Management of the Rheumatoid Foot & Forefoot Arthroplasty
Key Takeaway
Surgical management of the rheumatoid foot requires a meticulous balance of biomechanical restoration and soft tissue handling. While conservative measures like semirigid orthoses and rocker-bottom shoes remain the first line of treatment, progressive deformity often necessitates surgical intervention. Forefoot arthroplasty and first metatarsophalangeal joint arthrodesis provide reliable pain relief and functional improvement, provided strict adherence to preoperative vascular assessment and precise surgical technique is maintained.
INTRODUCTION TO RHEUMATOID FOOT PATHOANATOMY
The management of the rheumatoid foot represents one of the most complex challenges in operative orthopaedics. Rheumatoid arthritis (RA) is a systemic autoimmune disease characterized by chronic synovial inflammation, which inevitably leads to capsular distension, ligamentous laxity, and progressive articular destruction. In the foot and ankle, this biomechanical derangement manifests as a predictable cascade of deformities.
In patients with rheumatoid arthritis, pain and swelling in the hindfoot and ankle have historically been correlated with severe limitation and disability—often more so than isolated pain and swelling of the forefoot. However, the duration of the disease and the subjective experience of pain influence the patient's overall disability far more than the objective radiographic damage.
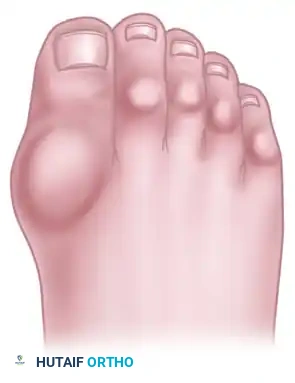
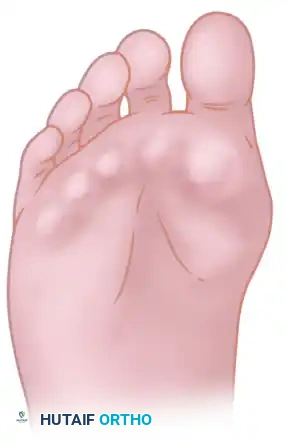
The classic "rheumatoid foot" presents with severe hallux valgus, dorsal subluxation or frank dislocation of the lesser metatarsophalangeal (MTP) joints, claw toes, hammer toes, and the formation of painful adventitial bursae. As the proximal phalanges subluxate dorsally, the plantar metatarsal fat pad is drawn distally, leaving the prominent metatarsal heads directly exposed to plantar pressure, leading to intractable plantar keratoses and ulceration.
CONSERVATIVE MANAGEMENT AND BIOMECHANICAL OPTIMIZATION
Conservative, nonoperative options must be exhausted before surgical treatment is entertained. Medical management should be rigorously optimized in all patients in coordination with a rheumatologist. Despite the advent of disease-modifying antirheumatic drugs (DMARDs) and biologic therapies, foot pain remains a common and disabling complaint. Unfortunately, rheumatologists are statistically less likely to examine patients’ feet than their hands, making the orthopaedic surgeon's role critical in early diagnosis and intervention.
Interestingly, conservative treatment is often more effective for forefoot disease than for hindfoot or ankle pathology. Patients with rheumatoid arthritis have been found to possess an altered "plantar pressure pain threshold," demonstrating decreased plantar foot sensitivity in all regions compared to healthy control groups.
Clinical Pearl: Because of this decreased sensitivity, pedobarography (plantar pressure mapping) is highly recommended early in the disease process. It allows the clinician to identify and correct excessive plantar loading before symptoms become severe or ulcerations develop.
Orthotics and Footwear Modifications
Initially, patients should be managed with extra-deep shoes featuring a wide, high toe-box to accommodate dorsal toe deformities.

Key conservative modalities include:
* Molded Inserts: Custom total-contact inserts distribute weight away from bony prominences.
* Semirigid Orthoses: Evidence suggests that semirigid orthoses are significantly more effective than soft, accommodative orthoses in controlling biomechanical forces. Early utilization is strongly recommended.
* Rocker Soles and Steel Shanks: These modifications help relieve midfoot pain by bypassing the propulsive phase of gait, thereby counteracting midfoot and forefoot stiffness.
* Ancillary Padding: Toe sleeves, silicone spacers, corn pads, and routine podiatric débridement of plantar callosities provide symptomatic relief.

