Tarsometatarsal Interpositional Arthroplasty: Surgical Guide
Key Takeaway
Tarsometatarsal interpositional arthroplasty is a joint-sparing procedure designed to preserve the essential mobility of the lateral column, specifically the articulation of the cuboid with the fourth and fifth metatarsals. By utilizing either a soft tissue "anchovy" or a spherical ceramic implant, surgeons can alleviate pain while preventing the stress fractures and hardware failures commonly associated with rigid lateral column fusions.
INTRODUCTION AND BIOMECHANICAL RATIONALE
Tarsometatarsal interpositional arthroplasty is a highly specialized, joint-sparing surgical intervention primarily targeting the lateral column of the foot—specifically the articulations between the cuboid and the fourth and fifth metatarsals. In the realm of midfoot reconstruction, understanding the distinct biomechanical roles of the medial, middle, and lateral columns is paramount.
The medial and middle columns (comprising the first, second, and third tarsometatarsal joints) are inherently rigid, functioning as a stable lever arm essential for the push-off phase of the gait cycle. Conversely, the lateral column is highly mobile. This mobility allows the foot to accommodate uneven terrain and acts as a critical shock absorber during the stance phase of gait.
If possible, the articulation of the cuboid with the fourth and fifth metatarsals should be spared from arthrodesis. Iatrogenic stiffness in these naturally mobile joints frequently leads to severe biomechanical complications, including adjacent joint arthritis, stress fractures of the metatarsals, and catastrophic hardware failure. While some historical literature reports acceptable results with lateral column fusion, contemporary orthopedic consensus strongly advocates for motion preservation. Tarsometatarsal interpositional arthroplasty achieves this by replacing the arthritic joint surfaces with either an autologous soft-tissue "anchovy" or a spherical ceramic implant, thereby maintaining lateral column compliance while effectively eradicating pain.
Clinical Pearl: Tarsometatarsal interpositional arthroplasty is rarely performed in isolation. It is most frequently executed in conjunction with rigid arthrodesis of the medial and middle columns to address global midfoot arthritis while preserving lateral flexibility.
INDICATIONS AND CONTRAINDICATIONS
Indications
- Primary Osteoarthritis: Symptomatic degeneration of the 4th and/or 5th tarsometatarsal joints refractory to conservative management (e.g., orthotics, NSAIDs, corticosteroid injections).
- Post-Traumatic Arthritis: Degeneration secondary to previous Lisfranc injuries or cuboid fractures.
- Rheumatoid Arthritis: Inflammatory arthropathy affecting the midfoot, where preserving lateral motion can significantly improve gait mechanics.
- Combined Midfoot Degeneration: As an adjunct to medial and middle column arthrodesis to prevent a completely rigid, non-compliant foot.
Contraindications
- Neuropathic Arthropathy (Charcot Foot): In cases of profound neuropathy and structural collapse, stability supersedes motion. Fusion of the lateral column is acceptable and often required to prevent progressive deformity.
- Active Infection: Absolute contraindication for any joint arthroplasty or implantation of foreign material.
- Severe Bone Loss: Inadequate bone stock in the cuboid or metatarsal bases that would preclude the stable seating of a ceramic implant.
- Uncorrectable Hindfoot Deformity: Significant malalignment must be addressed concurrently or prior to midfoot arthroplasty to prevent eccentric loading and premature implant failure.
PREOPERATIVE PLANNING AND IMPLANT SELECTION
Standard weight-bearing anteroposterior, lateral, and oblique radiographs of the foot are mandatory. A computed tomography (CT) scan is highly recommended to accurately assess bone stock, the extent of osteophyte formation, and the presence of subchondral cysts that might compromise implant seating.
Arthroplasty has been described using either a soft tissue “anchovy” (typically utilizing the peroneus tertius or a slip of the extensor digitorum longus from the fourth digit) or a spherical ceramic implant (e.g., Orthosphere, Wright Manufacturing, Memphis, TN). Clinical outcomes and survivorship data demonstrate that results are generally superior with the ceramic implant, as it maintains joint space height more reliably than soft tissue, which is prone to subsidence and scarring. However, the exact amount of motion retained after this procedure remains challenging to quantify biomechanically.
ANESTHESIA AND PATIENT POSITIONING
- Anesthesia: The procedure is typically performed under general anesthesia or a robust spinal block.
- Regional Block: Administration of a popliteal sciatic nerve block (often combined with a saphenous nerve block) is highly recommended for optimal postoperative pain control and to reduce the requirement for systemic opioids.
