaginous acetabulum (alpha angle) and the dynamic stability of the femoral head. In children older than 6 months, an anteroposterior (AP) and frog-leg lateral radiograph of the pelvis is required to assess the ossific nucleus, the acetabular index, and the integrity of Shenton's line.

The definitive decision to proceed with a medial open reduction is often made intraoperatively. The patient is placed supine on a radiolucent operating table to facilitate unimpeded fluoroscopic imaging. General anesthesia with complete muscle relaxation is mandatory. Both lower extremities are prepped and draped freely from the umbilicus to the toes to allow for symmetric evaluation of hip abduction and dynamic stability testing.
An examination under anesthesia (EUA) is performed first, followed by a closed reduction attempt. An intraoperative arthrogram is highly recommended. Contrast dye is injected into the hip joint, and fluoroscopy is utilized to assess the reduction. The presence of a "rose thorn" sign (dye pooling between the femoral head and the transverse acetabular ligament) or a persistent medial dye pool >5 mm indicates interposed tissue blocking a concentric reduction, thereby necessitating an open approach.
Detailed Surgical Approach and Technique
The medial approach offers direct access to the medial and inferior obstacles to reduction without violating the iliac apophysis or the abductor musculature, minimizing blood loss and postoperative stiffness. Several variations of the medial approach exist (Ludloff, Ferguson, Weinstein), but the fundamental principles remain consistent.
Incision and Superficial Dissection
The hip is positioned in flexion, abduction, and external rotation (the "frog-leg" position). A 3 to 4 cm transverse incision is made directly within the medial groin crease, centered over the palpable adductor longus tendon.

Subcutaneous tissues are sharply dissected, taking care to maintain hemostasis. The deep fascia is incised in line with the skin incision. The adductor longus is identified; a percutaneous or open adductor tenotomy is routinely performed at its tendinous origin on the pubis to relieve adductor contracture and expand the surgical field.

Deep Internervous Planes
The critical deep dissection involves identifying the interval between the pectineus muscle anteriorly and the adductor brevis/magnus complex posteriorly. Blunt dissection is utilized to develop this plane.

The pectineus is retracted anteriorly and superiorly. This maneuver inherently protects the anteriorly situated femoral neurovascular bundle. Deep within this interval, the lesser trochanter of the femur is palpated. The medial femoral circumflex artery (MFCA) must be meticulously identified and protected. It typically courses transversely across the operative field, deep to the pectineus but superficial to the iliopsoas. Gentle, blunt retraction is mandatory to avoid vasospasm or avulsion of the MFCA.
Iliopsoas Tenotomy and Capsulotomy
Once the lesser trochanter is exposed, the iliopsoas tendon is identified at its insertion. A right-angle clamp is passed deep to the tendinous portion of the iliopsoas, and a transverse tenotomy is performed. The underlying muscular portion may be left intact. Release of the iliopsoas eliminates the deforming force causing the capsular hourglass constriction.

With the iliopsoas released and retracted superiorly, the inferior aspect of the hip capsule is visualized. The capsule is sharply incised. A crucial technical point is to make the capsulotomy parallel to the acetabular labrum, remaining inferior to the equator of the femoral head to avoid inadvertent injury to the retinacular vessels supplying the epiphysis.

Intra Articular Dissection and Obstacle Clearance
Upon entering the joint, the hypertrophied ligamentum teres is immediately encountered. It is traced to its origin in the acetabular fossa and sharply excised. The fibrofatty pulvinar is then removed using a combination of pituitary rongeurs and a curette, exposing the medial wall of the acetabulum.

The transverse acetabular ligament (TAL) is identified spanning the inferior acetabular notch. A radial incision is made through the TAL to widen the inferior acetabulum, allowing the femoral head to seat deeply and medially. The superior labrum is inspected from within; if an inverted neolimbus is present, it is gently everted using a blunt dissector, taking care not to excise the labrum itself, as it is crucial for future acetabular development.
Reduction and Closure
With all mechanical blocks removed, the femoral head is gently reduced into the true acetabulum via flexion, abduction, and internal rotation. The reduction must be concentric and visually confirmed.

Fluoroscopy is utilized to confirm the depth of reduction and the restoration of Shenton's line. The hip is taken through a range of motion to establish the new "safe zone" of stability. Unlike the anterior approach, formal capsulorrhaphy is technically difficult and generally not performed in the medial approach. The capsule is left open or approximated loosely to prevent excessive intracapsular pressure, which can compromise epiphyseal perfusion. The surgical wound is copiously irrigated, and the subcutaneous tissues and skin are closed in layers using absorbable sutures.
Complications and Management
The medial approach is an exacting procedure, and deviations from meticulous surgical technique can result in profound complications. The most devastating complication is osteonecrosis (avascular necrosis) of the femoral head.