If the tibiotalar (ankle) joint or hindfoot is involved, a double upright brace with a limited-motion or locked ankle joint, combined with an inside (valgus-correcting) T-strap, may aid in nonoperative management.
While these treatments can be used indefinitely, surgery is usually required due to continued pain, progressive deformity, and patient dissatisfaction with unattractive, bulky footwear that requires frequent modifications.
PREOPERATIVE EVALUATION AND AVOIDING COMPLICATIONS
The complication rate in rheumatoid foot surgery is historically high (approximately 32%), emphasizing the absolute necessity for meticulous preoperative planning and patient education. Complications can be minimized if the following strict protocols are observed:
1. Vascular Assessment
Careful attention must be paid to the presence and intensity of pedal pulses. If asymmetry exists, a peripheral vascular consultation is mandatory.
* Objective Parameters: In nondiabetic patients with rheumatoid arthritis, an absolute ankle pressure of $\ge$ 90 mm Hg, or an Ankle-Brachial Index (ABI) of $\ge$ 0.7, is generally required to ensure forefoot wound healing in 90% of patients.
2. Dermatologic and Neurologic Inspection
The skin of the foot and distal leg must be inspected for rheumatoid vasculitis, which presents as non-blanching macules and papules (often over the anterolateral distal tibia and dorsolateral foot), occasionally with a necrotic preulcerative center.
* Rheumatoid Nodules: Caused by vasculitis of the subcutaneous connective tissue.
* Mononeuritis Multiplex: An immune complex–mediated vasculitis of the peripheral nerves. Patients presenting with hyperesthesia (distinct from joint synovitis pain) must be examined for sensory, motor, or mixed deficits. If vasculitis is suspected, a rheumatology consult or skin biopsy is warranted prior to any surgical intervention.
3. Perioperative Medication Management
While studies have shown that the perioperative use of methotrexate, gold salts, NSAIDs, or hydroxychloroquine does not significantly increase the risk of healing or infectious complications, corticosteroid use requires specific protocol adjustments.
Surgical Warning: If a patient is taking systemic corticosteroids, the tensile strength of the healing skin is severely compromised. Suture removal must be delayed to 3 weeks (21 days) or longer, rather than the customary 12 to 16 days, to prevent catastrophic wound dehiscence.
4. Infection Prophylaxis and Skin Preparation
- Skin Prep: Meticulously clean the skin, especially between the toes and around the nail folds, for 10 to 15 minutes before surgery, followed by a sterile wrap. This is repeated in the operating room to reduce scrub time.
- Antibiotics: Routine use of a prophylactic broad-spectrum antibiotic is required 30 minutes prior to incision, intraoperatively, and for 48 to 72 hours postoperatively.
- Postoperative Care: Elevate the feet to the maximal tolerable level for 48 to 72 hours postoperatively to mitigate severe edema.

SURGICAL DECISION MAKING AND PATIENT COUNSELING
Before forefoot arthroplasty is recommended, the surgeon must engage in frank, documented counseling with the patient. The patient must understand that rheumatoid arthritis is a progressive, systemic disease. Therefore, surgical correction of the deformity should be considered palliative rather than definitive or curative.
If both the patient and physician enter surgical management with this realistic perspective, the functional and subjective outcomes are highly rewarding, provided unexpected complications do not arise.
FOREFOOT ARTHROPLASTY: PRINCIPLES AND TECHNIQUES
Forefoot arthroplasty is directed primarily at the severe metatarsophalangeal joint deformities. The overarching goals are to relieve pain, correct deformity, improve cosmesis, enhance ambulatory function, and allow the patient to wear a reasonable variety of footwear.
The Importance of Adequate Bone Resection
Regardless of the specific surgical approach (plantar vs. dorsal incisions), adequate bony resection is mandatory. The phalanges must be allowed to realign loosely with the metatarsal remnants without any soft tissue tension. Insufficient relaxation of the soft tissues around the MTP joints due to inadequate bone resection will severely compromise the result, leading to recurrent dorsal subluxation and stiffness.


The Metatarsal Cascade
When performing a resection arthroplasty, the surgeon must carefully contour the remaining metatarsal necks. Unequal lengths of the metatarsal remnants, or metatarsals that do not cascade in a gentle, parabolic curve from metatarsals two through five, will result in transfer metatarsalgia and a compromised outcome. Furthermore, any bony fragments left in the forefoot weight-bearing pad will act as symptomatic pebbles, causing severe localized pain.