- Positioning: Place the patient supine on the operating table. A bump placed under the ipsilateral hip is crucial; it internally rotates the lower extremity, bringing the lateral aspect of the foot into a direct, accessible view. Alternatively, a semilateral position utilizing a beanbag can be employed.
- Tourniquet: Apply a well-padded thigh or calf tourniquet to ensure a bloodless surgical field. Exsanguinate the limb and inflate the tourniquet prior to incision.
SURGICAL TECHNIQUE: STEP-BY-STEP
1. Surgical Approach and Exposure
Make a longitudinal dorsolateral incision directly in line with the medial aspect of the fifth metatarsal joint. This incision allows access to both the 4th and 5th tarsometatarsal joints.
Surgical Warning: Meticulous superficial dissection is critical. Take extreme care to identify, mobilize, and protect the intermediate dorsal cutaneous branch of the superficial peroneal nerve medially, and the sural nerve laterally. Neuroma formation in this region is a debilitating complication.
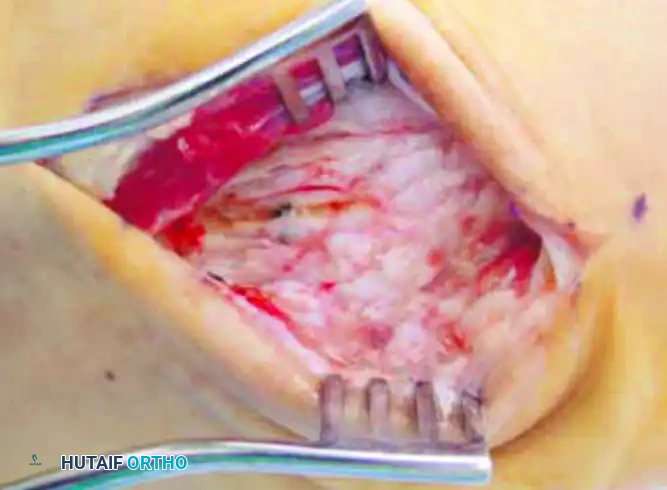
Deepen the incision through the subcutaneous tissues. Identify and retract the extensor tendons (extensor digitorum longus and peroneus tertius) medially or laterally as dictated by the exposure needs. Expose the tarsometatarsal joint capsule and create full-thickness subperiosteal flaps to expose the dorsal articular margins.
2. Joint Preparation and Synovectomy
Once adequate exposure is achieved, aggressively débride any dorsal, medial, and lateral osteophytes. Osteophyte excision is not merely for visualization; it is a critical step in restoring the mechanical block to motion. Perform a thorough synovectomy to remove inflamed tissue.
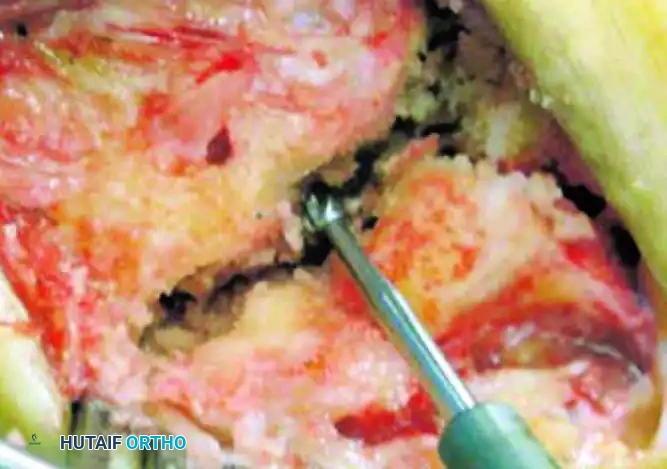
3. Pilot Hole Creation
Using a small round burr, create a precise center pilot hole in the opposing joint surfaces of the lateral metatarsal-cuboid joint.
Clinical Pearl: When burring, it is imperative to preserve the peripheral cortical rim and the robust plantar ligaments. The plantar ligamentous complex is the primary stabilizer of the midfoot; violating it will lead to dorsal subluxation of the metatarsal and catastrophic implant dislocation.