AVN is primarily caused by iatrogenic injury to the medial femoral circumflex artery during the deep dissection, or by excessive compression of the epiphyseal vessels due to extreme abduction (greater than 60 degrees) in the postoperative spica cast. Redislocation is another significant risk, usually stemming from incomplete removal of the pulvinar, failure to adequately release the transverse acetabular ligament, or improper molding of the spica cast.
| Complication | Estimated Incidence | Etiology | Prevention and Management Strategies |
|---|---|---|---|
| Avascular Necrosis (AVN) | 5% - 15% | MFCA injury, extreme cast abduction, high intracapsular pressure | Protect MFCA, cast in <50° abduction, avoid tight capsulorrhaphy. Management includes prolonged bracing or subsequent osteotomy for deformity. |
| Redislocation / Subluxation | 2% - 8% | Retained pulvinar, intact TAL, poor cast molding, inverted labrum | Complete clearance of acetabular fossa, radial cut of TAL, meticulous cast molding over greater trochanter. Requires revision open reduction. |
| Nerve Injury | < 1% | Aggressive retraction of femoral or obturator nerve | Gentle, blunt retraction. Avoid prolonged, heavy tension on retractors. Usually transient neuropraxia managed with observation. |
| Infection | 1% - 2% | Groin incision proximity to perineum, cast soiling | Preoperative antibiotics, meticulous skin closure, waterproof cast taping (petaling), caregiver education on cast hygiene. |
| Residual Dysplasia | 20% - 40% | Lack of capsulorrhaphy, older age at index surgery, intrinsic biology | Long-term radiographic follow-up. May require secondary pelvic osteotomy (e.g., Dega, Salter) if dysplasia persists >3-4 years of age. |
Post Operative Rehabilitation Protocols
Immediate postoperative immobilization is achieved with a one-and-a-half (1.5) hip spica cast applied in the operating room while the patient remains under general anesthesia. The position of immobilization is critical: the hips are placed in the "human position," consisting of 90 to 100 degrees of flexion and 40 to 50 degrees of abduction. Extreme abduction (the "frog-leg" position) must be strictly avoided to mitigate the risk of vascular occlusion and subsequent AVN.

The cast is meticulously molded over the posterior aspect of the greater trochanters to apply a gentle anteriorly directed force, maintaining the reduction. The initial spica cast is typically maintained for 6 weeks. Following this period, the child is returned to the operating room for a cast change under anesthesia. An arthrogram or MRI may be performed at this stage to confirm maintenance of the concentric reduction. A second spica cast is applied for an additional 6 weeks, bringing the total duration of rigid immobilization to 12 weeks.
Following cast removal, the infant is transitioned to an abduction orthosis (such as a Rhino Cruiser or Ilfeld splint). Initially, the brace is worn full-time (23 hours a day) for several weeks, gradually weaning to nap and nighttime wear until the acetabular index normalizes and the ossific nucleus is well-developed. Long-term radiographic surveillance is mandatory, typically continuing until skeletal maturity, to monitor for late-onset residual dysplasia or subtle manifestations of avascular necrosis.
Summary of Key Literature and Guidelines
The evolution of the medial approach is well-documented in orthopedic literature. Ludloff originally described the medial approach in 1913, advocating for access between the adductor longus and pectineus. Ferguson later modified the approach in 1973, utilizing the interval posterior to the adductor brevis to further protect the MFCA. Weinstein and Ponseti (1979) popularized the anteromedial approach, demonstrating excellent long-term outcomes with minimal AVN when strict adherence to the internervous planes and cast positioning was maintained.
Current academic guidelines and consensus statements emphasize that the medial approach is highly advantageous for the infant under 12 months of age due to its direct access to the pathology, minimal blood loss, and preservation of the abductor musculature and iliac apophysis. However, the literature universally cautions against its use in older toddlers due to the inability to perform a capsulorrhaphy or a concurrent pelvic osteotomy. Long-term outcome studies indicate that while the medial approach yields a high rate of successful initial reduction, up to one-third of patients may exhibit residual acetabular dysplasia requiring a secondary pelvic osteotomy later in childhood. Therefore, rigorous, protocol-driven radiographic follow-up remains the standard of care for all patients undergoing open reduction for developmental dysplasia of the hip.
Clinical & Radiographic Imaging
You Might Also Like