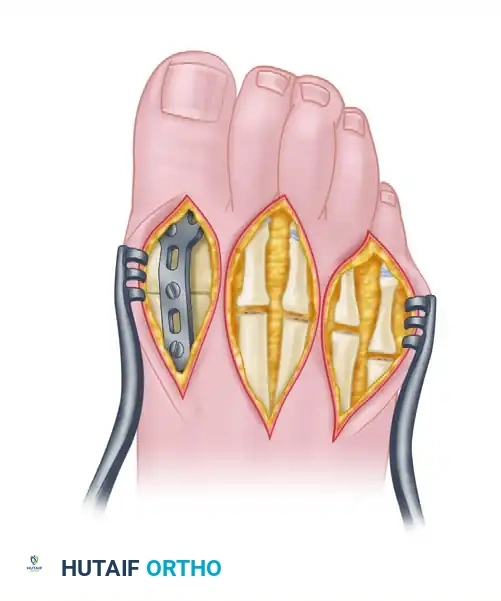
Surgical Options for the Lesser Rays
Resection of all five metatarsal heads, or fusion of the first MTP joint combined with resection of metatarsals 2 through 5, have both been shown to produce excellent results. All four of the lesser toes must be treated in the same manner, regardless of the varying severity of involvement of each individual ray. While there are rare exceptions where only one or two lesser metatarsal heads are removed, the patient must be warned that subsequent surgeries to remove the remaining heads are highly likely as the disease progresses.

Note: Early results of silicone-rubber, single-stem replacement arthroplasty were initially satisfactory, but severe concerns regarding silicone synovitis and particulate debris have rendered this procedure largely obsolete. Hemiarthroplasty should be performed with extreme caution as long-term survivorship data remains lacking.
ARTHRODESIS OF THE FIRST METATARSOPHALANGEAL JOINT
For the rheumatoid hallux, arthrodesis of the first MTP joint, combined with varying degrees of bony shortening/resection at the lesser MTP joints, is the gold standard. This approach yields satisfactory results in 80% to 90% of patients.

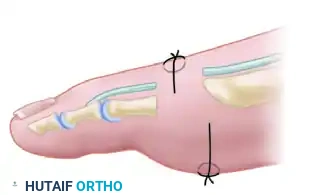
Biomechanical Positioning for Arthrodesis
The success of a first MTP fusion relies entirely on precise spatial positioning. Improper alignment will lead to gait dysfunction, interphalangeal joint arthritis, and transfer lesions.
* Valgus Alignment: Approximately 20 degrees of valgus.
* Dorsiflexion: 30 degrees of dorsiflexion in reference to the first metatarsal axis. (This equates to approximately 15 degrees of dorsiflexion in reference to the plantar aspect of the foot).
* Rotation: The hallux must be placed in absolute neutral rotation.
This specific alignment allows for a normal toe-off during the terminal stance phase of gait and accommodates a standard shoe heel height. Excellent gait patterns and improved first-second intermetatarsal angles are routinely achieved. Rarely is a proximal first metatarsal osteotomy necessary in conjunction with the arthrodesis.
Arthrodesis vs. Excisional Arthroplasty
Comparisons between first MTP arthrodesis and excisional arthroplasty (e.g., Keller procedure) heavily favor arthrodesis. Arthrodesis provides superior pain relief, better dynamic balance, improved cosmesis, and a greater ability to fit the foot into a normal shoe.
While one older study suggested patient satisfaction was lower after arthrodesis despite better objective foot function, modern prospective, randomized studies (such as Grondal et al.) comparing first MTP arthrodesis to first metatarsal head resection found no significant difference in deformity recurrence, lateral forefoot pressure, or patient satisfaction. However, given the small sample sizes in these studies, the consensus among master surgeons remains that even with a well-preserved hallux MTP joint, fusion is a more definitive and satisfactory procedure than attempts at joint preservation in the rheumatoid patient.

LONG-TERM OUTCOMES AND PROGNOSIS
From a comprehensive review of published series on forefoot arthroplasty, several definitive conclusions emerge:
- High Initial Success: In 80% to 90% of patients, a highly satisfactory result can be expected in the short to medium term. Pain relief, walking endurance, and footwear variety are significantly improved.
- Surgical Precision is Key: The location of the incision (plantar vs. dorsal) is less important than delicate soft-tissue handling, meticulous hemostasis, and the creation of a smooth metatarsal cascade.
- Inevitable Deterioration: After 3 to 5 years, the percentage of excellent results begins to decrease. Objective measures—such as the recurrence of hallux valgus, recurrent plantar callosities, dorsal posturing of the toes on the metatarsal remnants, and new bony proliferation on the distal metatarsals—often become apparent.
- Subjective vs. Objective Disconnect: Interestingly, although deformity has been reported to recur in more than 50% of patients over time, up to 97% of patients remain subjectively satisfied with their results. This discrepancy is likely because many rheumatoid patients gradually reduce their overall level of physical activity due to the generalized, systemic nature of the disease, rendering the recurrent foot deformities less symptomatic than they would be in a highly active individual.
In conclusion, surgical reconstruction of the rheumatoid forefoot is a highly effective, albeit palliative, intervention. By adhering to strict preoperative optimization, respecting the fragile soft-tissue envelope, and executing precise bony resections and fusions, the orthopaedic
You Might Also Like