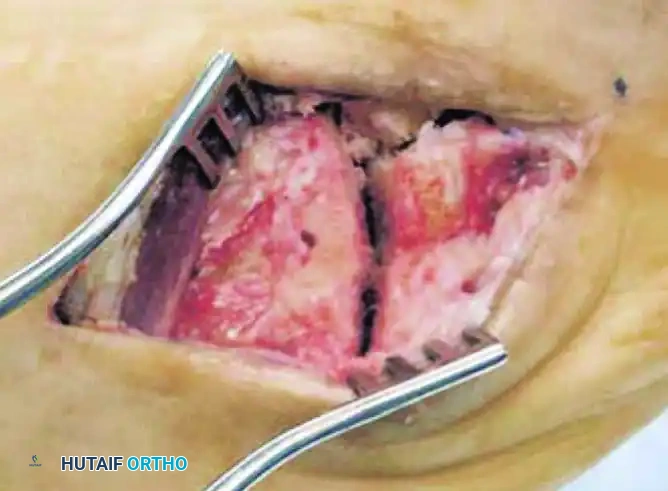
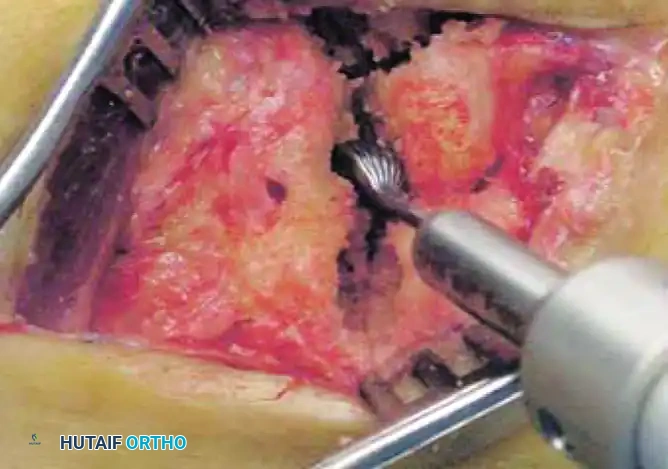
4. Hemispherical Reaming
Following the creation of the pilot hole, utilize specialized hemispherical power burrs to create matching hemispherical recesses on both sides of the joint (the base of the metatarsal and the distal articular surface of the cuboid). The reaming should be done sequentially, ensuring the recess is perfectly centered and deep enough to capture the implant without breaching the plantar cortex.
5. Trialing and Sizing
Insert a trial sizing tool into the prepared joint space. The goal is to select a size that provides stability and maintains the anatomical length of the lateral column without overstuffing the joint, which could lead to stiffness or adjacent joint subluxation.
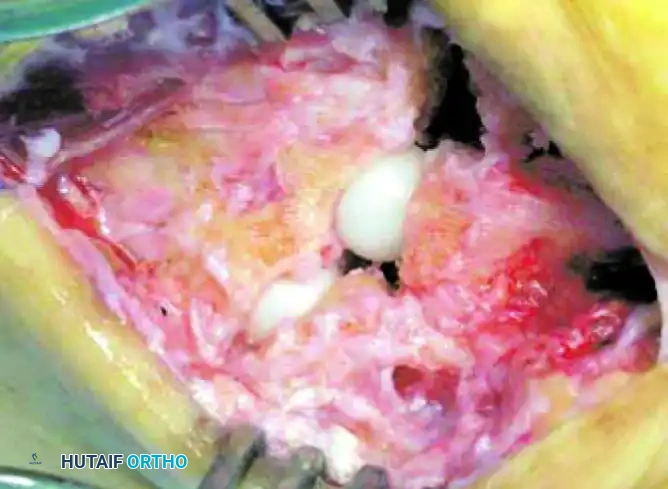
6. Implant Insertion
Once the optimal size has been determined, prepare the final implant. If utilizing a biological interposition, harvest the peroneus tertius or a slip of the extensor digitorum longus from the fourth digit, roll it into an “anchovy” fashion, and secure it with absorbable suture.
If utilizing the preferred spherical ceramic implant, select the corresponding size. To insert the implant, apply longitudinal traction and forcefully plantarflex the metatarsal. This maneuver opens the joint dorsally, allowing the sphere to be seated deep within the recessed cavity without damaging the dorsal cortical rim.

7. Verification and Closure
Release the traction and allow the joint to rest. Verify the stability of the joint through a full range of motion. The implant should remain deeply seated and stable during simulated weight-bearing and sagittal motion. Confirm the position and sizing with intraoperative fluoroscopy.
Deflate the tourniquet and obtain meticulous hemostasis. Copiously irrigate the wound with sterile saline to remove any bone debris generated during reaming. Close the joint capsule (if possible), the extensor retinaculum, and the subcutaneous tissue in a standard layered fashion. Close the skin with non-absorbable sutures or staples. Apply a sterile, bulky soft fluff dressing and a posterior splint in neutral dorsiflexion.
POSTOPERATIVE CARE AND REHABILITATION PROTOCOL
Postoperative immobilization and weight-bearing status are heavily dictated by whether the procedure was performed in isolation or combined with other midfoot reconstructions.
Isolated Lateral Column Arthroplasty
If the tarsometatarsal interpositional arthroplasty was performed as an isolated procedure:
* Weeks 0-2: The patient is placed in a bulky splint and kept strictly non–weight bearing. Elevation is critical to manage edema and protect the incision.
* Weeks 2-6: At the 2-week mark, if the wound is fully healed, sutures are removed. The patient is transitioned into a controlled ankle motion (CAM) boot walker. Weight-bearing is progressively advanced as tolerated.
* Week 6 and Beyond: The patient is transitioned from the boot to a supportive, wide toe-box shoe equipped with a rigid carbon fiber insert to limit excessive stress across the midfoot during the final phases of soft tissue healing. Physical therapy is initiated to restore gait mechanics and proprioception.
Combined Procedures (Medial/Middle Column Fusion)
If the arthroplasty was performed in conjunction with a medial and/or middle column arthrodesis (which is the most common clinical scenario):
* Weeks 0-8/10: The rehabilitation timeline is entirely dictated by the fusion sites. The patient must remain strictly non-weight bearing in a cast or rigid boot until definitive radiographic union of the arthrodesis sites is observed.
* Weeks 8-12: Once radiographic union is confirmed (typically at 8 to 10 weeks), progressive weight-bearing in a CAM boot is initiated, followed by a transition to stiff-soled footwear.
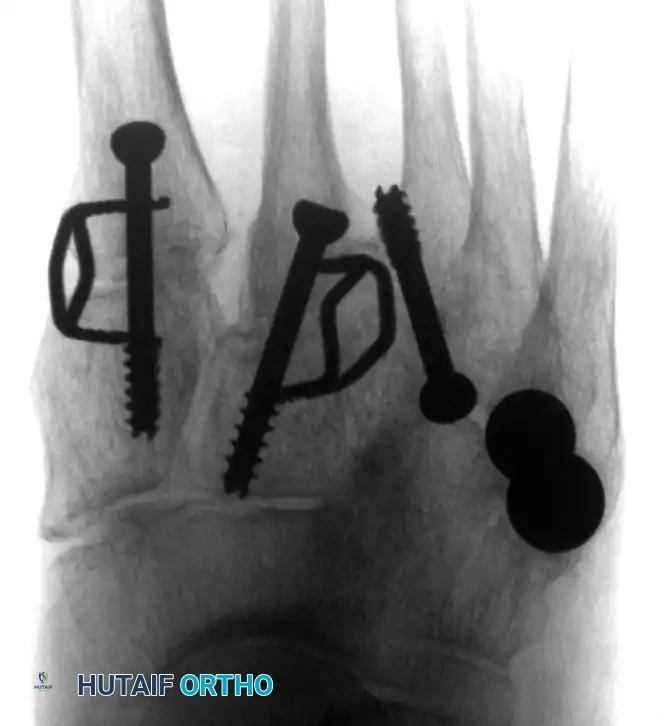

(Above: Anteroposterior and oblique radiographic appearance 10 months after a combined medial/middle column fusion with lateral tarsometatarsal ceramic interpositional arthroplasty. Note the preservation of the lateral joint space and stable seating of the spherical implants.)
COMPLICATIONS AND MANAGEMENT
While highly effective, tarsometatarsal interpositional arthroplasty carries specific risks:
1. Implant Subsidence or Dislocation: Usually secondary to over-reaming, violation of the plantar cortical hinge, or premature weight-bearing. Revision may require conversion to a fusion or a larger implant.
2. Nerve Injury: Damage to the sural or superficial peroneal nerves can lead to painful neuromas. Prevention through meticulous surgical technique is paramount.
3. Persistent Pain: May occur if the implant is improperly sized (overstuffing the joint) or if there is unrecognized pathology in adjacent joints.
4. Infection: Managed with standard protocols, which may necessitate implant removal and placement of an antibiotic spacer.
By adhering to strict indications, respecting the complex biomechanics of the lateral column, and executing precise surgical technique, orthopedic surgeons can utilize tarsometatarsal interpositional arthroplasty to provide durable pain relief while preserving essential foot mobility.
You Might Also Like